Page 2 of 19
PA30.{1,4} | Benign Breast Disease & Gynecomastia — SDL Guide (Part 2)
Fibrocystic Change — Classification and Carcinoma Risk
Fibrocystic change (FCC) is an umbrella term for a spectrum of histological findings that represent exaggerated or aberrant responses to cyclic hormonal stimulation. It is the commonest breast condition in women aged 25–50.
Clinical presentation: Bilateral, diffuse, lumpy, tender breasts — worst premenstrually. Multiple small cysts palpable or visible on ultrasound ('blue dome cysts' grossly).
Classification by carcinoma risk (Page & Dupont, 1985):
| Category | Histological findings | Relative cancer risk |
|---|---|---|
| Non-proliferative | Cysts, apocrine metaplasia, mild fibrosis, adenosis | No increased risk (1×) |
| Proliferative without atypia | Epithelial hyperplasia (>2 cell layers), sclerosing adenosis, papillomatosis | 1.5–2× baseline |
| Proliferative with atypia | Atypical ductal hyperplasia (ADH) or atypical lobular hyperplasia (ALH) | 4–5× baseline |
| ADH/ALH + family history | As above + first-degree relative with breast cancer | 8–10× baseline |
Key histological components:
- Cysts — distended TDLUs; lined by flattened or apocrine epithelium ('blue dome' appearance grossly because thin wall makes blood vessels visible)
- Apocrine metaplasia — eosinophilic granular cytoplasm, prominent nucleoli; always benign
- Adenosis — increased number of acini per lobule; normal if no distortion
- Sclerosing adenosis — lobulocentric proliferation of acini and myoepithelial cells with fibrosis; mimics carcinoma microscopically but myoepithelial cells are preserved (use SMA immunostain to confirm)
- Epithelial hyperplasia — more than 2 cell layers lining ducts; when mild/moderate, benign; when marked, raises risk
- ADH — partial involvement of a duct space by cells resembling low-grade DCIS; quantitatively less or qualitatively incomplete
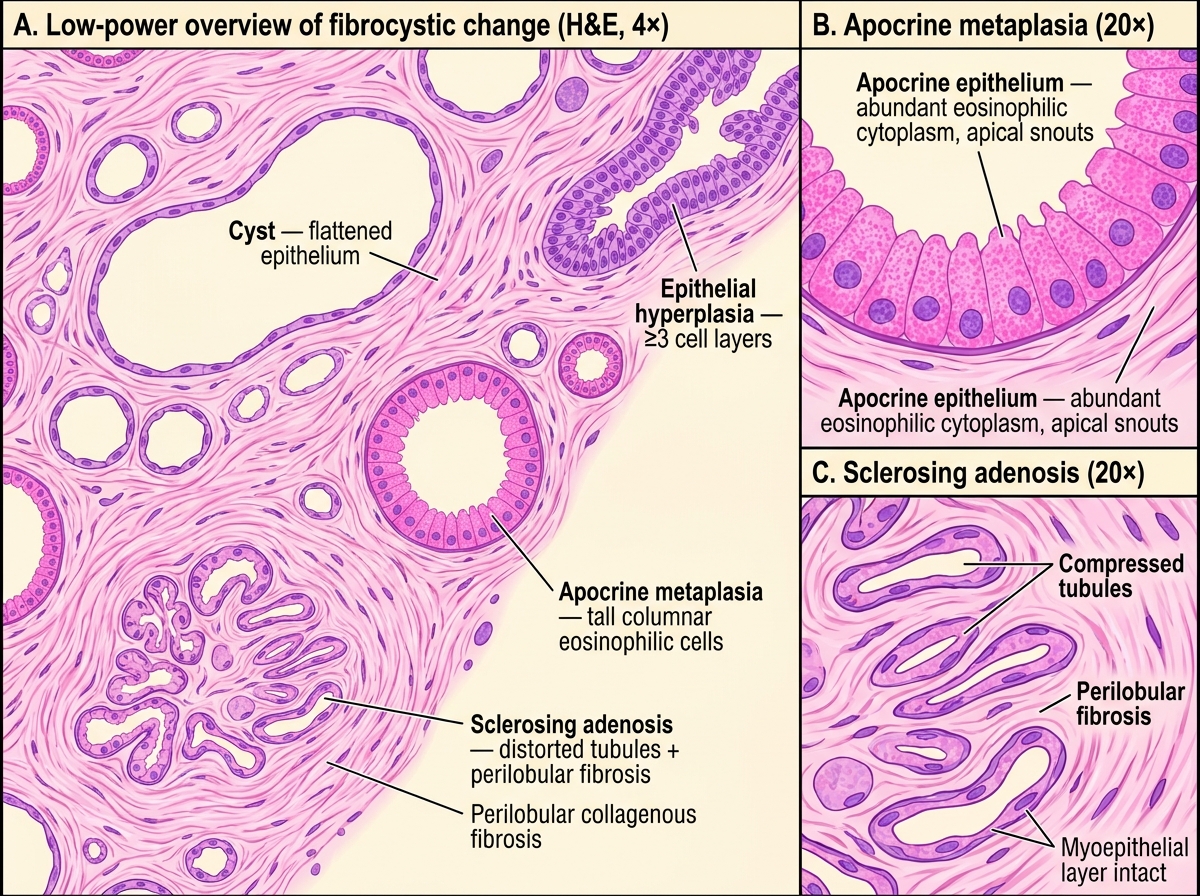
Histology of Fibrocystic Change — Low-Power Overview with High-Power Details
SELF-CHECK
A 40-year-old woman undergoes excision biopsy of a breast lump. Histology shows multiple cysts lined by apocrine epithelium, areas of sclerosing adenosis, and a focus where a duct is lined by 4–5 layers of cells without cytological atypia. What is her approximate relative risk of developing breast carcinoma compared to the general population?
A. No increased risk (1×)
B. 1.5–2× baseline
C. 4–5× baseline
D. 8–10× baseline
Reveal Answer
Answer: B. 1.5–2× baseline
The finding of epithelial hyperplasia of more than 2 cell layers without atypia places this patient in the 'proliferative without atypia' category, which carries a 1.5–2× relative risk. Risk escalates to 4–5× only when atypical ductal or lobular hyperplasia is present, and to 8–10× when atypia is combined with a first-degree family history.
Fibroadenoma — The Commonest Benign Breast Tumor
Fibroadenoma is the most common benign tumor of the breast, occurring predominantly in women aged 15–35 years.
Hormonal dependence:
Fibroadenomas arise from the intralobular stroma and are estrogen-sensitive. They grow during pregnancy and the luteal phase, and regress after menopause (often calcifying). Oral contraceptive pill (OCP) use is associated with slightly larger lesions but not malignant transformation.
Gross appearance:
• Well-circumscribed, encapsulated, rubbery/firm, mobile ('breast mouse')
• Cut surface — grey-white, whorled, may show cleft-like spaces
• Size: typically 1–3 cm (giant fibroadenoma >5 cm, especially in adolescents)
Microscopic appearance:
Biphasic proliferation of stromal and epithelial components.
Two growth patterns (both may coexist):
1. Intracanalicular — stroma proliferates and compresses ducts into curved, slit-like ('antler-horn') spaces. Stroma is the dominant component.
2. Pericanalicular — stroma proliferates around duct spaces that remain open and round.
Key microscopic features:
• Myoepithelial cell layer intact (confirms benignity)
• Stroma is loose, myxoid, paucicellular — NOT the hypercellular stroma of phyllodes tumor
• Epithelium shows no atypia
Malignant potential: Very low (<0.3% lifetime risk of malignancy within the lesion). Complex fibroadenomas (with cysts >3 mm, sclerosing adenosis, epithelial calcification, or papillary apocrine change) carry a slightly higher risk (2× baseline).
Differential from phyllodes tumor: Phyllodes has a hypercellular, mitotically active stroma with leaf-like projections ('phyllodes' = leaf). Stromal cellularity and mitotic count determine benign vs. borderline vs. malignant phyllodes.
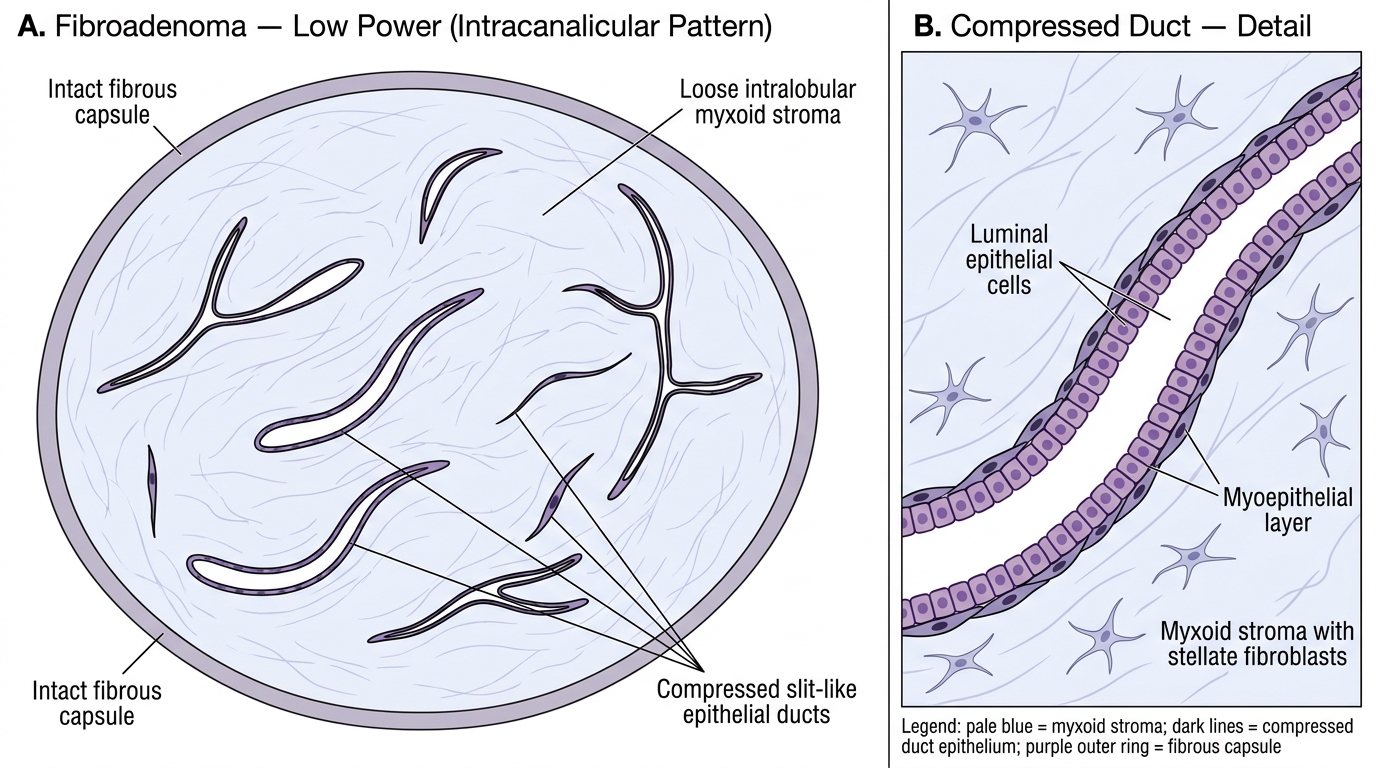
Intracanalicular Fibroadenoma — Low-Power Histological Pattern
CLINICAL PEARL
Fibroadenoma vs. phyllodes — why it matters clinically:
Both present as mobile breast lumps, but:
• Fibroadenoma → excision and discharge (no malignant potential at the population level)
• Phyllodes → wide local excision with 1 cm margins (even 'benign' phyllodes recurs locally; malignant phyllodes can metastasise haematogenously)
The only reliable distinguishing test is histology. Clinically, rapid growth, large size (>3 cm), and age >35 suggest phyllodes. FNA cytology can be misleading — it shows bland epithelial cells in both. Core biopsy (showing stromal architecture) is the diagnostic key.
Intraductal Papilloma
Intraductal papilloma is a benign epithelial tumor arising within a large or intermediate-sized duct. It is the commonest cause of bloody (haemoserous) nipple discharge in women of reproductive age.
Types:
| Feature | Solitary (central) | Multiple (peripheral) |
|---|---|---|
| Location | Large subareolar ducts | Smaller peripheral ducts / TDLU |
| Presentation | Nipple discharge, small subareolar lump | Incidental finding or diffuse lumps |
| Cancer risk | No significant increased risk | Slightly increased (especially if ADH present) |
Pathogenesis: Papillary fronds of fibrovascular cores lined by luminal epithelial and myoepithelial cells grow into a dilated duct. The duct becomes distended → discharge from the nipple.
Morphology:
• Grossly — soft friable wart-like growth within a dilated duct; cystic duct wall may contain blood-stained fluid
• Microscopically — branching fibrovascular cores lined by two cell layers: inner luminal cells (may show apocrine metaplasia) and outer myoepithelial cells
Distinguishing from papillary carcinoma:
• Benign papilloma: two cell layers (luminal + myoepithelial) present; no nuclear atypia; fibrovascular cores present
• Papillary carcinoma: loss of myoepithelial layer; nuclear atypia; may show cribriform or solid areas
• Immunostain for myoepithelial markers (p63, smooth muscle actin, calponin) is the definitive discriminator
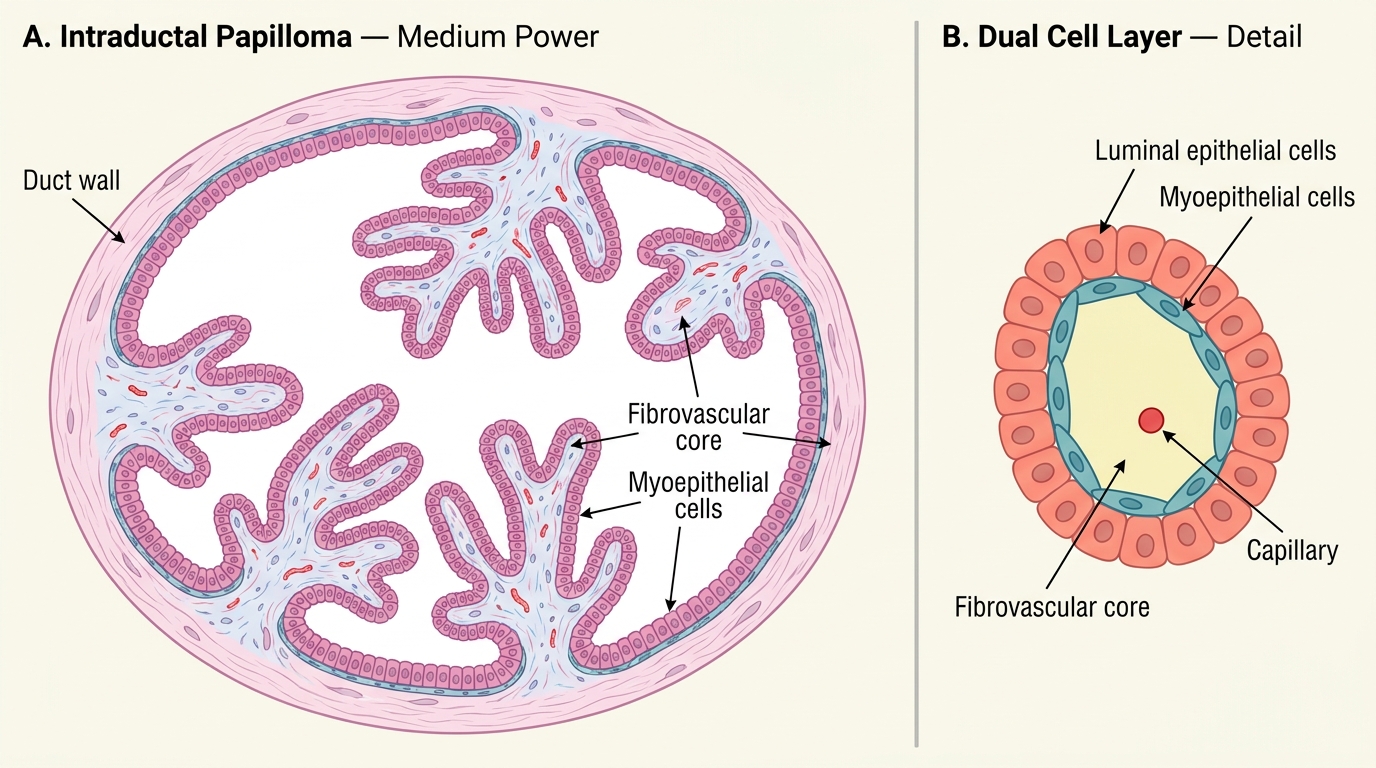
Histology of Intraductal Papilloma (Medium Power)