Page 3 of 19
PA30.{1,4} | Benign Breast Disease & Gynecomastia — SDL Guide (Part 3)
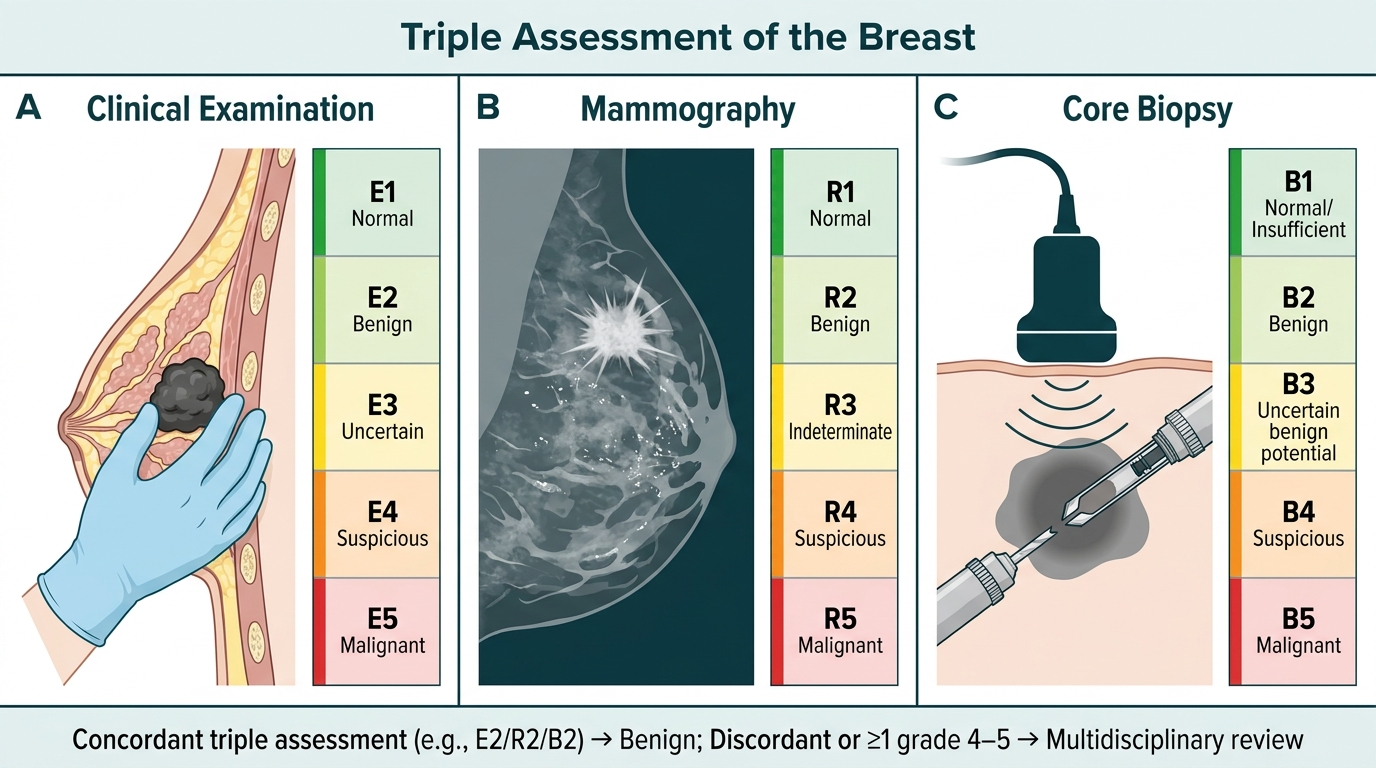
Triple Assessment — The Clinical Framework
Triple assessment is the gold-standard approach to evaluating any breast lump. It integrates three independent investigations, each graded 1–5 (1 = normal, 2 = benign, 3 = equivocal, 4 = suspicious, 5 = malignant).
The three components:
| Component | Method | What it detects |
|---|---|---|
| 1. Clinical examination | History + physical | Mass characteristics, lymph nodes |
| 2. Radiological | Mammography (>35 yrs) / Ultrasound (<35 yrs or pregnancy) | Density, calcification, margins |
| 3. Pathological | FNAC (cytology) or core needle biopsy (histology) | Cellular atypia, architecture |
Why 'triple'?: Each modality has its own false-negative rate:
• Clinical alone: misses 10–20% of cancers
• Imaging alone: misses 10–15%
• FNAC alone: misses 5–10%; cannot distinguish DCIS from invasive
• Triple concordance (all benign): sensitivity for malignancy >99.6%
Which benign lesions require ongoing surveillance?
| Lesion | Surveillance needed? |
|---|---|
| Non-proliferative FCC | No |
| Fibroadenoma (simple) | No (may observe if <2 cm, patient young) |
| Proliferative FCC without atypia | Annual clinical exam |
| ADH / ALH | Annual mammogram; consider chemoprevention |
| Lobular carcinoma in situ (LCIS) | High risk; consider bilateral surveillance/prophylaxis |
LCIS is no longer classified as truly 'benign' — it is a risk indicator and non-obligate precursor.
Triple Assessment of Breast Disease: Clinical, Radiological, and Pathological Grading
SELF-CHECK
A 38-year-old woman presents with bloody nipple discharge from the right nipple. No palpable lump. Ultrasound shows a 7 mm hypoechoic lesion in the subareolar region. Core biopsy shows branching papillary fronds with fibrovascular cores lined by two cell layers — an inner layer of cuboidal cells and an outer flattened layer. p63 immunostain highlights the outer layer. What is the most likely diagnosis and the key diagnostic feature that confirms benignity?
A. Intraductal papilloma — presence of myoepithelial cells (p63 positive outer layer)
B. Papillary carcinoma — loss of myoepithelial cells
C. Fibroadenoma — biphasic stroma and epithelium
D. Sclerosing adenosis — preserved lobular architecture
Reveal Answer
Answer: A. Intraductal papilloma — presence of myoepithelial cells (p63 positive outer layer)
The bilateral cell layer (luminal epithelial + myoepithelial) is the defining feature of a benign intraductal papilloma. p63 is a nuclear marker of myoepithelial cells. Its presence confirms the outer cell layer is myoepithelial, ruling out papillary carcinoma, which characteristically lacks myoepithelial cells. The presentation of bloody nipple discharge in a premenopausal woman with a small subareolar lesion is the classic scenario for a solitary (central) intraductal papilloma.
Gynecomastia — Etiology and Estrogen/Androgen Imbalance
Gynecomastia is the benign proliferation of male breast glandular tissue. It is distinguished from pseudogynecomastia (fat deposition without glandular proliferation) by histology or the feel of a rubbery retroareolar disc on examination.
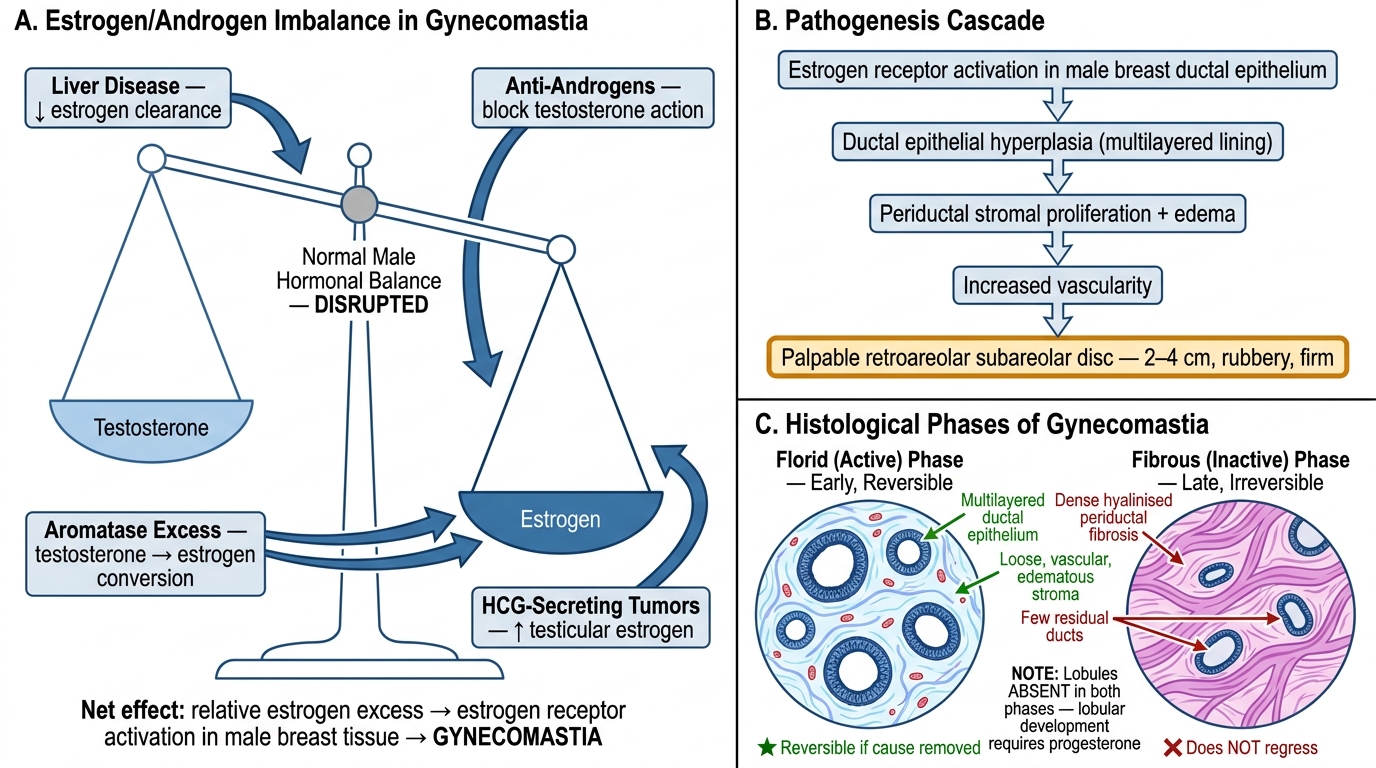
The central mechanism: altered estrogen/androgen (E/A) ratio
Breast tissue responds to estrogen (stimulates ductal proliferation) and is suppressed by androgens. Any condition that raises effective estrogen or reduces effective androgen produces gynecomastia.
Etiological classification:
| Category | Examples | Mechanism |
|---|---|---|
| Physiological | Neonatal, pubertal, senescent | Transient E/A imbalance at age extremes |
| Drugs | Spironolactone, cimetidine, digoxin, anabolic steroids, marijuana, metoclopramide, ketoconazole | Anti-androgen, estrogen agonist, ↑ aromatase, ↑ prolactin |
| Liver disease (cirrhosis) | Alcoholic cirrhosis | ↓ androgen clearance by liver + ↑ aromatase in fat; alcohol also directly inhibits testosterone synthesis |
| Hypogonadism | Klinefelter syndrome (47,XXY), orchitis, cryptorchidism | ↓ testosterone production |
| Endocrine tumors | Leydig cell tumor, adrenal cortical tumor, HCG-secreting tumors | Excess estrogen or HCG (stimulates testicular estrogen) |
| Renal failure | Dialysis patients | Altered hormone metabolism |
| Malnutrition/refeeding | Concentration camp survivors, anorexia recovery | Relative estrogen rebound ('refeeding gynecomastia') |
Pubertal gynecomastia (most common type): occurs in 50–60% of adolescent males at Tanner stage 3–4. Caused by transient estrogen excess before testosterone fully rises. Regresses spontaneously within 2 years in >90%.
Drug causes to memorise (high-yield):
• Anti-androgens: spironolactone (K-sparing diuretic), finasteride, flutamide
• Estrogen agonists: diethylstilbestrol, phytoestrogens
• ↑ Prolactin (indirect): metoclopramide, domperidone, antipsychotics (haloperidol, risperidone)
• Anabolic steroids: aromatised peripherally to estradiol
• Digoxin: structural similarity to estrogen
Estrogen/Androgen Imbalance and Pathogenesis of Gynecomastia
Gynecomastia — Pathogenesis and Morphology
Pathogenesis:
Estrogen receptor activation in male breast tissue → ductal epithelial hyperplasia → periductal stromal proliferation and edema → palpable retroareolar disc.
Two histological phases:
1. Florid (active) phase — early, reversible: marked ductal epithelial hyperplasia, loose edematous periductal stroma, increased vascularity. If the cause is removed at this stage, regression can occur.
2. Fibrous (inactive) phase — late, irreversible: ductal hyperplasia subsides; dense periductal hyalinised fibrosis replaces stroma. This phase does not regress after cause removal.
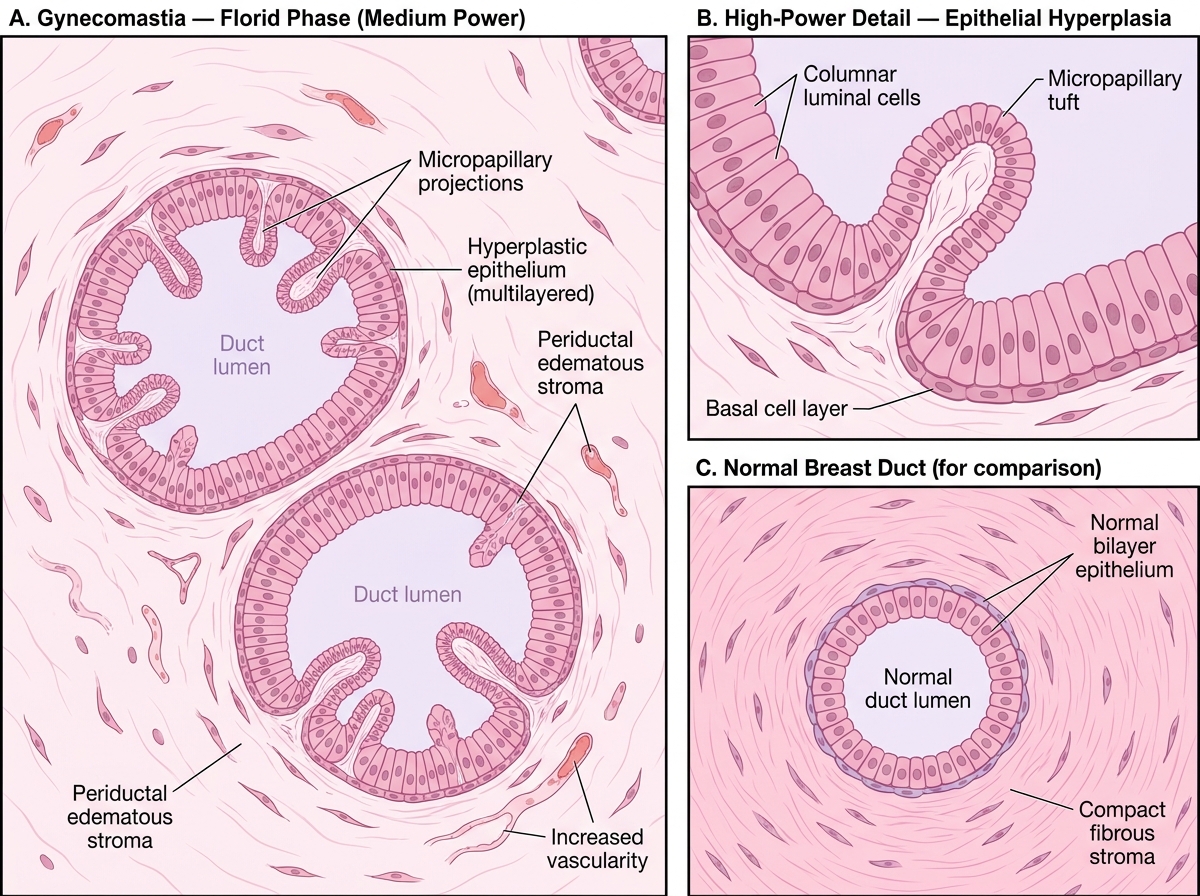
Morphology:
• Gross: rubbery button-like firm subareolar disc, usually 2–4 cm (may be unilateral or bilateral)
• Microscopic (florid phase): proliferating ducts lined by multilayered epithelium; loose, vascular, edematous periductal stroma; occasional intraluminal micropapillary tufts; minimal lobule formation (male breast lacks normal lobules)
• Microscopic (fibrous phase): few ducts, dense pericollaginous fibrosis, no active proliferation
Important: Lobules are absent in gynecomastia, because lobular development requires progesterone, which is absent in males. Ductal structures only.
Relationship to male breast carcinoma:
Gynecomastia itself does not significantly increase risk of male breast carcinoma. However, the underlying cause may: Klinefelter syndrome has 20–50× increased risk of male breast cancer. Men with gynecomastia warrant investigation for underlying etiology.
Histology of Gynecomastia — Florid Phase vs. Normal Breast Duct
CLINICAL PEARL
Gynecomastia workup — a systematic approach:
When a male patient presents with breast enlargement, ask:
1. Drugs? — review entire medication list (spironolactone and antipsychotics are the most overlooked)
2. Liver disease? — look for spider naevi, palmar erythema, jaundice
3. Testicular exam — small firm testes → Klinefelter; hard nodule → Leydig cell tumor; soft atrophic → hypogonadism
4. Investigations: LFTs, testosterone/LH/FSH, estradiol, β-HCG, AFP (to exclude testicular germ cell tumor causing HCG-driven gynecomastia)
Bilateral, soft, pubertal-onset in an adolescent = physiological — no workup needed if regression begins by 18 months.
Unilateral, hard, eccentric, progressive in an adult = biopsy to exclude male breast carcinoma.
SELF-CHECK
A 55-year-old man with alcoholic cirrhosis develops bilateral tender breast enlargement. Biopsy of the right breast shows dilated ducts lined by multilayered hyperplastic ductal epithelium with intraluminal tufts, and surrounding loose edematous periductal stroma. No lobules are identified. What phase of gynecomastia is this, and what is the primary pathophysiological mechanism in cirrhosis?
A. Fibrous phase; decreased androgen clearance leads to androgen excess
B. Florid phase; decreased hepatic clearance of estrogens and increased peripheral aromatase activity shift the estrogen/androgen ratio toward estrogen excess
C. Florid phase; direct toxic effect of alcohol on breast ductal epithelium
D. Fibrous phase; elevated prolactin from liver failure stimulates ductal proliferation
Reveal Answer
Answer: B. Florid phase; decreased hepatic clearance of estrogens and increased peripheral aromatase activity shift the estrogen/androgen ratio toward estrogen excess
Loose, edematous periductal stroma with active ductal hyperplasia is the hallmark of the florid (active) phase of gynecomastia. In cirrhosis, two mechanisms converge: (1) impaired hepatic metabolism of estrogens → elevated serum estradiol; (2) increased adipose aromatase converts adrenal androgens to estrogens. Alcohol also directly suppresses testicular testosterone synthesis via inhibition of 17β-hydroxysteroid dehydrogenase. The net effect is a markedly elevated estrogen/androgen ratio. Prolactin elevation does not cause gynecomastia directly.