Page 4 of 19
PA30.{1,4} | Benign Breast Disease & Gynecomastia — Summary & Reflection
REFLECT
Pause here before reading the summary.
Reflect on these three scenarios and formulate your answer before scrolling:
- A biopsy report arrives: 'Fibrocystic change with sclerosing adenosis and atypical ductal hyperplasia bilaterally; family history: mother diagnosed with breast cancer at 52.' What specific carcinoma risk estimate do you give, and what surveillance plan do you recommend?
- A histopathology slide shows a breast lesion with fibrovascular papillary fronds. The inner epithelial layer stains for CK7; the outer layer does NOT stain with p63. Is this a benign intraductal papilloma or a malignant papillary lesion? What is the key discriminating finding?
- A 28-year-old male presents with bilateral breast enlargement after starting spironolactone for ascites. Which phase of gynecomastia would you expect on biopsy if the drug was started 3 weeks ago? If the drug was started 3 years ago and never stopped?
Think through these before moving to the summary — active retrieval consolidates learning more than re-reading.
KEY TAKEAWAYS
Core concepts to retain from this SDL:
Normal breast:
• TDLU = functional unit; myoepithelial cells are the benignity sentinel
• Estrogen → ducts; progesterone → lobules; both → full lactational development
Inflammatory/reactive:
• Acute mastitis → S. aureus, lactation; abscess formation
• Periductal mastitis → duct ectasia + plasma cell infiltrate; simulates carcinoma
• Fat necrosis → ghost adipocytes + lipophages + dystrophic calcification; simulates carcinoma on mammogram
Fibrocystic change — carcinoma risk:
• Non-proliferative = no increased risk
• Proliferative without atypia = 1.5–2×
• ADH/ALH = 4–5× (×2 if family history → 8–10×)
Fibroadenoma:
• Commonest benign tumor; 15–35 yrs; estrogen-sensitive
• Biphasic: intracanalicular (slit-like) vs. pericanalicular (round) pattern
• Myoepithelial layer intact = benign; hypercellular stroma = phyllodes
Intraductal papilloma:
• Commonest cause of bloody nipple discharge
• Dual cell layer (luminal + myoepithelial, p63+) = benign
• Loss of myoepithelial layer = papillary carcinoma
Triple assessment: clinical + imaging + pathology; all three concordantly benign = >99.6% negative predictive value
Gynecomastia:
• Mechanism: ↑ estrogen / ↓ androgen ratio
• Causes: physiological (puberty), drugs, cirrhosis, hypogonadism, tumors
• Florid phase: ductal hyperplasia + edematous stroma (reversible)
• Fibrous phase: hyalinised stroma (irreversible)
• No lobules (progesterone absent in males)
• Klinefelter syndrome → 20–50× risk male breast carcinoma
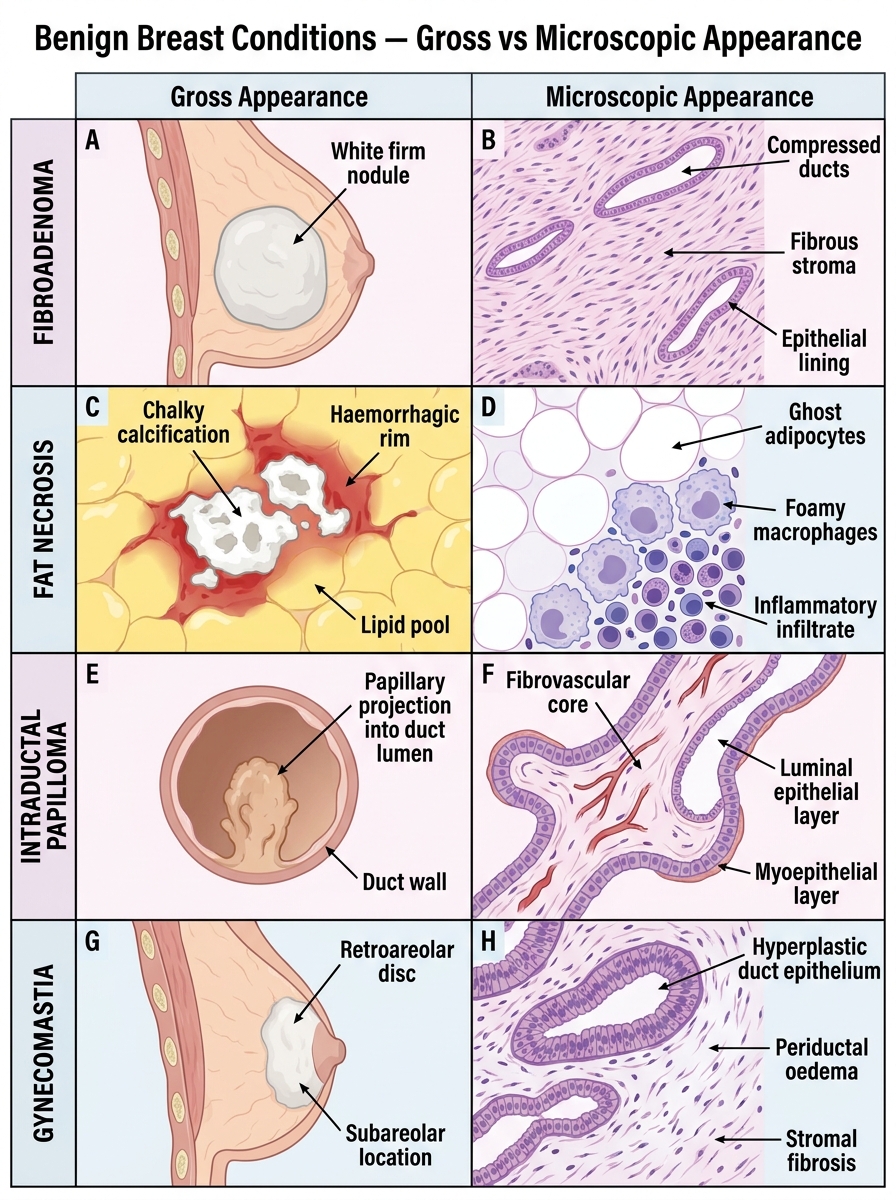
Benign Breast Conditions — Gross vs Microscopic Comparison