Page 5 of 19
PA30.2 | Carcinoma of the Breast — SDL Guide
Learning Objectives
- Classify carcinoma of the breast into in situ (DCIS, LCIS) and invasive categories with their subtypes.
- Describe the epidemiology, hormonal risk factors, and hereditary predisposition (BRCA1/2) for breast cancer.
- Explain the molecular pathogenesis: ER signalling pathway, HER2 amplification, and the ductal carcinogenesis sequence.
- Compare the gross and microscopic features of the common invasive carcinoma subtypes (IDC NST, ILC, medullary, mucinous, tubular, inflammatory, Paget disease).
- Classify breast carcinoma by molecular/intrinsic subtype (Luminal A/B, HER2-enriched, basal-like/triple-negative) and relate this to ER/PR/HER2 immunohistochemistry.
- Apply the Nottingham (Bloom-Richardson) grading system and TNM staging to a breast carcinoma case.
- List the prognostic and predictive factors and describe the routes of spread of breast carcinoma.
INSTRUCTIONS
Breast carcinoma is the most common cancer in women worldwide and a top cause of cancer death in Indian women. Understanding its classification and molecular biology is essential not only for the pathology examination but for appreciating how modern oncologists choose surgery, chemotherapy, hormonal therapy, and targeted agents. Work through each block sequentially; use the micro-quizzes to self-test before moving on.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 23 — The Breast (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch. 27 — Diseases of the Breast (textbook)
- Kumar, Abbas & Aster: Robbins Basic Pathology, 10th ed., Ch. 22 (textbook)
- WHO Classification of Tumours of the Breast, 5th ed., 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old woman notices a hard, painless lump in her right breast upper outer quadrant. Fine-needle aspiration shows clusters of pleomorphic cells with irregular nuclei. Her mother had breast cancer at 52. Immunohistochemistry of the core biopsy returns: ER+, PR+, HER2 2+ (equivocal), Ki-67 18%. Her oncologist orders a FISH test and recommends a multidisciplinary tumour board review.
By the end of this module, you will understand exactly why each of those IHC markers was ordered, what the results mean for prognosis, and how the microscopic features you study today translate directly into the treatment decision for this patient.
WHY THIS MATTERS
Breast carcinoma is the most common invasive cancer in women globally, accounting for ~2.3 million new cases per year (WHO 2022). In India it has overtaken cervical cancer as the leading female malignancy. For Year-2 MBBS, this topic appears in every university theory and practical examination. More importantly, pathologists issue every diagnosis that drives surgery, chemotherapy, and targeted therapy — understanding the morphology and molecular subtypes makes you an effective partner in the multidisciplinary team from day one of clinical posting.
RECALL
Before starting, test your recall:
- Name the two main in situ breast lesions you should know.
- Which chromosome carries BRCA1? Which carries BRCA2?
- What does the term desmoplasia mean histologically?
- What are the three parameters in the Nottingham grading system?
- Which lymph node group is most important in breast cancer staging?
If any of these are unfamiliar, that is fine — each will be covered in detail. Use them as a roadmap for what to watch for.
Epidemiology and Risk Factors
Breast carcinoma has a bimodal age distribution: a small pre-menopausal peak and a larger post-menopausal peak; the median age at diagnosis in India is ~50–52 years, roughly a decade earlier than in Western populations.
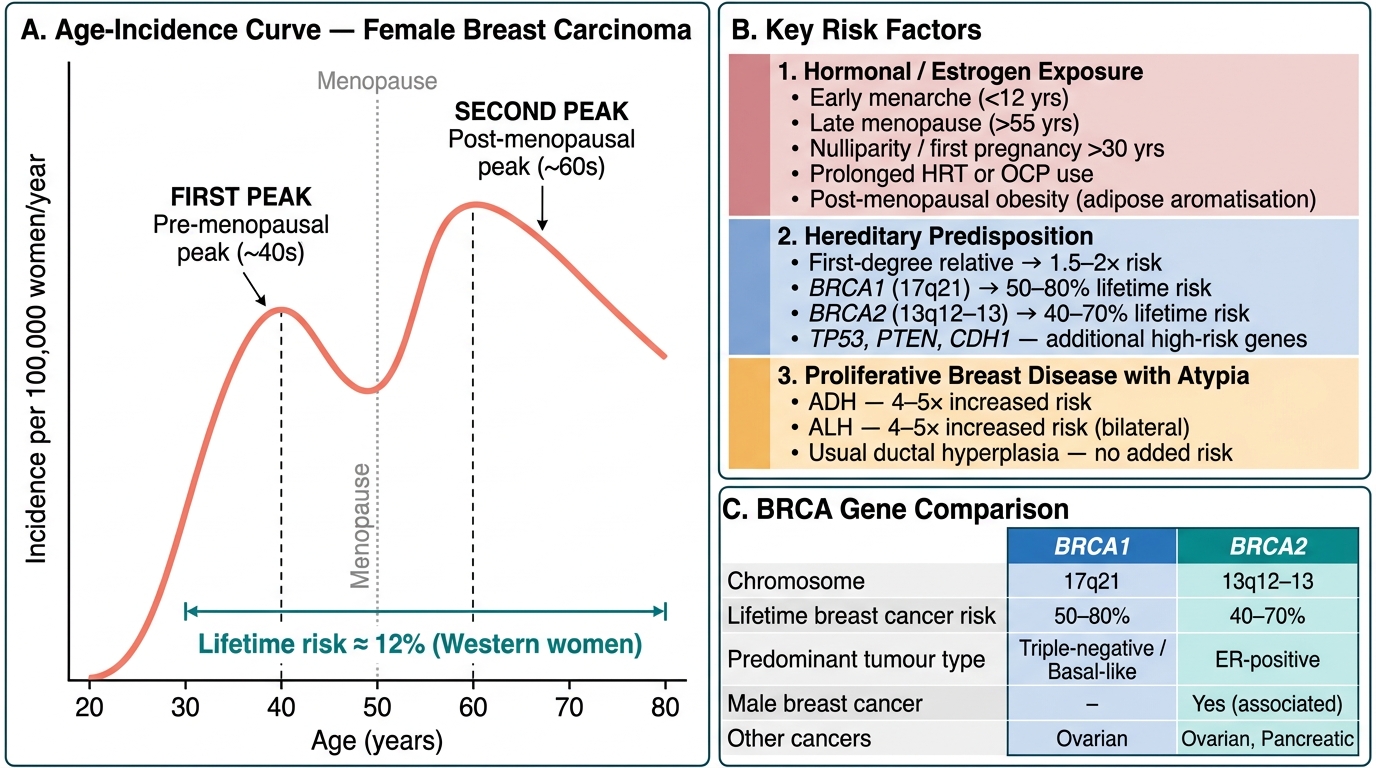
Epidemiology of Breast Carcinoma: Age-Incidence Curve and Key Risk Factors
Risk factors can be organised into three broad categories:
1. Hormonal/Estrogen Exposure
• Early menarche (<12 yrs) and late menopause (>55 yrs) — prolonged estrogen exposure
• Nulliparity or first pregnancy after age 30
• Prolonged combined HRT or oral contraceptive use
• Obesity (post-menopausal: adipose tissue aromatises androgens → estrogen)
• Exogenous estrogen (DES exposure in utero — rare)
2. Hereditary Predisposition
• First-degree relative with breast cancer → 1.5–2× risk; 2 relatives → 2–4×
• BRCA1 (chromosome 17q21) — predominantly triple-negative / basal-like carcinomas; lifetime risk 50–80%
• BRCA2 (chromosome 13q12–13) — more often ER-positive carcinomas; lifetime risk 40–70%; also associated with male breast cancer
• Other high-risk genes: TP53 (Li-Fraumeni), PTEN (Cowden syndrome), CDH1 (hereditary lobular carcinoma)
3. Proliferative Breast Disease with Atypia
• Usual ductal hyperplasia — no increased risk
• Sclerosing adenosis — slight risk
• Atypical ductal hyperplasia (ADH) — 4–5× increased risk
• Atypical lobular hyperplasia (ALH) — 4–5× increased risk (risk is bilateral)
Other factors: ionising radiation (especially in adolescence — e.g. mantle field radiation for Hodgkin lymphoma), high breast density on mammography, and contralateral breast cancer all increase risk.
Pathogenesis: Molecular Pathways
Three major molecular mechanisms underlie the development of breast carcinoma.
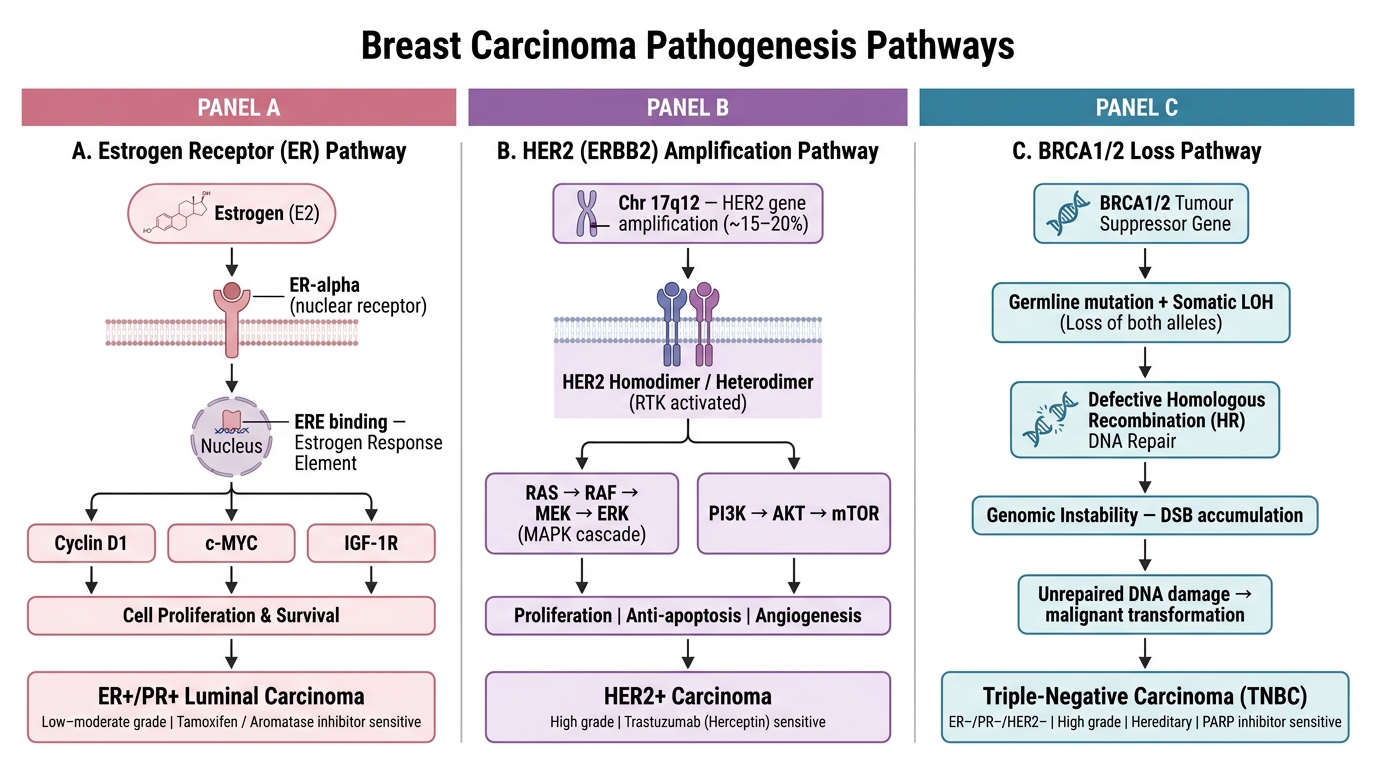
Three Molecular Pathways to Breast Carcinoma
1. Estrogen Receptor (ER) Pathway — Luminal Carcinomas
Estrogen binds nuclear ER-alpha → receptor-ligand complex translocates to nucleus → binds estrogen response elements → upregulates cyclin D1, c-MYC, IGF-1R → cell proliferation and survival. Prolonged ER stimulation accumulates mutations in ductal epithelium. These tumours are ER+/PR+, low to moderate grade, and respond to hormonal therapy (tamoxifen, aromatase inhibitors).
2. HER2 (ERBB2) Amplification Pathway
HER2 (chromosome 17q12) encodes a receptor tyrosine kinase. Amplification (not just overexpression) occurs in ~15–20% of breast carcinomas. The activated HER2 homodimer/heterodimer drives RAS-MAPK and PI3K-AKT-mTOR signalling → uncontrolled proliferation, anti-apoptosis, angiogenesis. These tumours are high-grade, aggressive, and sensitive to trastuzumab (Herceptin) — an anti-HER2 monoclonal antibody.
3. BRCA1/2 Pathway — Hereditary & Triple-Negative Carcinomas
BRCA1/2 are tumour suppressor genes encoding proteins critical for homologous recombination DNA repair. Loss of both alleles (germline mutation + somatic LOH) causes genomic instability. BRCA1-related tumours are typically high-grade, ER/PR/HER2-negative (triple-negative), basal-like; BRCA2 tumours are more often ER-positive. These tumours cannot repair double-strand DNA breaks and are exquisitely sensitive to PARP inhibitors (e.g. olaparib).
The Ductal Carcinogenesis Sequence:
Normal ductal epithelium → usual ductal hyperplasia (UDH) → atypical ductal hyperplasia (ADH) → ductal carcinoma in situ (DCIS) → invasive ductal carcinoma. Each step accumulates molecular alterations: ER expression, HER2 amplification, TP53 mutation, and loss of CDKN2A (p16). This sequence takes 10–15 years on average.
CLINICAL PEARL
BRCA testing and surgical decision-making: When a premenopausal woman is diagnosed with triple-negative breast cancer, BRCA1/2 germline testing is reflexively offered. A confirmed BRCA1 mutation changes the surgical plan (risk-reducing contralateral mastectomy), guides surveillance (ovarian cancer risk), and opens eligibility for PARP inhibitors. The pathologist's role begins with accurate hormone receptor and HER2 reporting — that single IHC report can dictate whether a patient undergoes additional genetic testing.
Ductal Carcinoma In Situ (DCIS)
Ductal carcinoma in situ (DCIS) is a malignant proliferation of ductal epithelial cells confined within the basement membrane — there is no invasion of the surrounding stroma. It is detectable by mammography (often as clustered microcalcifications) and represents ~15–25% of screen-detected breast cancers.
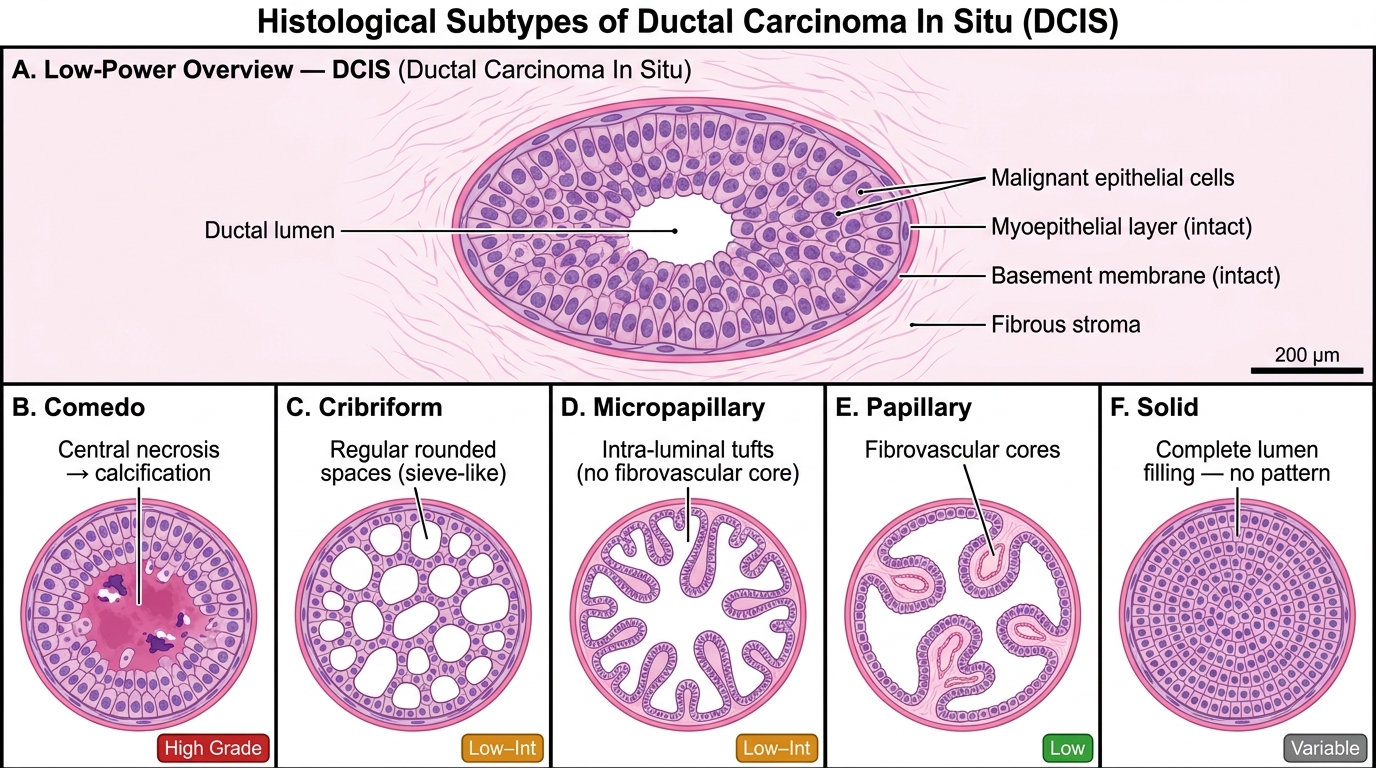
DCIS: Annotated Histology and Architectural Classification
Classification by Architecture and Grade:
| Pattern | Key Feature | Grade |
|---|---|---|
| Comedo | Central necrosis (ghost cells) → calcifies → linear/branching microcalcs on mammogram | High |
| Cribriform | Regular rounded spaces (sieve-like) within solid cell sheets | Low–intermediate |
| Micropapillary | Intra-luminal papillary tufts without fibrovascular cores | Low–intermediate |
| Papillary | Papillary fronds with fibrovascular cores; often in elderly women | Low |
| Solid | Completely fills lumen with no special pattern | Variable |
Comedo DCIS is the most clinically important subtype:
• Central coagulative necrosis of high-grade cells that calcify → linear/branching microcalcifications on mammography
• High nuclear grade, prominent mitoses, HER2 amplification common
• Highest risk of progression to invasive carcinoma (~30–50% if untreated)
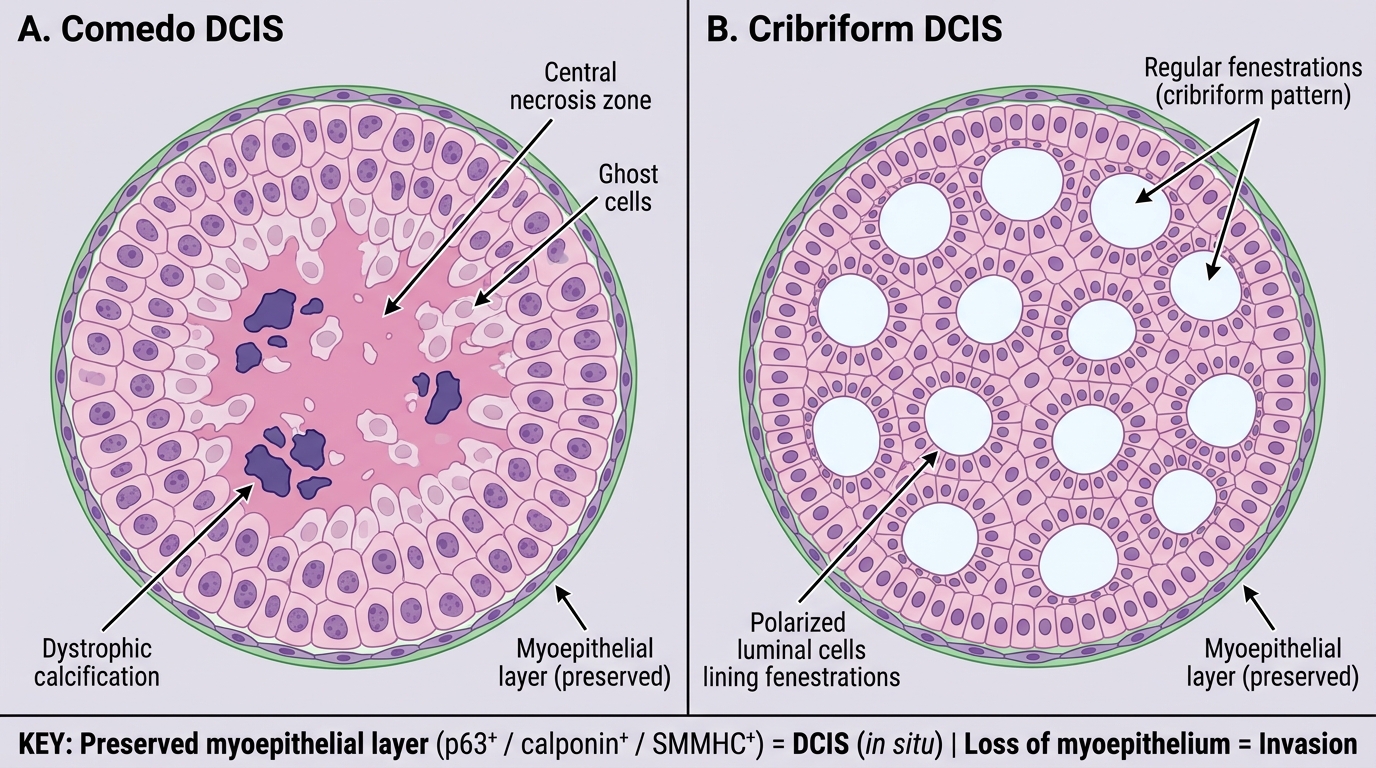
Comedo vs Cribriform DCIS — Medium Power Comparison
Key distinction: In DCIS, the myoepithelial cell layer is preserved (demonstrable by IHC with p63, calponin, or smooth muscle myosin heavy chain). Loss of myoepithelium = invasion. This is the critical distinguishing feature between in situ and invasive carcinoma in daily diagnostic practice.