Page 6 of 19
PA30.2 | Carcinoma of the Breast — SDL Guide (Part 2)
Lobular Carcinoma In Situ (LCIS)
Lobular carcinoma in situ (LCIS) is a proliferation of small, uniform, loosely cohesive cells filling and distending the terminal duct-lobular unit (TDLU) without invading the stroma. Unlike DCIS, LCIS is almost never palpable or mammographically visible — it is most often an incidental finding in breast biopsies done for other reasons.
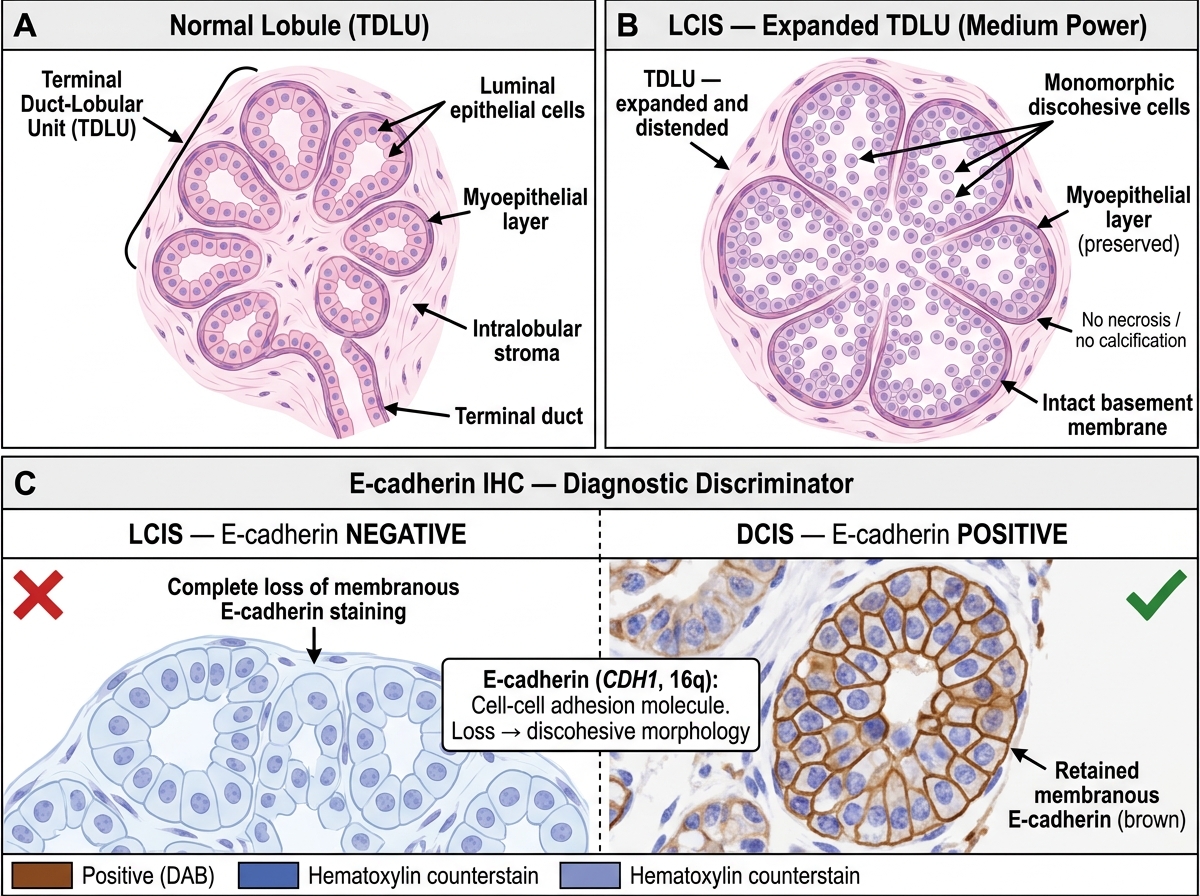
LCIS: Histology and E-cadherin Immunophenotype
Key molecular feature: Loss of E-cadherin expression (encoded by CDH1, chromosome 16q). E-cadherin is a cell-cell adhesion molecule; its loss explains the characteristic discohesive/non-cohesive cell morphology seen in LCIS and its invasive counterpart, invasive lobular carcinoma. IHC for E-cadherin shows complete absence of membranous staining in LCIS cells (positive in DCIS — a useful diagnostic discriminator).
Clinical significance:
• LCIS is a bilateral risk marker — risk increased ~4× in both breasts (not just the biopsy side)
• ~1–2% per year risk of developing invasive carcinoma (lobular or ductal)
• Treated with close surveillance ± chemoprevention (tamoxifen/raloxifene) rather than surgery
• Pleomorphic LCIS (rare variant with higher-grade cells, necrosis) behaves more like DCIS and may be excised
SELF-CHECK
A pathologist examining a breast biopsy performs E-cadherin immunohistochemistry. The in situ lesion shows complete loss of E-cadherin expression. Which in situ carcinoma does this confirm?
A. Ductal carcinoma in situ (DCIS), cribriform type
B. Ductal carcinoma in situ (DCIS), comedo type
C. Lobular carcinoma in situ (LCIS)
D. Atypical ductal hyperplasia (ADH)
Reveal Answer
Answer: C. Lobular carcinoma in situ (LCIS)
E-cadherin loss is the hallmark of lobular neoplasia (LCIS and invasive lobular carcinoma). It is encoded by CDH1 and its loss results in cell discohesion — the defining morphological feature. DCIS retains E-cadherin expression and is therefore E-cadherin positive on IHC. ADH also retains E-cadherin.
Invasive Ductal Carcinoma — No Special Type (NST)
Invasive ductal carcinoma of no special type (IDC NST) — also called invasive carcinoma NST in the WHO 2022 classification — is the most common breast malignancy, accounting for ~70–80% of all invasive breast carcinomas. The term "no special type" reflects that it does not show sufficient features to classify it as one of the special types.
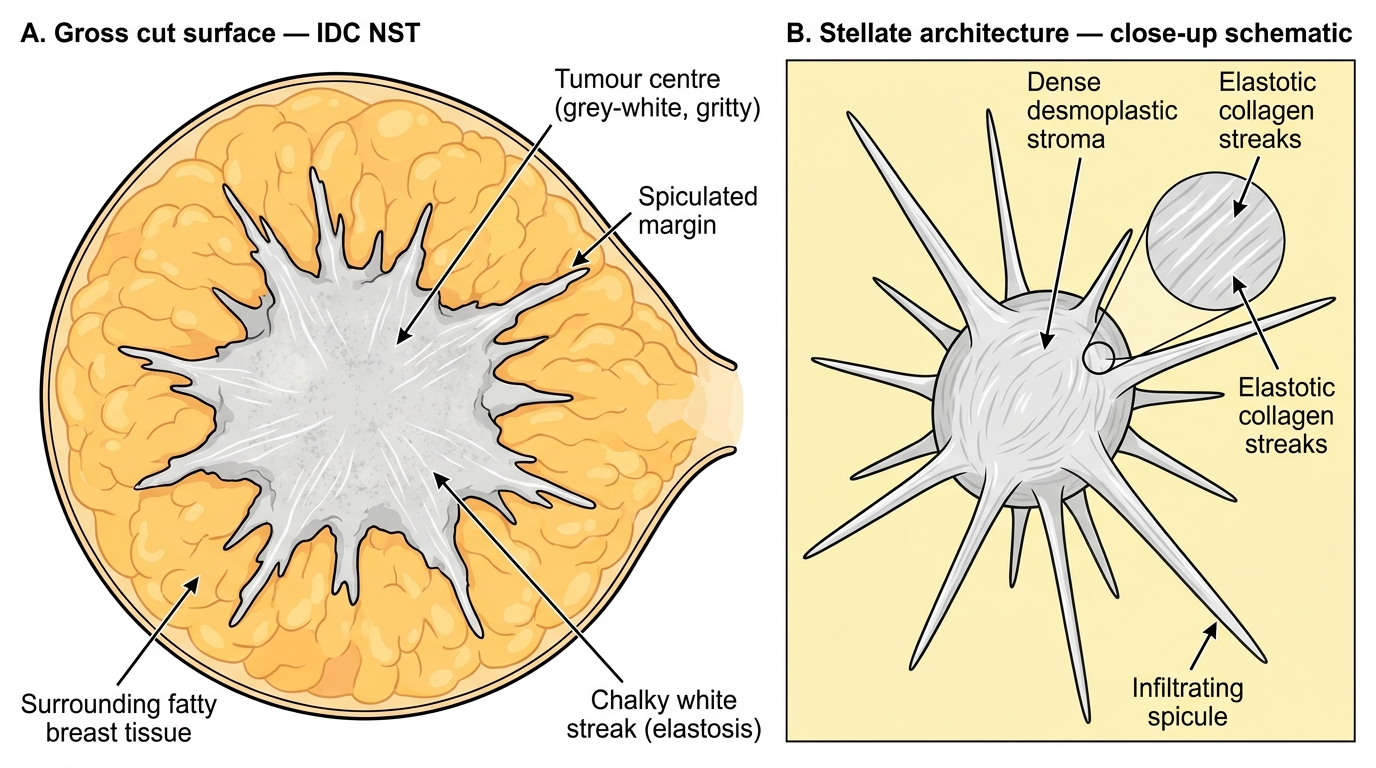
Gross features of Invasive Ductal Carcinoma, No Special Type (IDC NST)
Gross features:
• Firm to hard (scirrhous) mass — due to extensive desmoplasia
• Irregular, stellate (star-shaped) margins that infiltrate surrounding fat
• Cut surface: grey-white, gritty texture (fibrotic stroma)
• Chalky white streaks represent elastosis of periductal collagen
• May show skin dimpling (tethering of Cooper's ligaments), nipple retraction
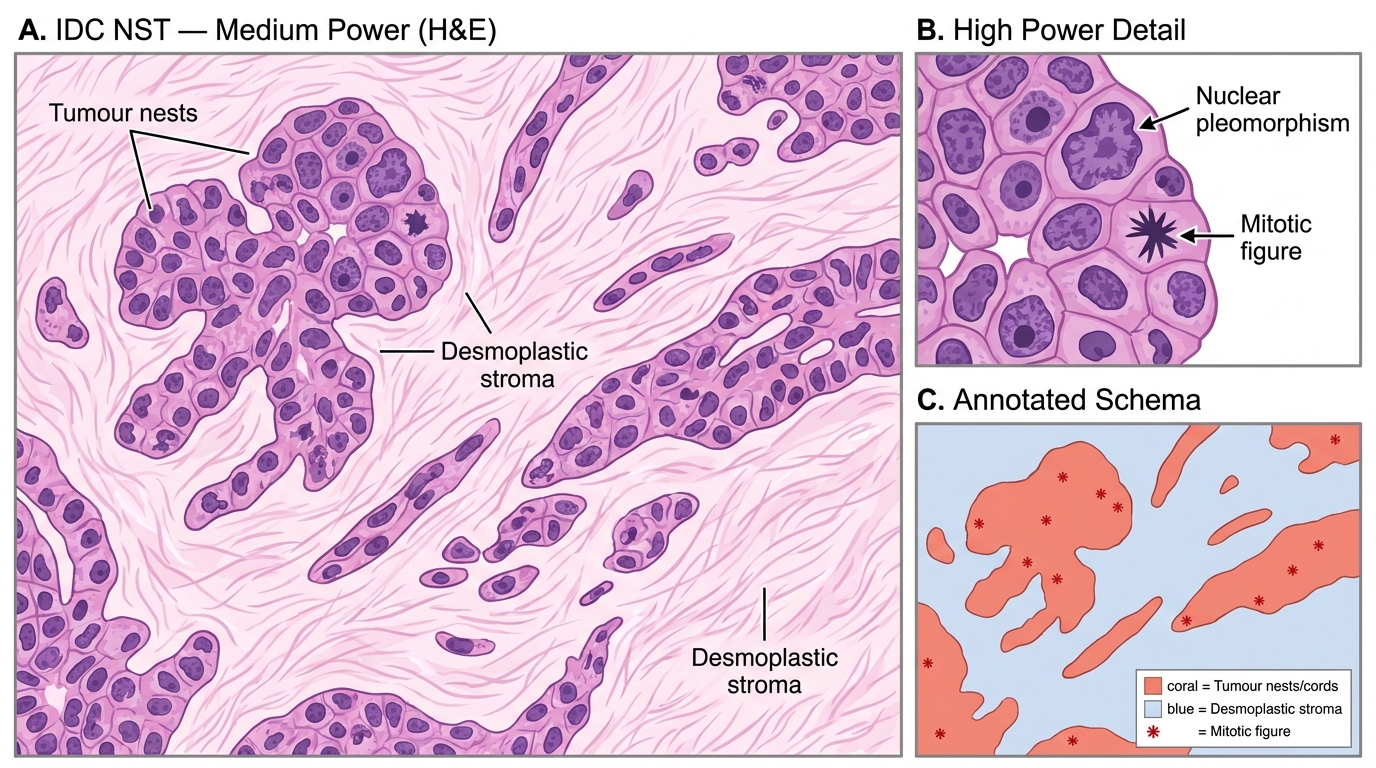
Histology of Invasive Ductal Carcinoma NST — Architecture, Stroma, and Cytological Features
Microscopic features:
• Malignant epithelial cells arranged in nests, cords, solid sheets, or tubules — with variable patterns
• Dense desmoplastic stroma (fibroblastic reaction to tumour invasion) — this is responsible for the hard, gritty feel on gross
• Cells show nuclear pleomorphism, prominent nucleoli, variable mitoses
• May have associated DCIS ("DCIS component")
• Perineural invasion and lymphovascular invasion may be present
IHC profile: Variable — may be ER+/PR+/HER2− (most common), HER2+, or triple-negative, depending on the specific tumour.
Invasive Lobular Carcinoma
Invasive lobular carcinoma (ILC) is the second most common invasive breast carcinoma (~10–15%). It is characterised by a unique growth pattern directly attributable to loss of E-cadherin (same CDH1 deletion as LCIS).
Histological Patterns of Invasive Lobular Carcinoma — Indian File and Targetoid Arrangements
Gross features:
• Often no discrete mass — diffuse rubbery induration of the breast
• Can be difficult to detect clinically and mammographically (low desmoplasia, no calcifications)
• May cause bilateral involvement more often than IDC
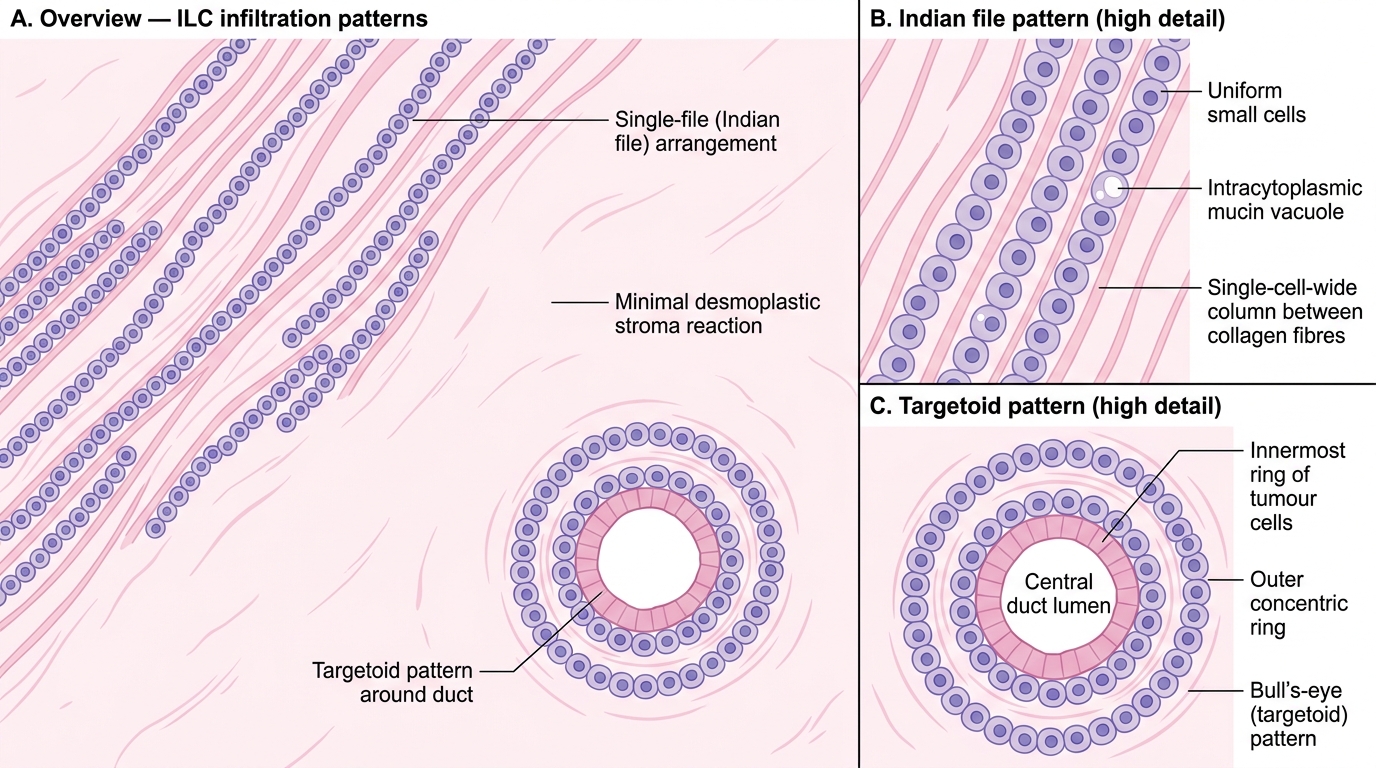
Microscopic features — classic pattern:
1. Single-file (Indian file) infiltration — cells arranged in single rows between collagen bundles
2. Targetoid pattern — concentric rings of tumour cells around a central duct
3. Minimal desmoplasia — unlike IDC NST, stroma reaction is sparse
4. Cells are small, uniform, with scanty cytoplasm and intracytoplasmic mucin vacuoles ("signet-ring" cells in variant)
5. E-cadherin negative on IHC
IHC profile: Almost universally ER+/PR+ (strongly hormone-dependent); HER2 amplification is rare; triple-negative ILC is uncommon.
Spread: ILC has a peculiar metastatic pattern — it preferentially spreads to the peritoneum, retroperitoneum, and gastrointestinal tract (particularly stomach, simulating linitis plastica), ovaries, and leptomeninges — in addition to axillary nodes and bone.
CLINICAL PEARL
Why ILC is the great mimicker: Because invasive lobular carcinoma produces minimal desmoplasia and infiltrates diffusely without forming a discrete mass, it can be mammographically occult (negative mammogram despite palpable disease). MRI is more sensitive. Histologically, the single-file pattern is sometimes subtle and can mimic a fibrous scar or chronic inflammation at low power. The stain for E-cadherin (negative in ILC, positive in IDC) is the decisive IHC test when the morphology is ambiguous.