Page 7 of 19
PA30.2 | Carcinoma of the Breast — SDL Guide (Part 3)
Special Invasive Types: Medullary, Mucinous, and Tubular Carcinoma
Several invasive carcinoma types have better prognosis than IDC NST when diagnosis is strict. They account for ~5–10% of invasive breast carcinomas collectively.
Breast Carcinoma Histology: Medullary vs Mucinous (Colloid) Subtypes
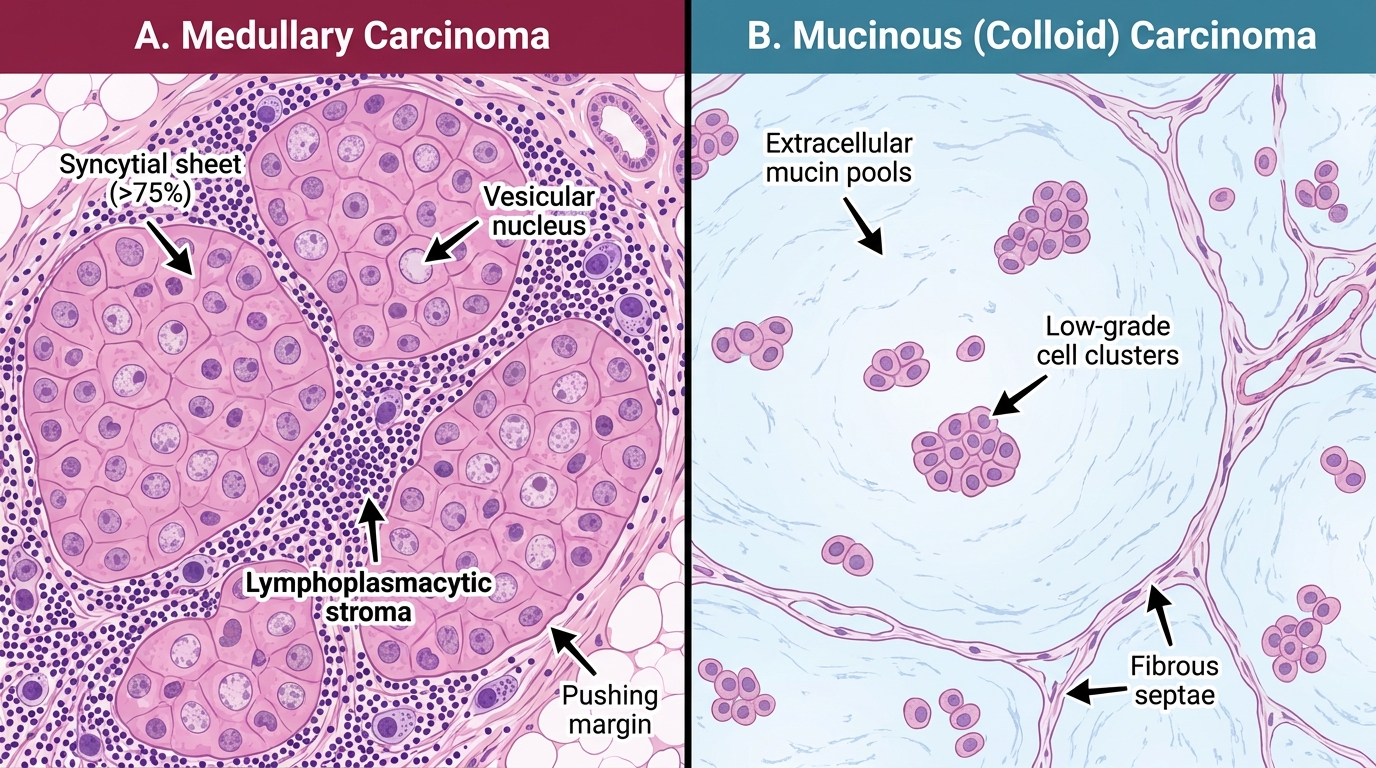
1. Medullary Carcinoma (Classic)
• Rare; more common in BRCA1 mutation carriers
• Soft, well-circumscribed, fleshy ("pusher" margins — not invasive-stellate)
• Histology: Syncytial sheets (>75%) of high-grade vesicular-nucleus cells + prominent lymphoplasmacytic infiltrate in stroma
• Triple-negative (ER−/PR−/HER2−) yet paradoxically better prognosis than grade-matched IDC NST
• Good prognosis relates to the immune infiltrate — tumour-infiltrating lymphocytes (TILs) are a favourable prognostic marker
2. Mucinous (Colloid) Carcinoma
• Mostly in older women (>60 yrs)
• Gross: Glistening, gelatinous, grey-blue tumour
• Histology: Small, uniform, low-grade tumour cells floating in large pools of extracellular mucin (mucin surrounds cell clusters, not intracellular)
• ER+/PR+, low proliferation, very favourable prognosis (>90% 10-year survival for pure mucinous)
3. Tubular Carcinoma
• Detected by screening mammography as a tiny spiculated lesion
• Histology: Well-formed, open, angulated tubules lined by a single layer of bland low-grade cells, infiltrating stroma; no myoepithelium around tubules (distinguishes from sclerosing adenosis)
• Grade 1 by definition; ER+/PR+
• Excellent prognosis — 10-year survival >95%
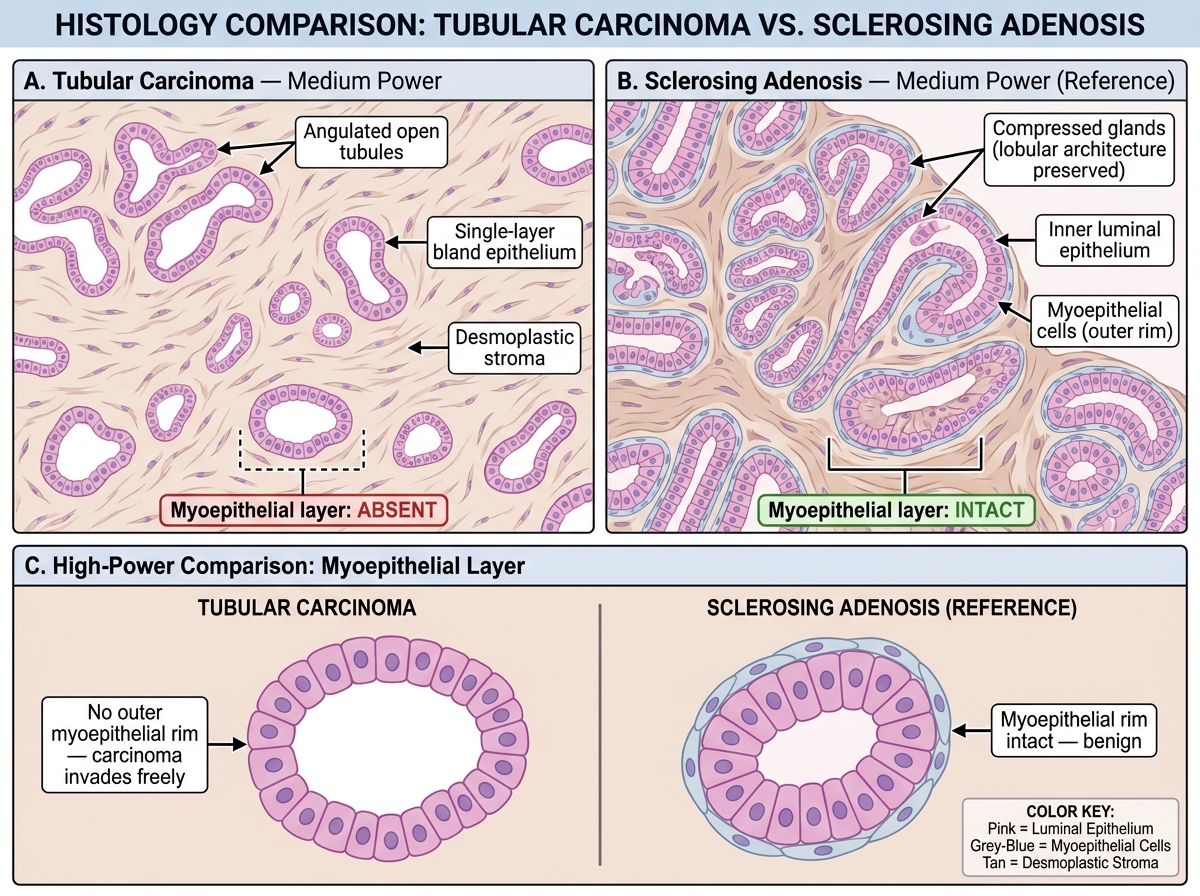
Tubular Carcinoma vs Sclerosing Adenosis — Medium and High Power Histology
Inflammatory Carcinoma and Paget Disease of the Nipple
These two entities have distinctive clinical presentations and are must-know for examinations.
Inflammatory Carcinoma
Inflammatory carcinoma is a clinical diagnosis, not a histologic subtype. It is the most aggressive presentation of breast carcinoma.
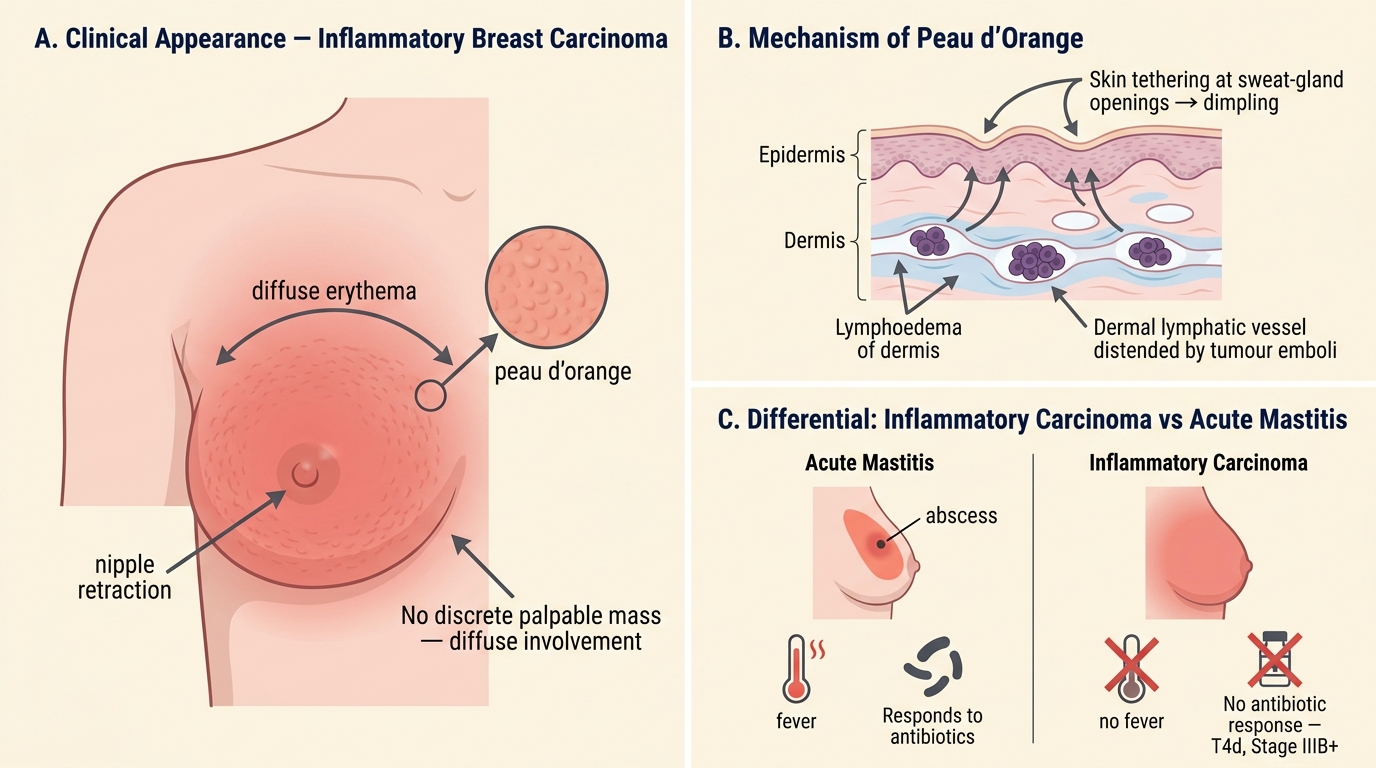
Inflammatory Carcinoma of the Breast — Clinical Features, Mechanism of Peau d'Orange, and Differential Diagnosis
- Presentation: Rapid onset (weeks) of breast erythema, warmth, tenderness, swelling, and skin oedema resembling acute mastitis — but without fever and without response to antibiotics
- Peau d'orange (orange-peel skin): Dermal lymphatic obstruction by tumour emboli causes lymphoedema of the skin → tethering of skin at sweat-gland openings → orange-peel texture
- Key histological finding: Dermal lymphatic invasion — tumour cell emboli within dermal lymphatics. This is required for diagnosis (not just carcinoma with secondary skin oedema)
- Usually high-grade, ER-negative, HER2+ or triple-negative
- Staging: T4d (Stage IIIB minimum) regardless of tumour size
- Treated with neoadjuvant chemotherapy first (not primary surgery)
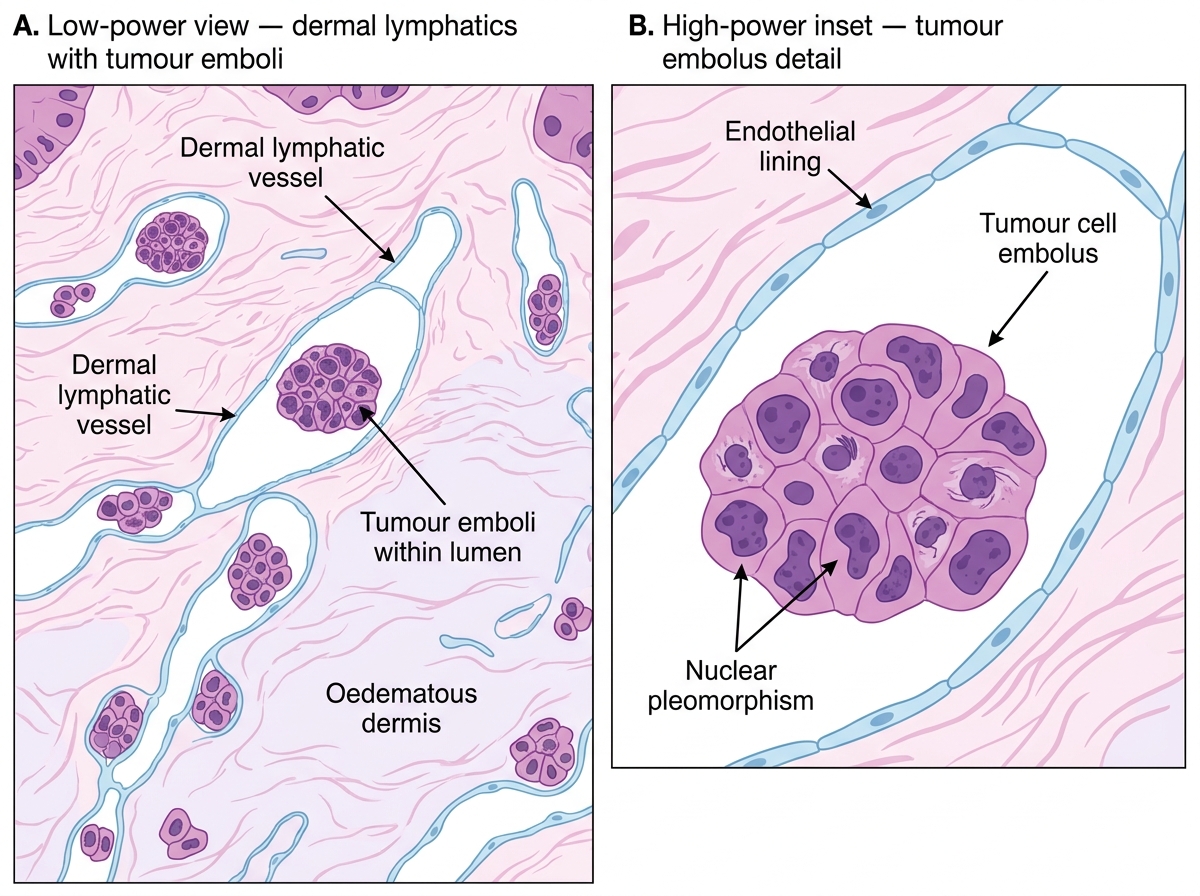
Histology of Inflammatory Carcinoma — Dermal Lymphatic Tumour Emboli
Paget Disease of the Nipple
- Clinical: Eczematous, crusted, itchy, erythematous lesion of the nipple-areola complex, may ooze/bleed; mimics eczema but does NOT respond to topical steroids
- Histology: Large, pale, vacuolated malignant cells (Paget cells) individually or in clusters within the squamous epithelium of the nipple epidermis, with a clear halo around each cell
- Pathogenesis: Malignant ductal cells migrate from an underlying DCIS (or invasive carcinoma) up the nipple ducts into the epidermis
- Key point: Paget disease of the nipple always indicates underlying carcinoma (DCIS in ~30–40%, invasive carcinoma in ~60–70%)
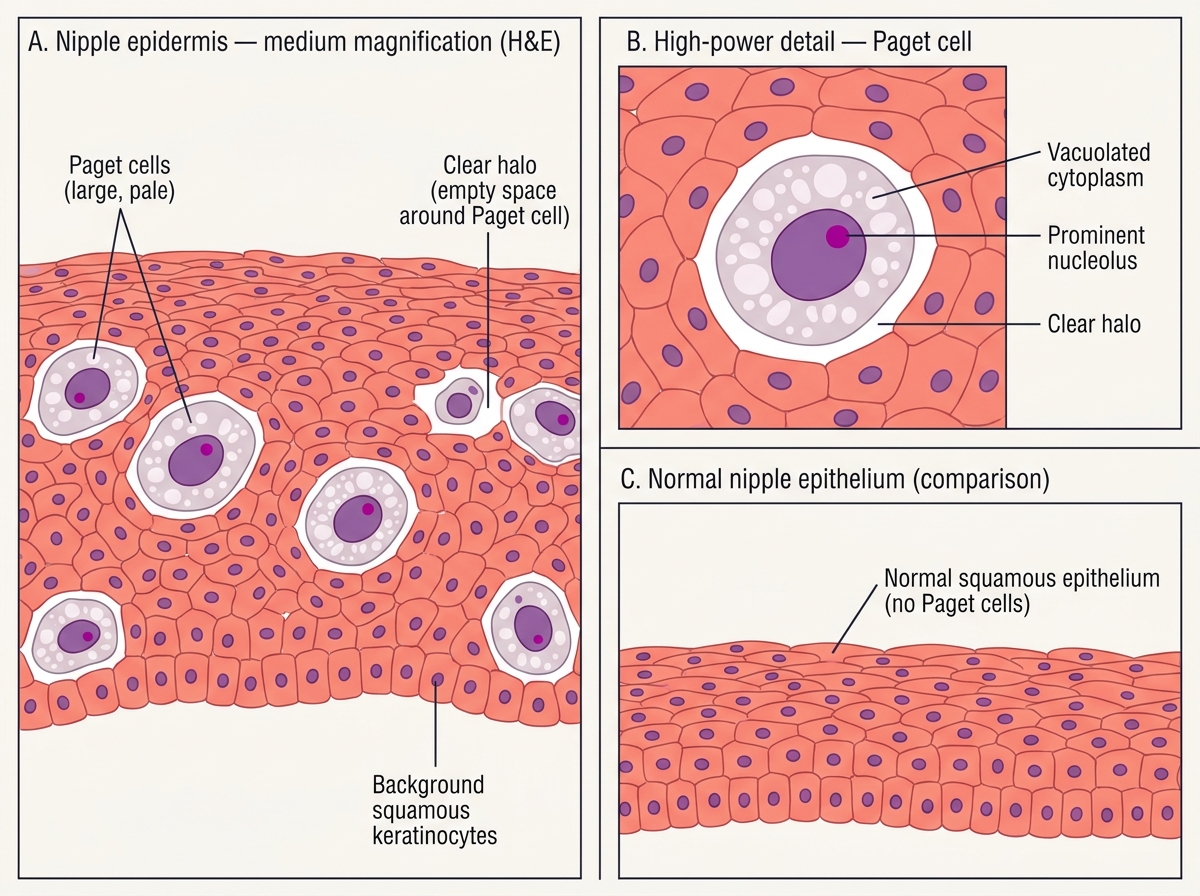
Histology of Paget Disease of the Nipple
SELF-CHECK
A 60-year-old woman presents with a 3-week history of erythema, warmth, and oedema of the entire right breast with peau d'orange skin change. Skin punch biopsy shows tumour cell emboli in dermal lymphatics. What is the minimum TNM T-stage for this lesion?
A. T1 (tumour ≤2 cm)
B. T2 (tumour 2–5 cm)
C. T3 (tumour >5 cm)
D. T4d (inflammatory carcinoma)
Reveal Answer
Answer: D. T4d (inflammatory carcinoma)
Inflammatory carcinoma with dermal lymphatic invasion is classified as T4d regardless of tumour size. This places it at Stage IIIB minimum. The defining histological requirement is tumour cell emboli in dermal lymphatics — the clinical syndrome alone (erythema + peau d'orange) is insufficient without biopsy confirmation.
Molecular/Intrinsic Subtypes and IHC-Based Classification
Gene expression profiling (microarray) has identified intrinsic molecular subtypes of breast carcinoma with distinct biology, prognosis, and treatment sensitivity. In routine practice, surrogate IHC markers (ER, PR, HER2, Ki-67) approximate these subtypes.
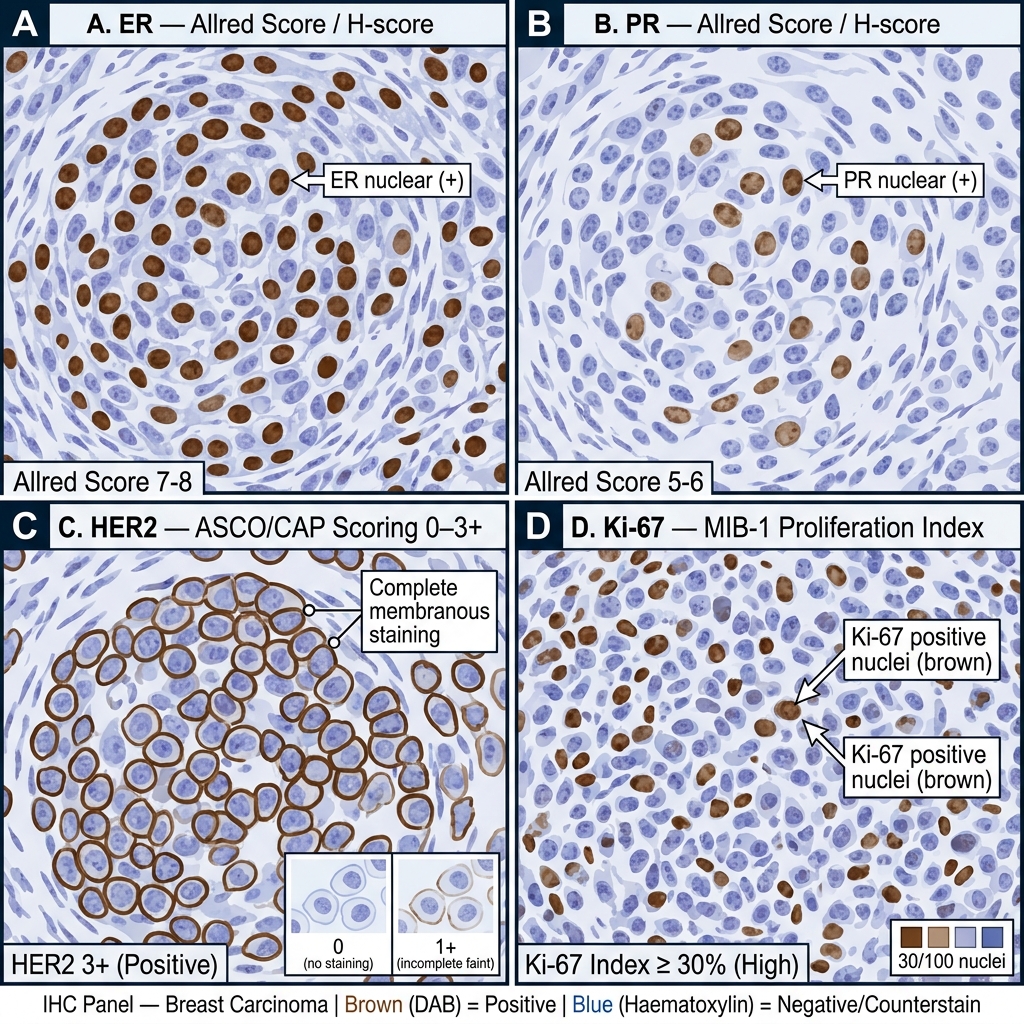
IHC Panel of Breast Carcinoma — ER, PR, HER2, and Ki-67 Expression with Scoring Methods
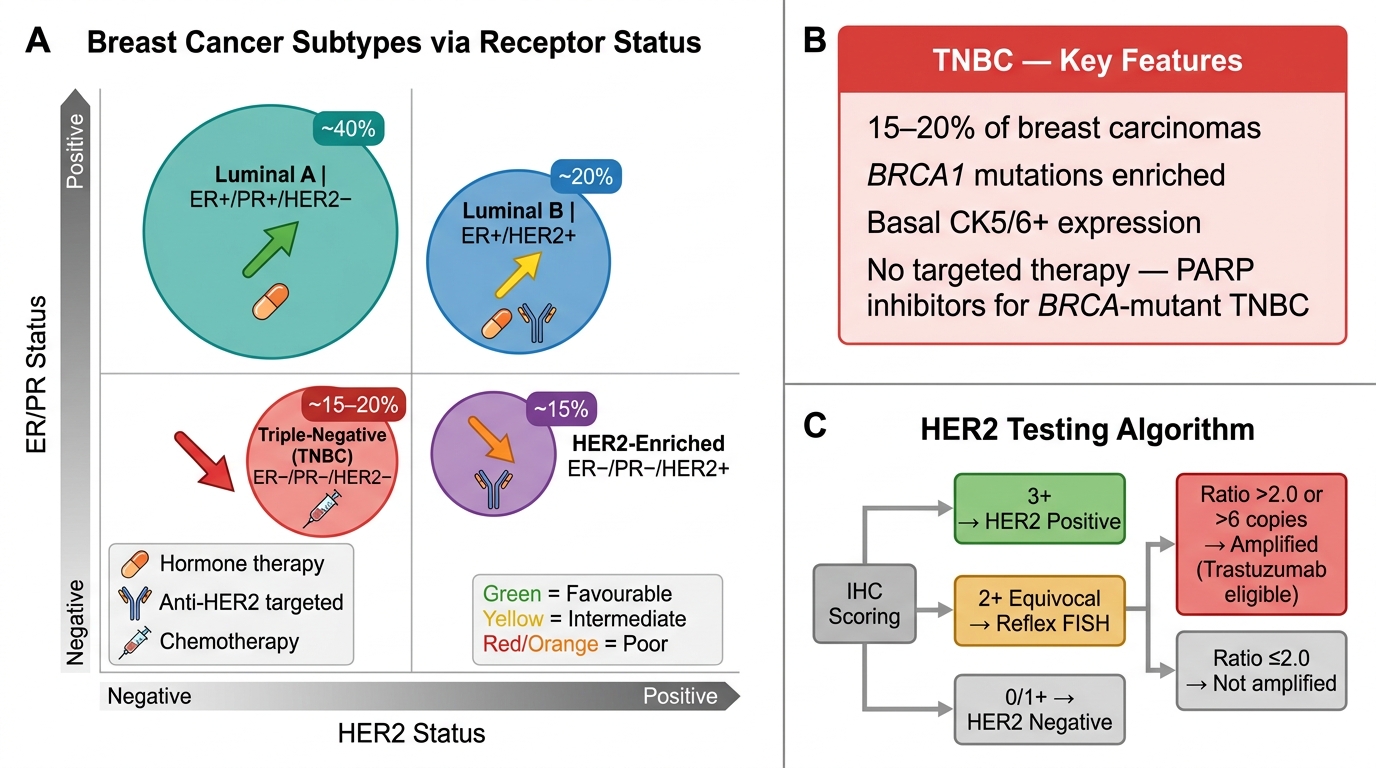
| Molecular Subtype | ER | PR | HER2 | Ki-67 | Prognosis | Treatment |
|---|---|---|---|---|---|---|
| Luminal A | + | + | − | Low (<20%) | Best | Endocrine therapy only |
| Luminal B (HER2−) | + | +/− | − | High (≥20%) | Intermediate | Endocrine + chemo |
| Luminal B (HER2+) | + | +/− | + | Any | Intermediate | Endocrine + anti-HER2 + chemo |
| HER2-enriched | − | − | + | High | Poor | Anti-HER2 + chemo |
| Basal-like / Triple-negative (TNBC) | − | − | − | High | Worst | Chemo (± PARP inhibitors if BRCA+) |
Key IHC scoring rules:
• ER/PR: Positive if ≥1% of nuclei show staining (Allred score ≥3 or ≥1% per ASCO/CAP 2020 guidelines). Positive = hormone-dependent.
• HER2: Scored 0/1+/2+/3+. 3+ (strong, complete membranous staining in >10% of cells) = positive. 2+ (equivocal) → reflex FISH/CISH for HER2 gene amplification. 0/1+ = negative.
• Ki-67: Proliferation marker (% positive nuclei). Cutoff varies (~14–20%); high Ki-67 = aggressive biology.
Molecular Subtypes of Breast Carcinoma: Classification, Prognosis, and Treatment Targets
Triple-negative breast cancer (TNBC) merits special attention:
• Comprises ~15–20% of breast carcinomas
• Highly aggressive, high proliferation, early haematogenous spread
• Enriched for BRCA1 mutations (hereditary) and basal cytokeratin expression (CK5/6+)
• No targeted therapy currently (no hormone receptor, no HER2) — but PARP inhibitors for BRCA-mutant TNBC are now standard
CLINICAL PEARL
HER2 2+ equivocal — the FISH reflex: When IHC returns HER2 2+ (equivocal), the pathologist must order reflex fluorescence in situ hybridisation (FISH). FISH counts the number of HER2 gene signals per cell (and the chromosome 17 centromere as reference). A ratio >2.0 or absolute copy number >6 signals/cell = amplified = positive. Trastuzumab is only effective in HER2-amplified tumours. This is why the case in the hook scenario required a FISH test — the IHC alone was inconclusive.