Page 8 of 19
PA30.2 | Carcinoma of the Breast — SDL Guide (Part 4)
Histological Grading: Nottingham (Bloom-Richardson) System
Histological grade is one of the strongest independent prognostic factors in breast carcinoma and is reported for every invasive carcinoma. The Nottingham Grading System (modified Bloom-Richardson) evaluates three morphological parameters, each scored 1–3.
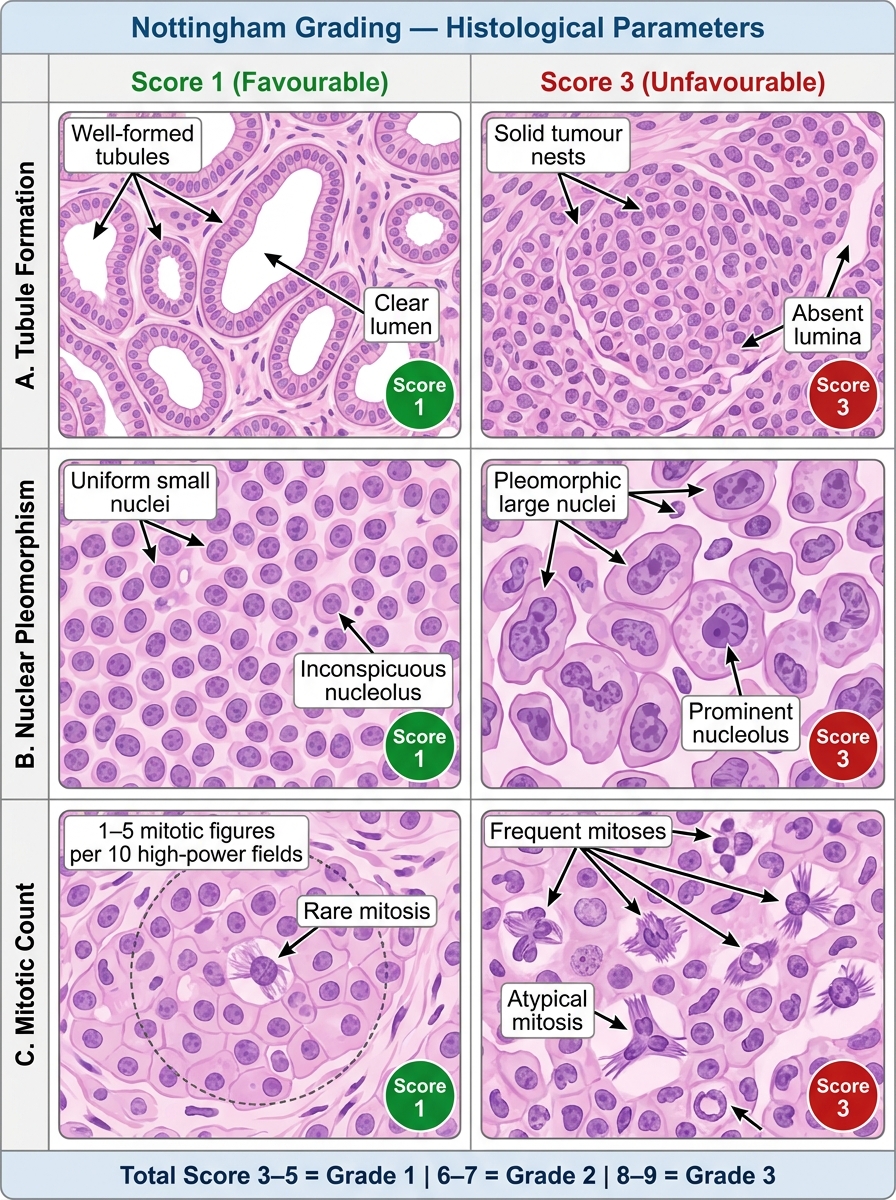
Nottingham Grading System — Composite Histological Scoring Panel
| Parameter | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| Tubule formation | >75% of tumour forms tubules | 10–75% tubules | <10% tubules |
| Nuclear pleomorphism | Uniform small nuclei (similar to normal breast nuclei) | Moderate size variation | Marked variation, prominent nucleoli |
| Mitotic count | Low (1–5 per 10 HPF) | Intermediate (6–10) | High (>10) |
HPF = high-power fields (40× objective, field diameter 0.44 mm — count must be calibrated to microscope field area)
Total score → Grade:
• 3–5 → Grade 1 (well-differentiated) — best prognosis
• 6–7 → Grade 2 (moderately differentiated) — intermediate
• 8–9 → Grade 3 (poorly differentiated) — worst prognosis
Grade correlates strongly with molecular subtype: Luminal A tumours are usually Grade 1–2; triple-negative and HER2-enriched carcinomas are almost always Grade 3. Grade is a histological parameter (not molecular) but aligns with biology.
Staging (TNM), Prognostic Factors, and Routes of Spread
TNM Staging (AJCC 8th edition — anatomic stage):
T (Primary Tumour):
• Tis — In situ (DCIS or LCIS)
• T1 — ≤2 cm (T1a ≤0.5 cm, T1b 0.5–1 cm, T1c 1–2 cm)
• T2 — >2 cm to ≤5 cm
• T3 — >5 cm
• T4 — Any size with chest wall/skin extension; T4d = Inflammatory carcinoma
N (Regional Nodes — axillary):
• N0 — No nodal metastasis
• N1 — 1–3 axillary nodes; or internal mammary node(s) by sentinel biopsy
• N2 — 4–9 axillary nodes; or internal mammary nodes clinically
• N3 — ≥10 axillary; or infraclavicular; or supraclavicular nodes
M (Distant Metastasis): M0 = absent; M1 = present → Stage IV
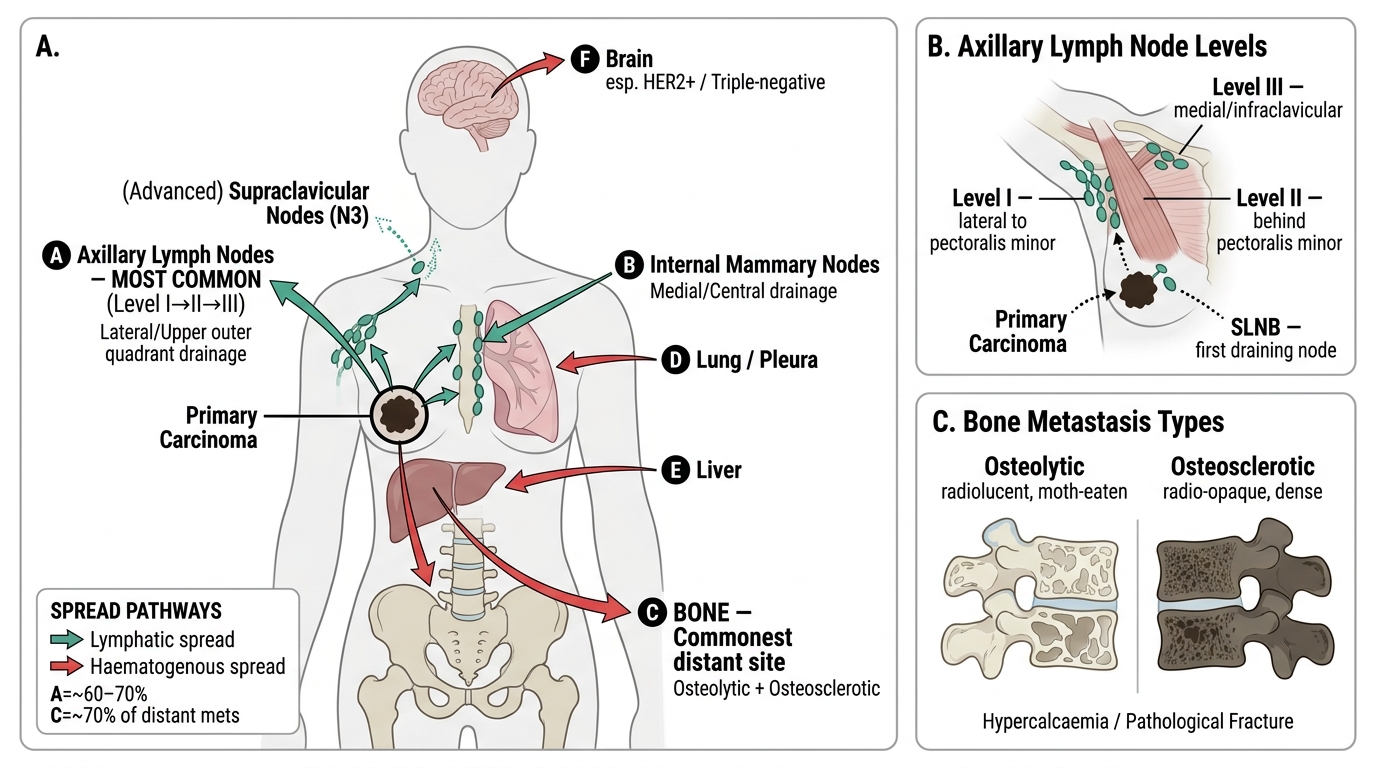
Routes of Spread of Breast Carcinoma
Routes of Spread:
Lymphatic (most important clinically):
• Axillary lymph nodes — most common; upper outer quadrant tumours → Level I/II axillary nodes
• Internal mammary nodes (medial/central tumours)
• Supraclavicular nodes (advanced disease, N3)
• Sentinel lymph node biopsy (SLNB) samples the first draining node — if negative, skip axillary dissection
Haematogenous:
• Bone — most common distant site (osteolytic or osteosclerotic; causes hypercalcaemia, pathological fracture)
• Lungs — pulmonary nodules, malignant pleural effusion
• Liver — hepatomegaly, jaundice
• Brain — particularly in HER2+ and triple-negative carcinoma (also leptomeninges in ILC)
Direct extension:
• Skin (ulceration, peau d'orange, satellite nodules)
• Chest wall (pectoral muscles, ribs) — fixation on clinical exam
• Cooper's ligament tethering → skin dimpling
• Nipple retraction (central tumours pulling lactiferous ducts)
Key Prognostic and Predictive Factors:
Prognostic (predict outcome regardless of treatment):
• Axillary nodal status — single most important prognostic factor
• Tumour size — T stage inversely correlates with survival
• Histological grade (Nottingham 1–3)
• Lymphovascular invasion (LVI) — independent predictor of nodal involvement
• Molecular subtype (Luminal A → best; TNBC → worst)
• Ki-67 proliferation index
Predictive (predict response to a specific treatment):
• ER/PR status — predicts response to tamoxifen/aromatase inhibitors
• HER2 amplification — predicts response to trastuzumab (Herceptin), pertuzumab, TDM1
• BRCA1/2 mutation — predicts response to PARP inhibitors
• PD-L1 expression — predicts response to immunotherapy (pembrolizumab in TNBC)
SELF-CHECK
A breast carcinoma shows: tubule formation 20% of tumour (score 2), moderately pleomorphic nuclei (score 2), and 8 mitoses per 10 HPF (score 2). What is the Nottingham grade and total score?
A. Score 6, Grade 2 (moderately differentiated)
B. Score 7, Grade 2 (moderately differentiated)
C. Score 8, Grade 3 (poorly differentiated)
D. Score 5, Grade 1 (well-differentiated)
Reveal Answer
Answer: A. Score 6, Grade 2 (moderately differentiated)
Tubule score 2 + nuclear score 2 + mitotic score 2 = total 6. Score 6–7 = Nottingham Grade 2 (moderately differentiated). Note: mitoses 6–10/10 HPF = score 2, which fits '8 per 10 HPF'. Total score 6 is the lower end of Grade 2.