Page 10 of 19
PA30.{3,5} | Phyllodes Tumor & Breast Morphology — SDL Guide
Learning Objectives
- Describe and distinguish the gross and microscopic features of phyllodes tumor from fibroadenoma.
- Grade phyllodes tumor as benign, borderline, or malignant using the WHO criteria (stromal cellularity, atypia, mitoses, margins, stromal overgrowth).
- Systematically identify key breast lesions — both benign and malignant — from gross photographs and microscopic images in a practical exam context.
- Distinguish DCIS from invasive carcinoma and fibroadenoma from phyllodes tumor — the two most commonly tested practical-exam distinctions.
- Recognise the characteristic microscopic pattern of each major breast carcinoma subtype: invasive ductal NST, invasive lobular, mucinous, medullary, tubular, and Paget disease.
- Correlate gross and microscopic appearances with clinical behavior and prognosis.
INSTRUCTIONS
This is the morphology-consolidation SDL for the PA Systemic Pathology — Breast cluster. You will encounter breast pathology specimens in your practical exams AND in clinical postings (both surgery and pathology). The ability to name and describe a gross or microscopic slide is a core MBBS Year-2 skill. Work through this SDL with your histology atlas open. Every IMAGE_NEEDED marker signals a slide or photograph you should find, examine, and be able to describe in a viva — 'I see leaf-like fronds of stroma projecting into cyst-like spaces, with a hypercellular, moderately pleomorphic stroma' is the quality of answer expected.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 23 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old woman walks into your surgery outpatient clinic with a lump she noticed 3 months ago. The lump has grown visibly in the last 6 weeks. On examination it is 8 cm, smooth-surfaced, firm-to-rubbery, and moves freely. The resident beside you says, 'Probably just a fibroadenoma — she's young.' But something nags at you: fibroadenomas don't grow this fast. You send her for an excision biopsy. The histopathology report arrives: 'Leaf-like epithelial-lined clefts separated by hypercellular stroma. Mitoses: 4 per 10 HPF. Margins: infiltrative. No heterologous elements. Diagnosis: Phyllodes tumor, borderline.' One word on that report — borderline — changes the surgical plan entirely. Why? Because benign phyllodes gets a 1 cm clear margin, borderline gets a 2 cm margin, and malignant may need mastectomy. Knowing how to read the pathology of breast lumps is not an exam trick — it changes what happens to your patient on the operating table.
WHY THIS MATTERS
PA30.3 and PA30.5 are directly assessed in your practical exams (slide identification and description), in the theory paper (short-answer morphology questions), and in clinical postings in surgery and pathology. Beyond exams: India has a high burden of breast disease — fibroadenoma is the commonest breast lump in young Indian women, and breast carcinoma is now the most common cancer in Indian women (overtaking cervical carcinoma in urban centres). You will encounter these slides, these reports, and these patients throughout your career. This SDL is deliberately image-heavy because pattern recognition — not just naming — is what makes you clinically useful.
RECALL
From SDL1 (Breast Benign Diseases) you know: fibroadenoma is a benign biphasic tumor (epithelium + stroma), most common in women 15–35 years. From SDL2 (Breast Carcinoma) you know: DCIS is in-situ malignancy confined to ducts by the basement membrane; invasive carcinoma NST (no special type) is the commonest invasive cancer; ER/PR/HER2 status drives treatment. You also know that fibrocystic change, intraductal papilloma, and sclerosing adenosis are benign lesions that may mimic malignancy on imaging. This SDL builds on both — it adds phyllodes tumor as a distinct fibroepithelial entity, and then systematically walks through all breast lesions for practical identification.
Phyllodes Tumor: Concept and Distinction from Fibroadenoma
Phyllodes tumor (from Greek phyllon = leaf) is a fibroepithelial neoplasm of the breast, closely related to fibroadenoma but biologically distinct. The name captures its defining architectural feature: leaf-like stromal fronds lined by epithelium projecting into cyst-like spaces, creating a bulging, lettuce-leaf cross-section on gross examination.
Why it is NOT a fibroadenoma — the key distinctions:
| Feature | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Age peak | 15–35 years | 40–50 years (older) |
| Size | Usually < 3 cm | Often > 4 cm; can reach 20+ cm |
| Growth rate | Slow, static | Often rapid (weeks to months) |
| Gross architecture | Firm, rubbery, lobulated | Bulging cystic spaces, leaf-like cross-section |
| Stromal cellularity | Low (fibrous, hypocellular) | High — the hallmark |
| Stromal atypia | None | Variable (grades benign/borderline/malignant) |
| Mitoses | Absent or rare | Graded (see below) |
| Margins | Pushing (well-defined) | Variable — pushing → infiltrative |
| Behavior | Benign; recurrence rare | Local recurrence; rare metastasis in malignant grade |
| Treatment | Enucleation acceptable | Wide local excision — margin width determines grade |
The mnemonic: PhyLLodes = Leaf-Like, Larger, Later in life, Less well-behaved than fibroadenoma.
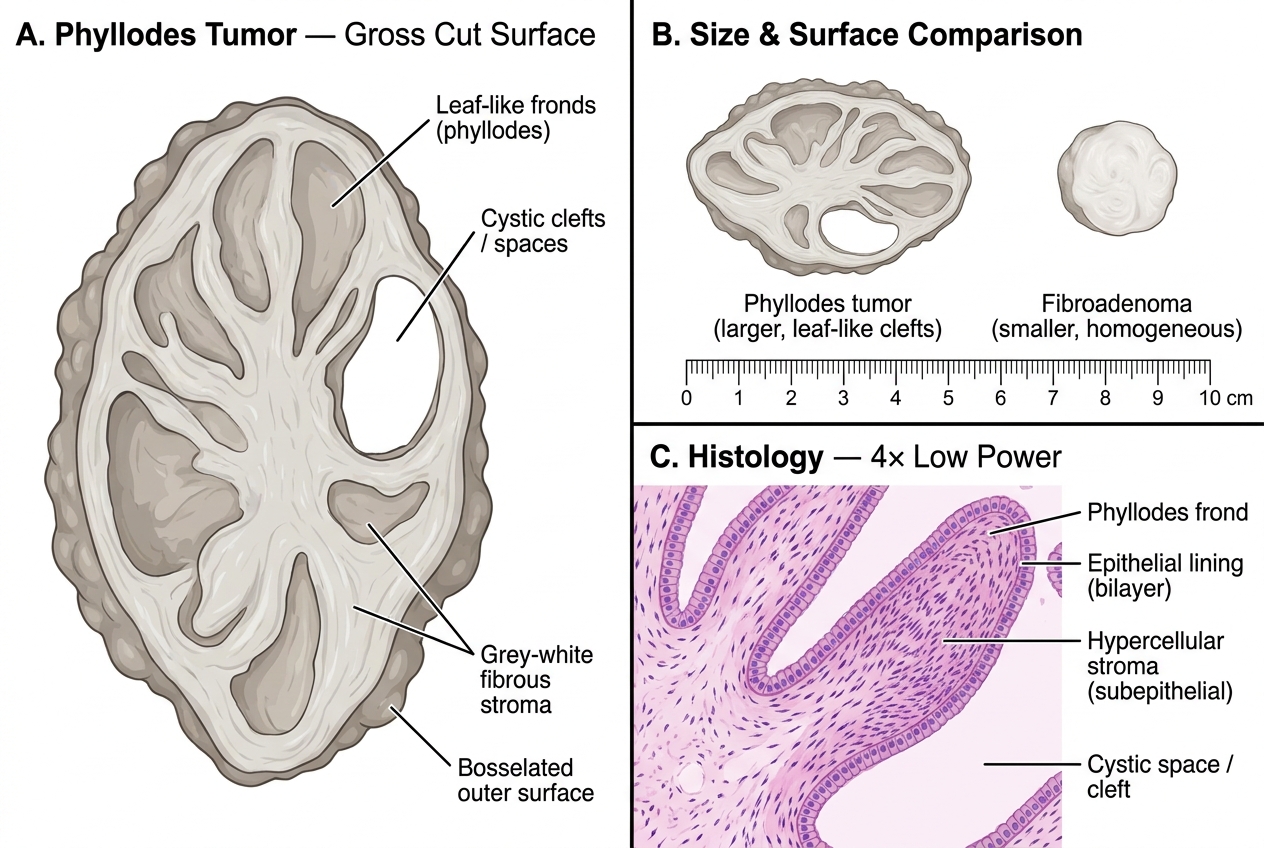
Phyllodes Tumor — Gross Morphology, Size Comparison with Fibroadenoma, and Low-Power Histology
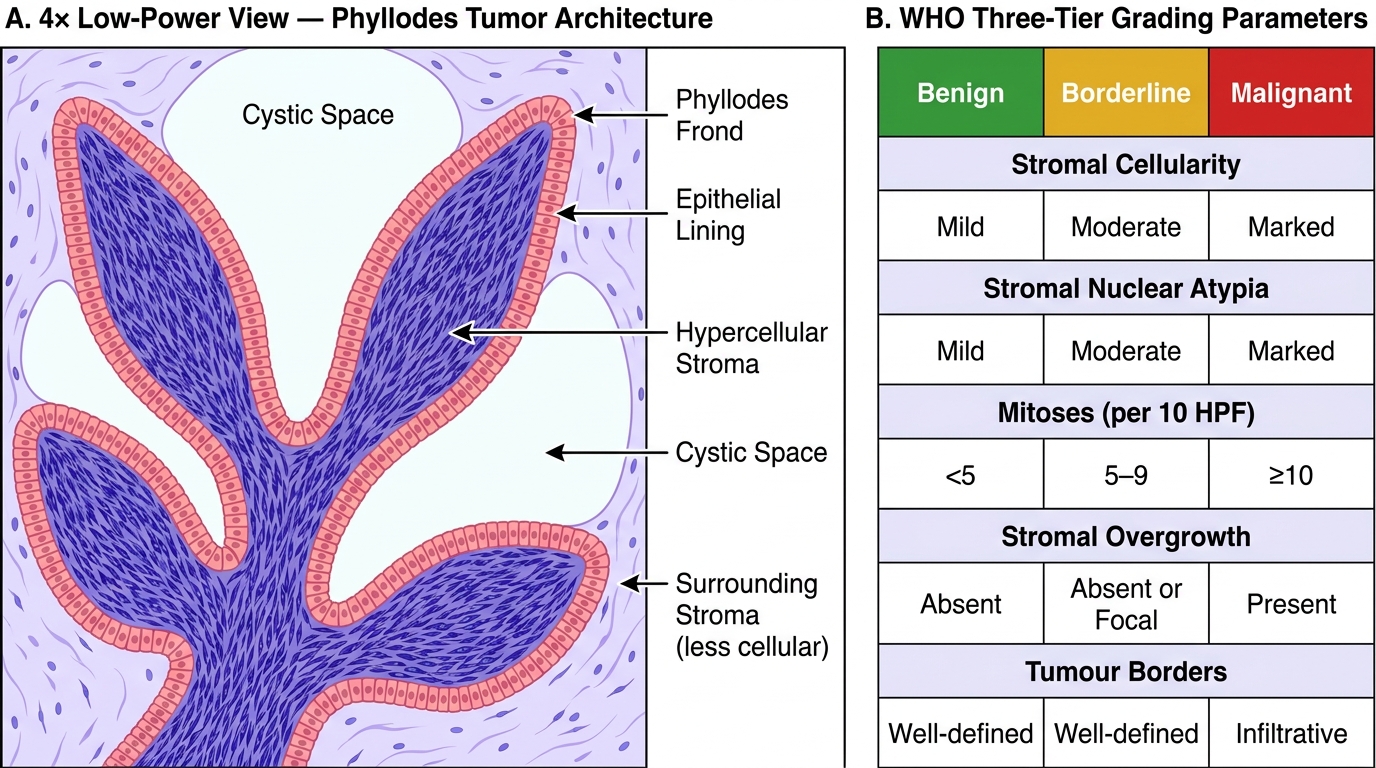
Phyllodes Tumor — Histological Architecture and WHO Grading
Grading Phyllodes Tumor: WHO Three-Tier System
The WHO grades phyllodes tumor into benign, borderline, and malignant based on five histological parameters. You must know all five and their cut-offs — this is a commonly tested short-answer question.
The Five Grading Parameters:
| Parameter | Benign | Borderline | Malignant |
|---|---|---|---|
| Stromal cellularity | Mild | Moderate | Marked |
| Stromal nuclear atypia | Mild | Moderate | Marked |
| Mitoses (per 10 HPF) | < 5 | 5–9 | ≥ 10 |
| Tumor margins | Well-defined (pushing) | Variable | Infiltrative |
| Stromal overgrowth | Absent | Absent | Present |
Stromal overgrowth — the most serious finding, and one students often miss. It is defined as stroma that has completely replaced the epithelial component in at least one 4× field. When stroma overgrows the epithelium, it is behaving like a pure sarcoma — this is the feature most strongly associated with distant metastasis.
Heterologous elements may appear in malignant phyllodes: the stroma can differentiate into liposarcoma, rhabdomyosarcoma, chondrosarcoma, or osteosarcoma. Their presence immediately upgrades the lesion to malignant regardless of the mitotic count.
Clinical behavior and management:
- Benign (75% of cases): local recurrence in 10–17%; no distant metastasis. Wide excision with 1 cm clear margins.
- Borderline (10–15%): local recurrence in 15–25%; rare metastasis. Wide excision with 2 cm clear margins.
- Malignant (10%): local recurrence in 20–30%; distant metastasis in 10–22% (lungs most common — haematogenous, NOT lymphatic like carcinoma). Simple mastectomy often required. Note: axillary dissection is NOT routinely done because lymphatic spread is rare.
Key exam point: Phyllodes tumor metastasizes haematogenously; breast carcinoma metastasizes lymphatically first. This is why sentinel node biopsy is done for carcinoma but NOT for phyllodes.
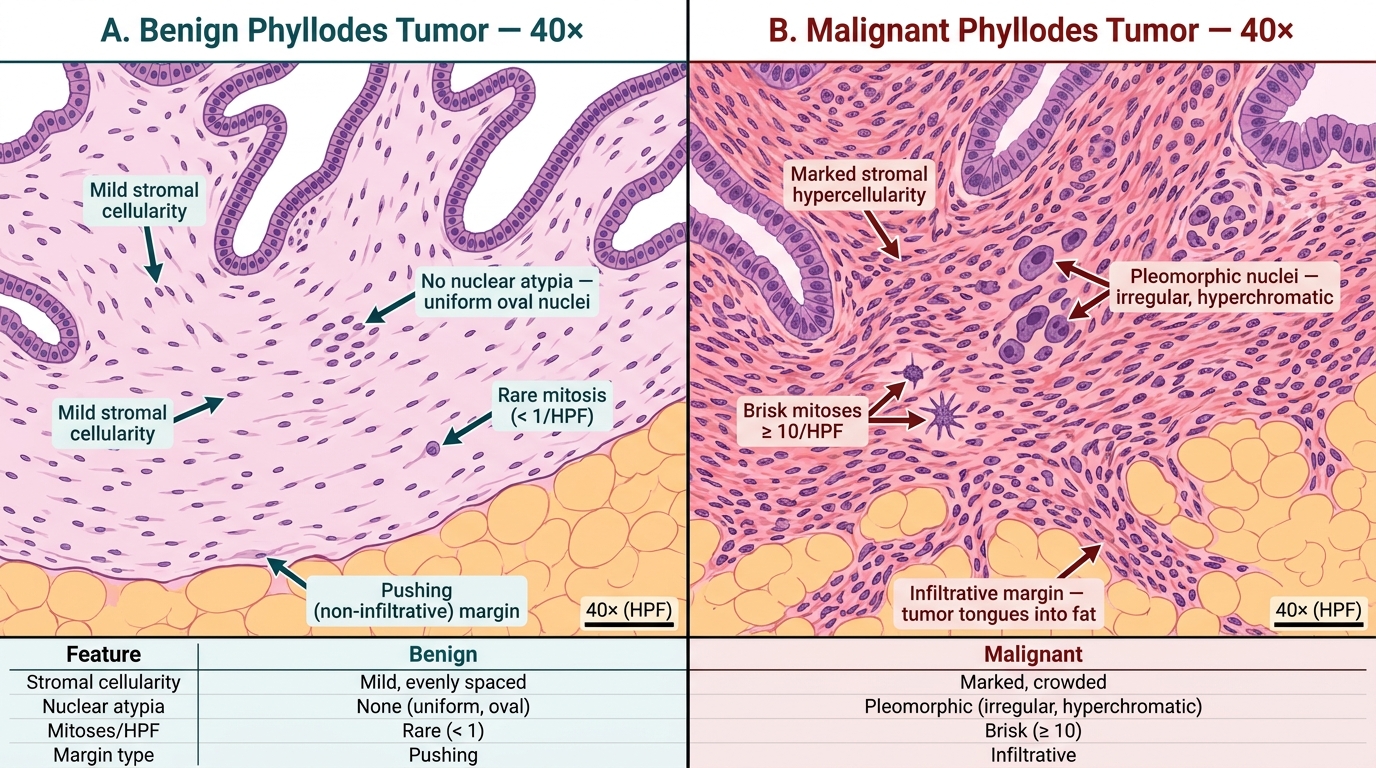
Phyllodes Tumor Grading: Benign vs Malignant — High-Power (40×) Histology Comparison
CLINICAL PEARL
The rapid growth red flag: Any 'fibroadenoma' that grows rapidly in an older woman (> 35 years) should be biopsied and NOT assumed benign. Core needle biopsy of a phyllodes tumor shows the characteristic hypercellular stroma but cannot reliably grade the lesion — excision with margin assessment is required for definitive grading. Leaving a positive margin in a phyllodes tumor (even benign grade) is associated with a 3× increase in local recurrence rate. The surgeon and pathologist must communicate clearly about margin adequacy — this is a joint responsibility.
Practical Morphology: Gross Appearances of Key Breast Lesions
In the practical exam you may be given a gross specimen (usually fixed in formalin) or a photograph. The following is a systematic walk-through of what to look for and what to say.
Fibroadenoma (gross):
Well-circumscribed, encapsulated nodule, 1–3 cm, firm, rubbery, grey-white cut surface with a slightly whorled or lobulated pattern. Glistening surface that bulges above the cut margin. No necrosis. Mobile from surrounding breast tissue (this is why it is called a 'breast mouse' clinically — it slips away from the examining finger).
Fibrocystic change (gross):
Diffuse, bilateral, poorly-defined thickening. Cut section shows multiple small cysts (blue-domed, fluid-filled, up to 3 cm — the Bloodgood blue-domed cysts) set within fibrous stroma. No discrete mass. Rubbery to firm areas of fibrosis.
Intraductal papilloma (gross):
Small (< 1 cm) friable, warty, pink-red intraluminal growth within a dilated duct, usually beneath the nipple-areola complex. The duct may be dilated and contain serosanguineous fluid. The nipple discharge (serous or bloody) is the clinical clue.
DCIS (gross):
May be invisible on gross examination (especially low-grade). High-grade DCIS (comedo type) may show toothpaste-like necrotic material that can be expressed from duct cross-sections — this is called comedonecrosis. Microcalcifications may be visible as white gritty foci on cut section (and are the basis for the mammographic finding).
Invasive ductal carcinoma NST (gross):
The classic gross appearance: irregular, stellate, gritty, grey-white mass with hard consistency (like unripe pear). The spiculated edges are due to the dense desmoplastic stroma. Skin puckering and nipple retraction result from the fibrous retraction through Cooper's ligaments. Cut section reveals the gritty texture (calcification within the desmoplastic stroma).
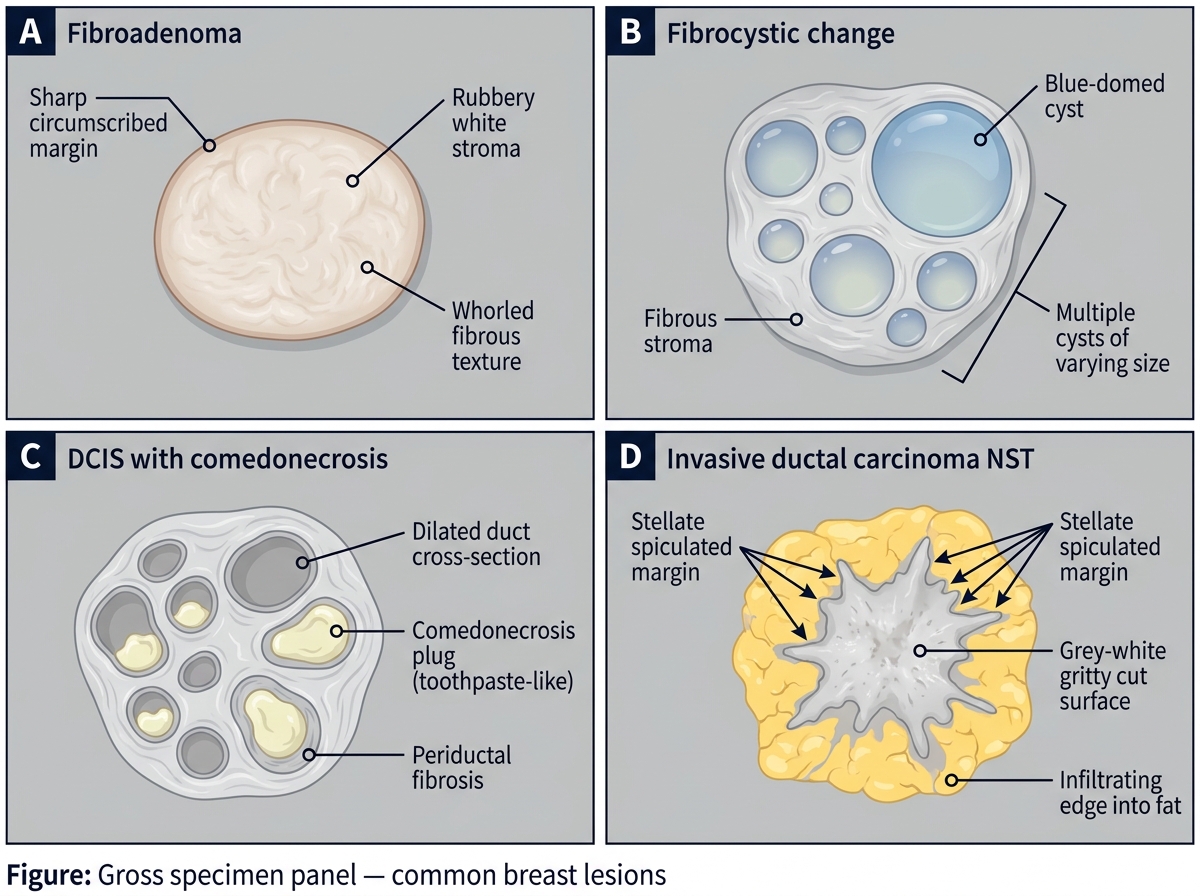
Gross Specimen Panel: Common Breast Lesions
Inflammatory carcinoma (gross):
No discrete mass — the entire breast is indurated, red, warm, and edematous. The skin has the appearance of peau d'orange (orange-peel skin) due to lymphatic obstruction causing subcutaneous lymphedema. This is NOT an inflammatory condition — it is a carcinoma with dermal lymphatic invasion. Diagnosis is often clinical (T4d staging); skin punch biopsy confirms dermal lymphatic tumor emboli.
Paget disease of the nipple (gross):
Erythematous, eczematous, crusted nipple-areola lesion. Always associated with underlying DCIS or invasive carcinoma. The nipple is the entry point — Paget cells migrate from the underlying malignancy through the ductal system to the epidermis of the nipple.
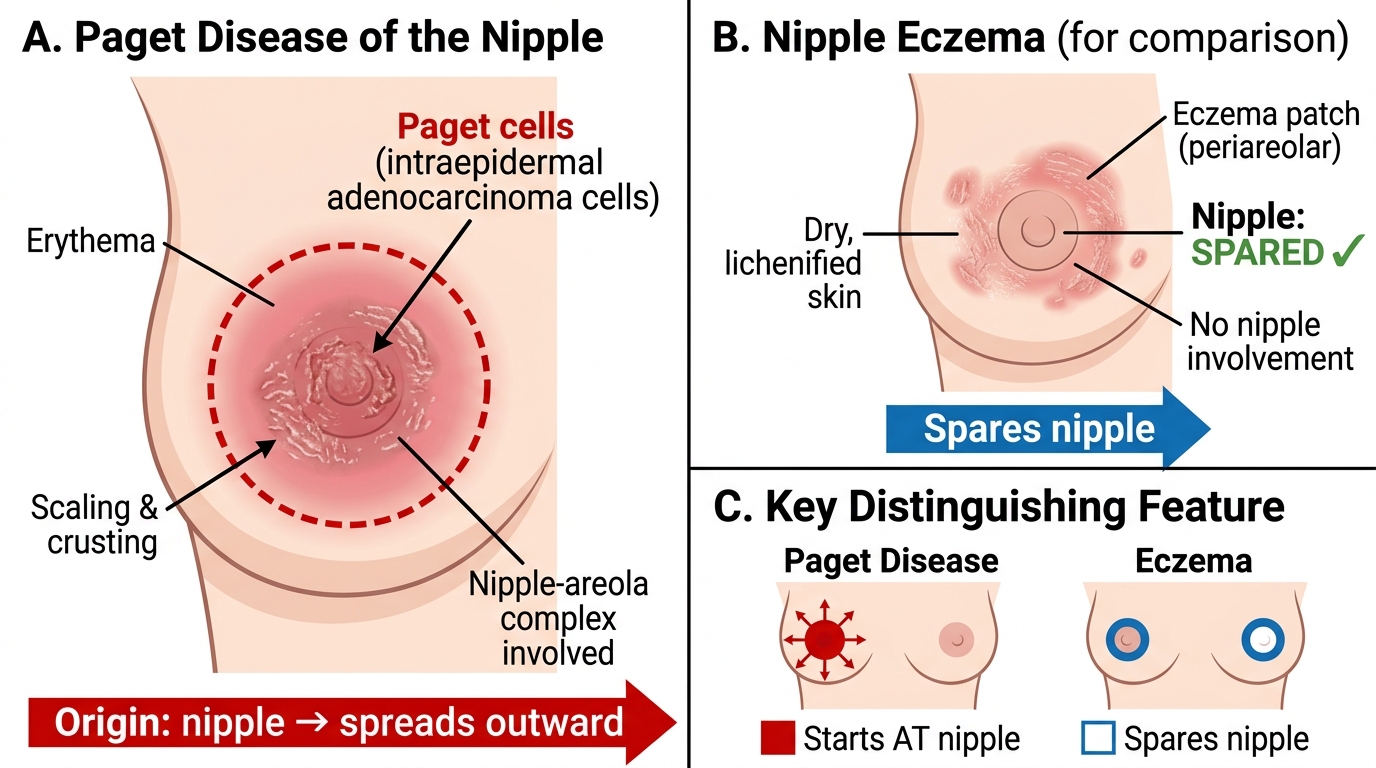
Paget Disease of the Nipple vs Nipple Eczema — Clinical Features and Distribution