Page 11 of 19
PA30.{3,5} | Phyllodes Tumor & Breast Morphology — SDL Guide (Part 2)
Microscopic Morphology Part 1 — Benign Lesions
Fibroadenoma (microscopy):
Two architectural patterns co-exist:
- Intracanalicular pattern: Proliferating stroma compresses the ducts into irregular slit-like spaces — the ducts appear as curvilinear clefts in a fibrous background.
- Pericanalicular pattern: Stroma grows around the ducts, which remain open and rounded.
Critical teaching point: the stroma in fibroadenoma is loose, myxoid, hypocellular (it looks like a sparse, pale background with scattered spindle cells). This is what distinguishes it from phyllodes at a glance.
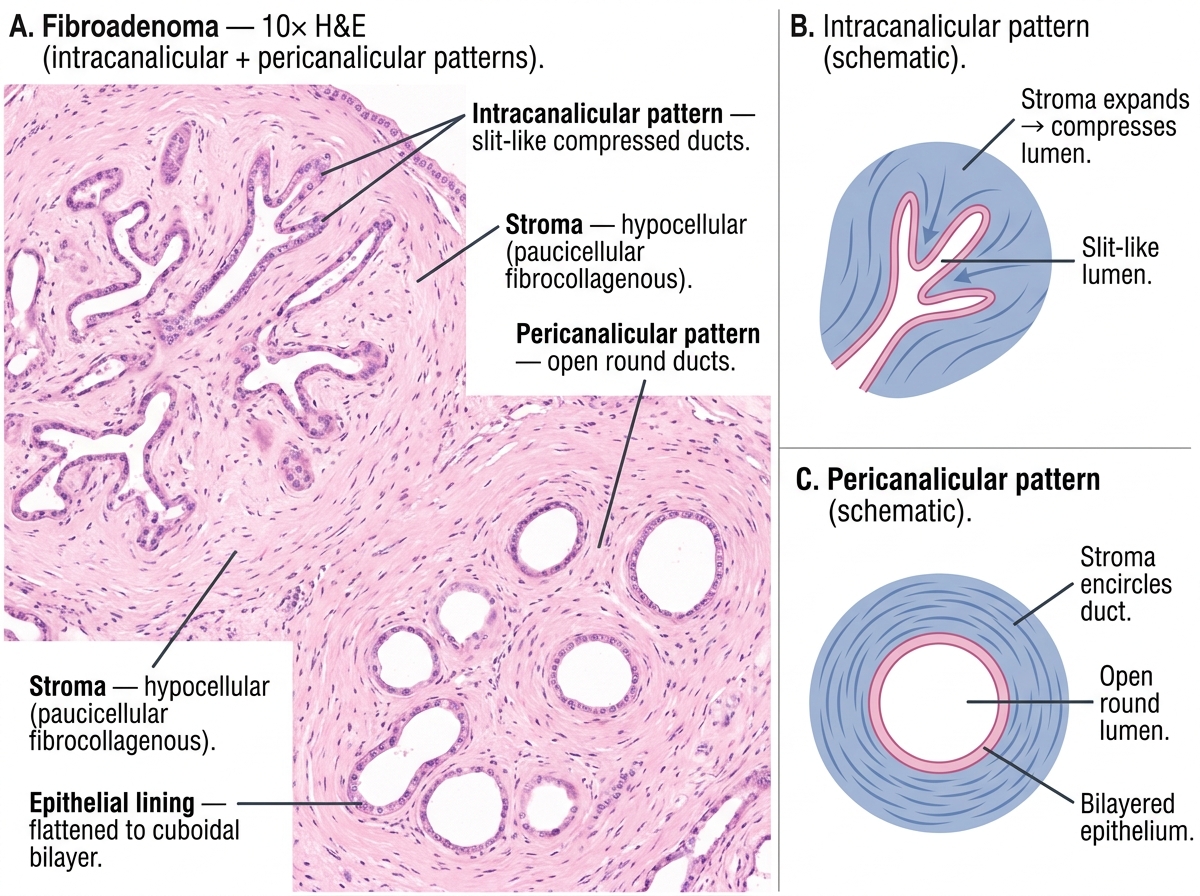
Fibroadenoma — Histological Patterns (10×): Intracanalicular vs. Pericanalicular
Fibrocystic change (microscopy):
Three key components, all often present together:
1. Cysts — dilated ducts and acini lined by flattened (atrophic) or apocrine epithelium. Apocrine metaplasia (cells with abundant pink granular cytoplasm and apical snouts — decapitation secretion) is the hallmark.
2. Fibrosis — increased stromal collagen.
3. Epithelial hyperplasia — increased layers of epithelial cells within ducts. When hyperplasia shows nuclear atypia, it is called atypical ductal hyperplasia (ADH) — a precursor lesion.
Intraductal papilloma (microscopy):
Fibrovascular core (stalk of connective tissue with a central capillary) lined by two layers of cells — inner epithelial and outer myoepithelial. The preserved myoepithelial layer is critical — it is absent in invasive carcinoma. The branching architecture creates a tree-like structure within the duct lumen.
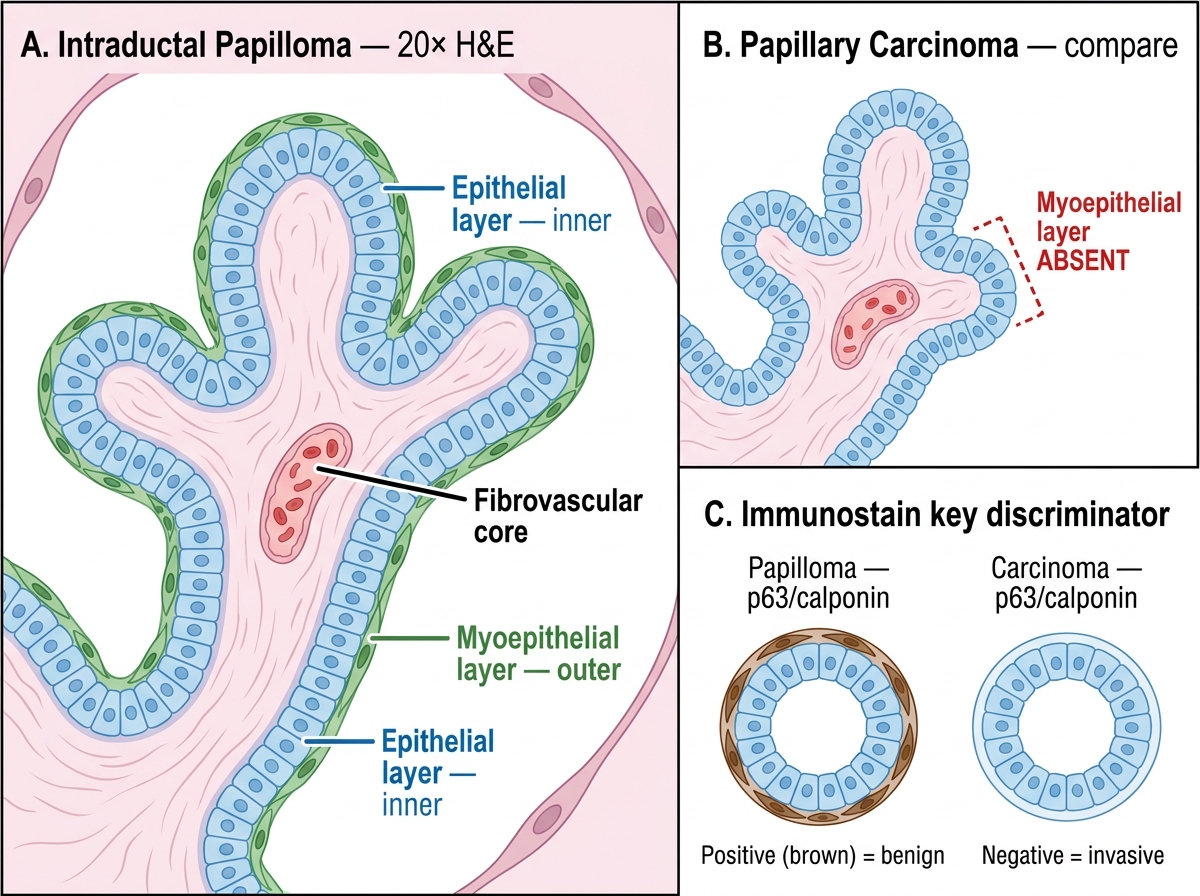
Intraductal Papilloma vs Papillary Carcinoma — Histology and Immunostain
Sclerosing adenosis (microscopy):
Loose glands of increased number, preserved architecture but compressed and distorted by perilobular fibrosis. May mimic carcinoma. Key discriminator: myoepithelial cells are preserved (immunostain for p63 or calponin positive in benign, negative in invasive carcinoma).
Microscopic Morphology Part 2 — DCIS and LCIS
DCIS (ductal carcinoma in situ):
Malignant epithelial cells confined to the duct-lobular system by an intact basement membrane. The basement membrane is the fence — if it is breached, the lesion is by definition invasive. Myoepithelial cells are still present (a useful immunohistochemical marker).
Grades of DCIS:
- Low-grade DCIS: Small, uniform, monomorphic cells filling the duct in solid, cribriform (sieve-like) or micropapillary patterns. No necrosis. Low nuclear grade (nuclei < 1.5× RBC diameter).
- High-grade (comedo) DCIS: Large, pleomorphic cells with central necrosis occupying the duct lumen — this necrosis calcifies and is seen as linear/branching microcalcifications on mammography. The pattern is called comedo because the expressed necrotic material resembles a comedo (blackhead).
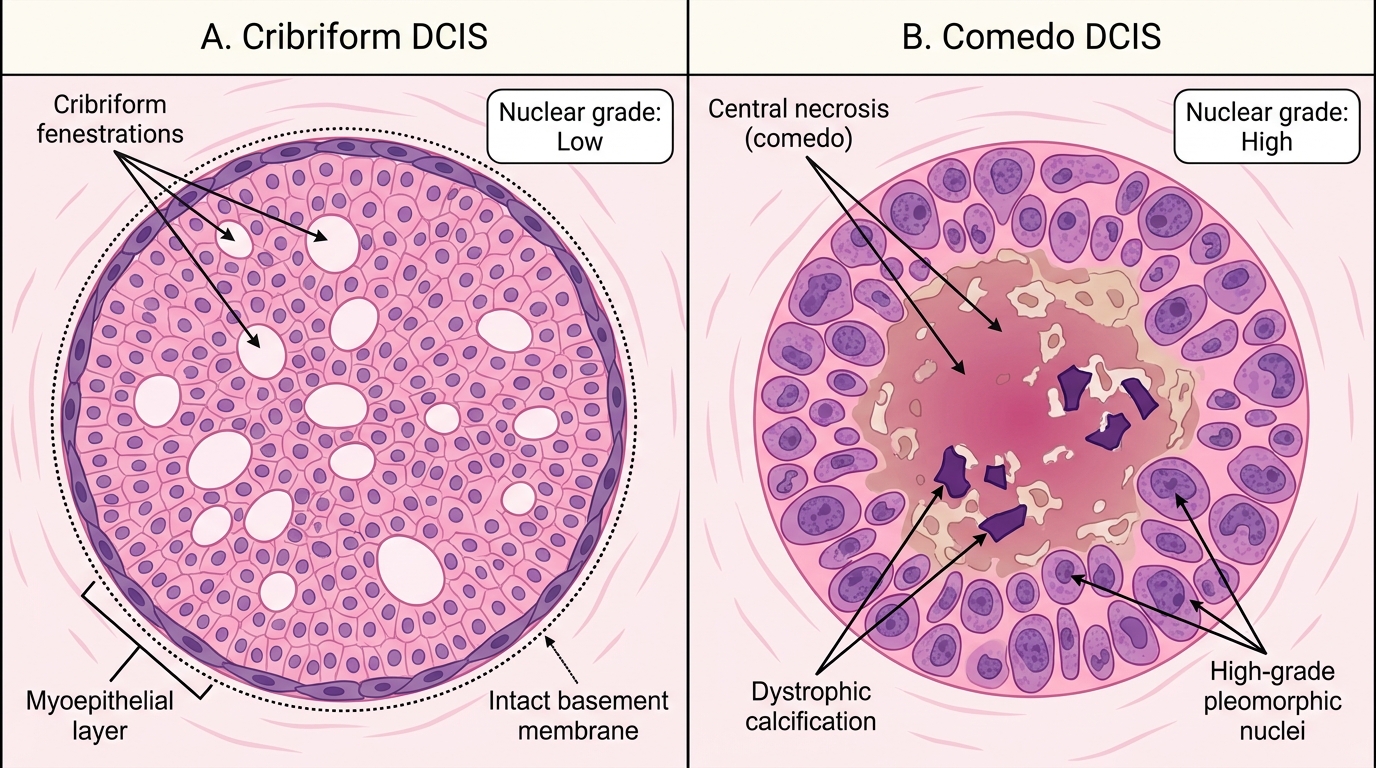
DCIS Subtypes: Cribriform vs Comedo Patterns (H&E, 10×)
The most important distinction in breast pathology: DCIS vs Invasive carcinoma:
- DCIS: duct rounded, intact outer contour, myoepithelial layer present, basement membrane intact on PAS/laminin stain.
- Invasive carcinoma: irregular nests and cords infiltrating the stroma, no surrounding myoepithelial layer, basement membrane absent, stromal desmoplasia.
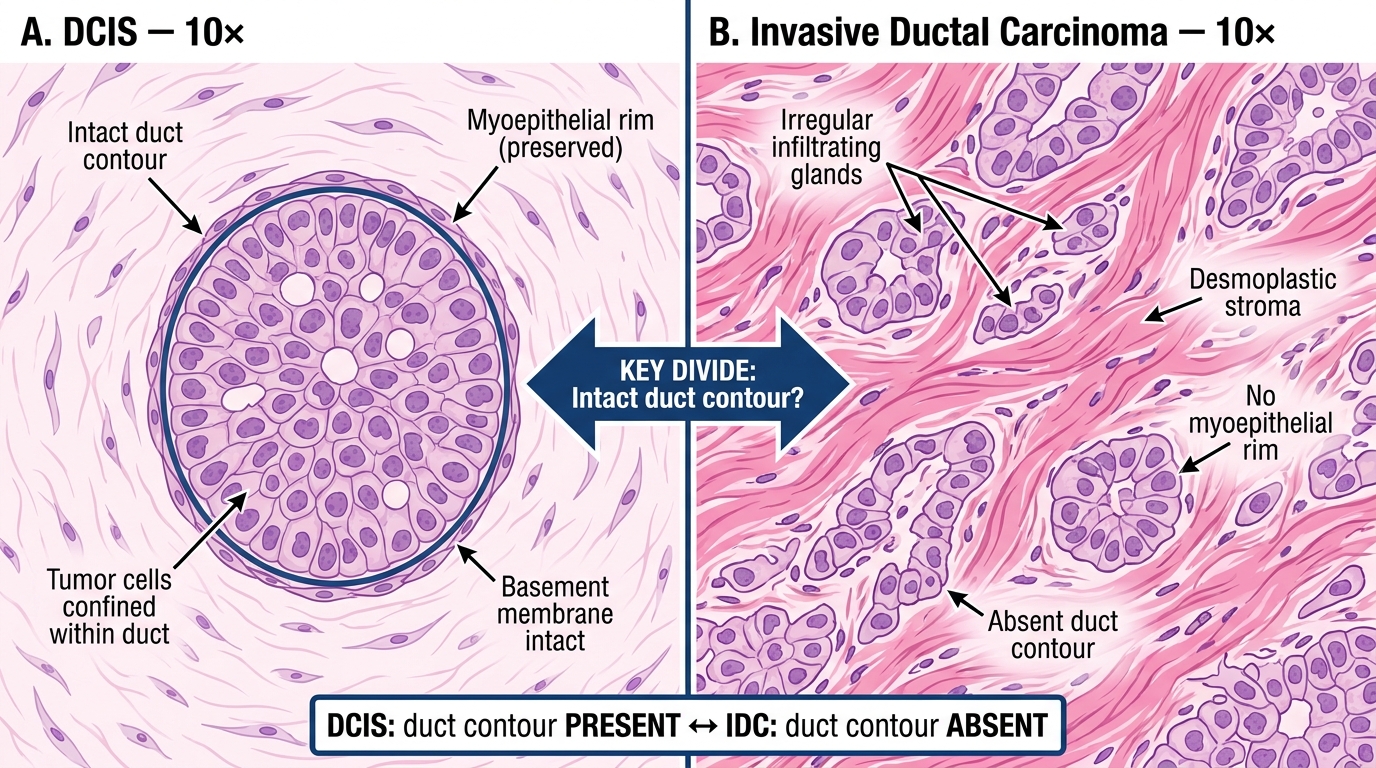
DCIS vs Invasive Ductal Carcinoma — Medium Power (10×) Comparison
LCIS (lobular carcinoma in situ):
Uniform, discohesive small, round cells distending the acini of the terminal duct-lobular unit. The cells lack E-cadherin (a cell-adhesion molecule) — this is what makes them discohesive and is the basis of the IHC stain that distinguishes LCIS/ILC from ductal lesions. No necrosis. No microcalcifications. LCIS is a risk marker (bilateral risk of invasive cancer, 8–10× baseline) not a direct precursor like DCIS.
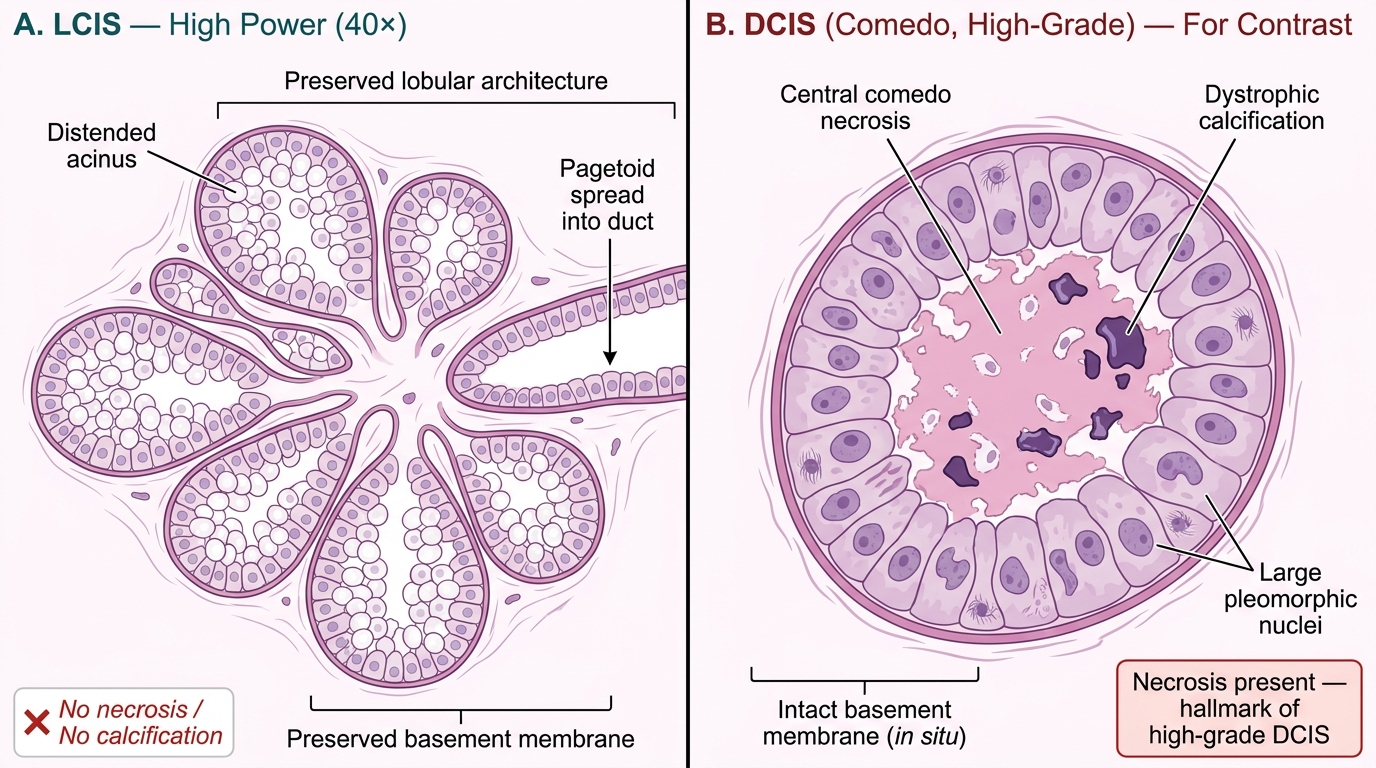
LCIS vs. High-Grade Comedo DCIS — Comparative High-Power Histology (40×)
SELF-CHECK
A biopsy shows tumor cells confined within a duct with central necrosis, calcification, and large pleomorphic nuclei. The basement membrane is intact. Which diagnosis and grade does this BEST represent?
A. Low-grade cribriform DCIS
B. High-grade (comedo) DCIS
C. LCIS with comedonecrosis
D. Invasive ductal carcinoma with central necrosis
Reveal Answer
Answer: B. High-grade (comedo) DCIS
The key features are: (1) confined to the duct — basement membrane intact, so it is in situ (not invasive); (2) central necrosis and calcification — the hallmark of comedo (high-grade) DCIS; (3) large pleomorphic nuclei — high nuclear grade. LCIS does not show necrosis. Invasive carcinoma would have infiltrating nests in stroma without an intact duct outline.
Microscopic Morphology Part 3 — Invasive Carcinomas
Invasive ductal carcinoma NST (no special type) — the most common:
Irregular nests, cords, and solid sheets of pleomorphic cells infiltrating a dense desmoplastic stroma. Desmoplasia (from Greek desmos = binding) is the reactive fibrosis induced by the invasive tumor — it gives the carcinoma its hard, gritty feel on gross examination. At high power: nuclear pleomorphism, prominent nucleoli, mitoses (grade dependent). No special architectural features — that is what 'no special type' means.
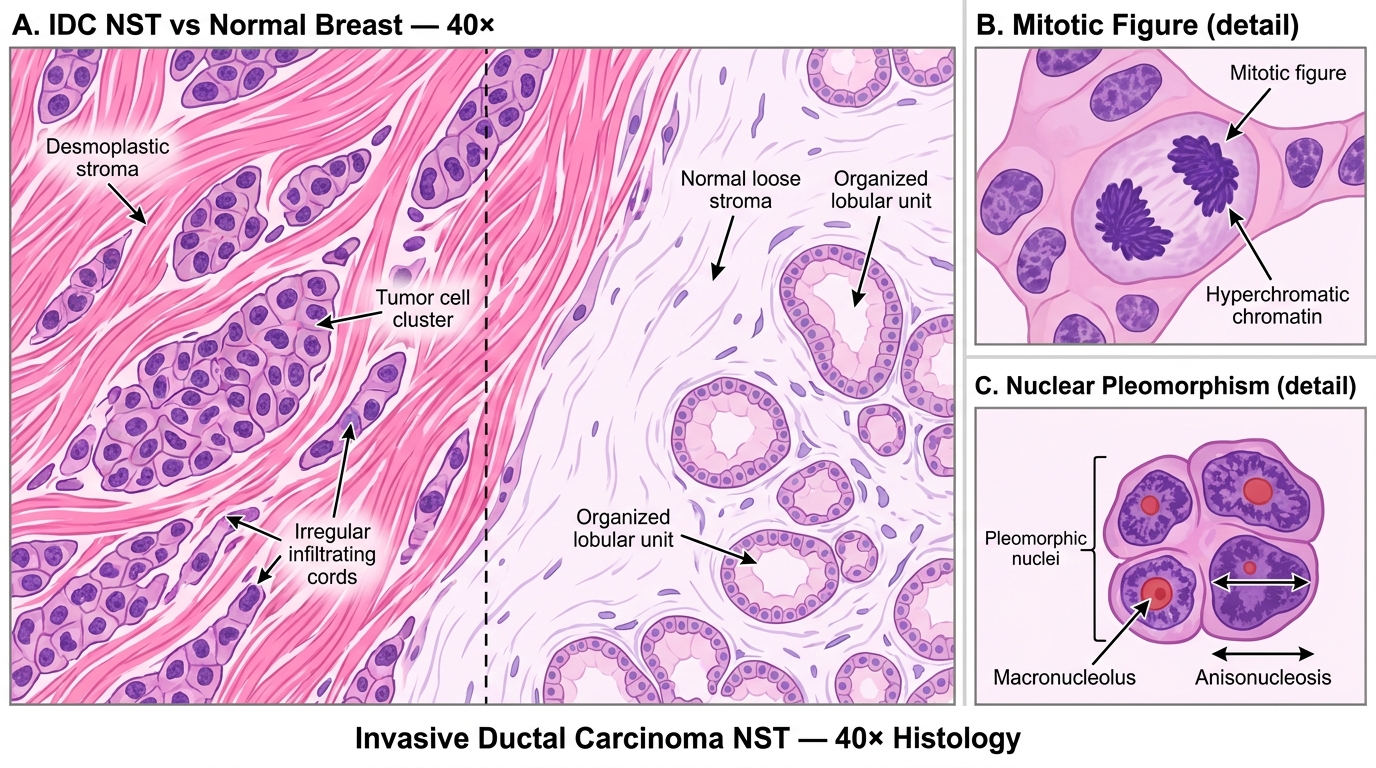
Invasive Ductal Carcinoma NST — High-Power Histology (40×)
Invasive lobular carcinoma (ILC) — the single-file pattern:
The pathognomonic feature: tumor cells infiltrate singly or in single-file linear cords (Indian file / single-file pattern) through the stroma. Cells are small, uniform, discohesive (same E-cadherin loss as LCIS). Because they do not form a solid mass and grow between normal structures, ILC can be occult on mammography. They often form a targetoid pattern around normal structures. ILC constitutes 10–15% of invasive breast cancers.
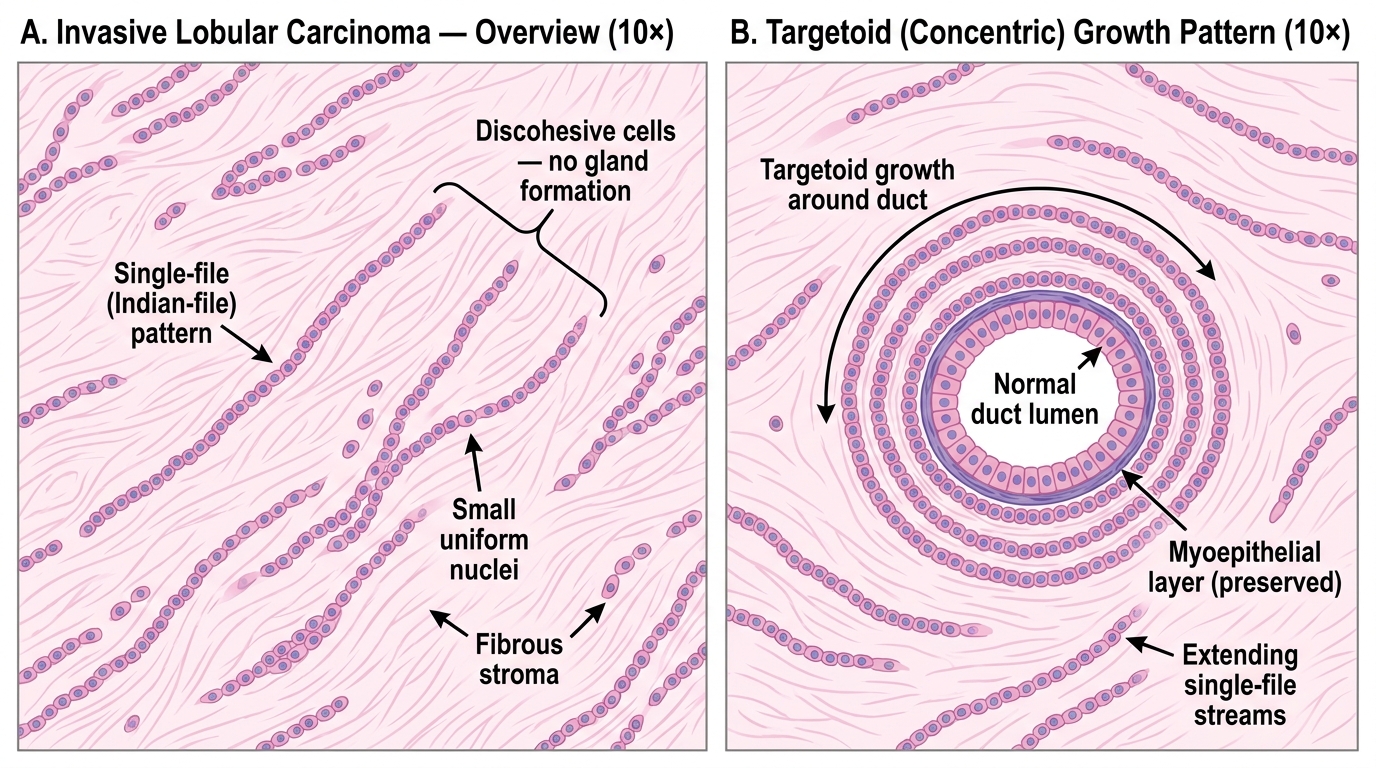
Invasive Lobular Carcinoma — Indian-File Pattern and Targetoid Growth (10×)
Mucinous (colloid) carcinoma:
Tumor cells floating in large pools of extracellular mucin — the mucin is produced by the tumor cells and accumulates outside them in the stroma. Gross appearance: soft, gelatinous, glistening. Low-grade. Good prognosis (90% 10-year survival). The mucin stains strongly with Alcian blue and PAS-AB on special stains.
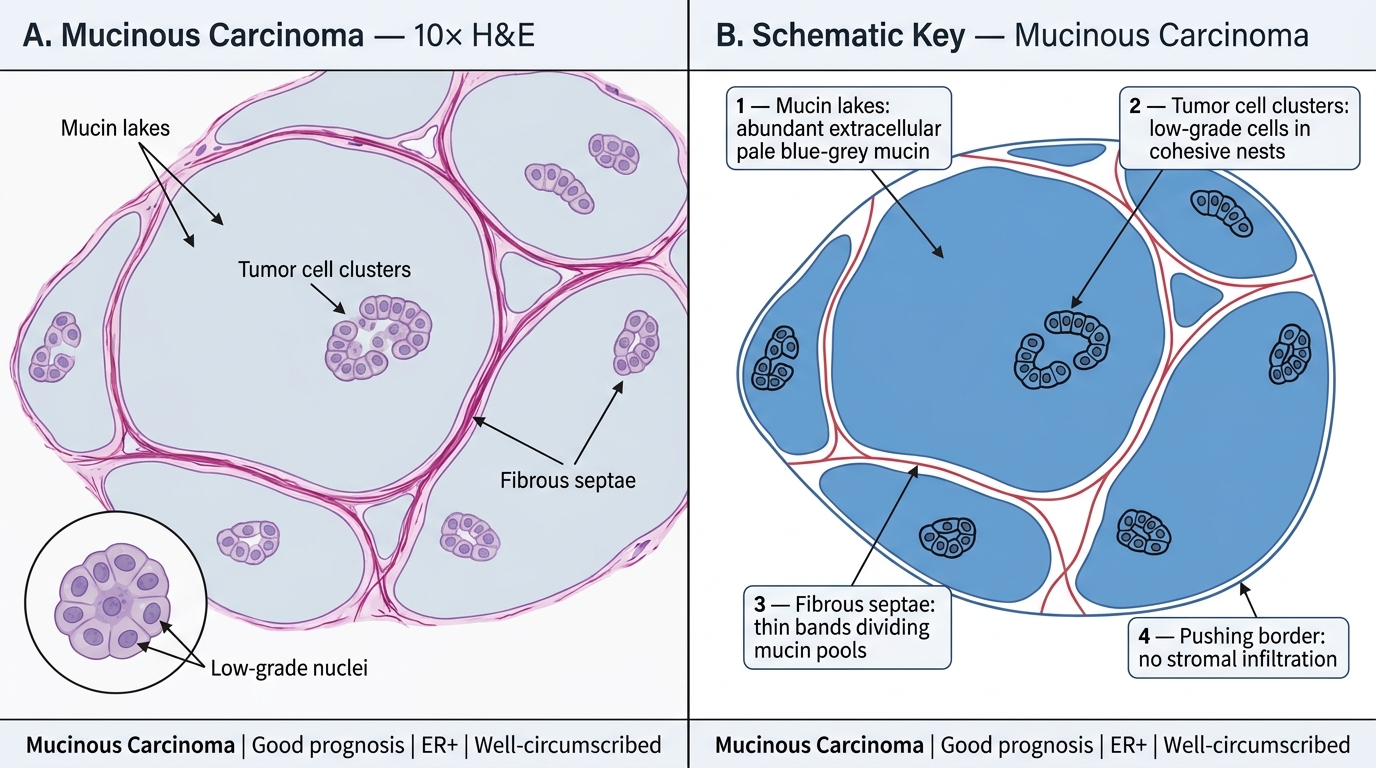
Mucinous Carcinoma — Medium-Power (10×) Histology and Annotated Schematic
Medullary carcinoma:
Paradoxically good prognosis despite high-grade appearance. Four features in combination:
1. Syncytial growth — sheets of high-grade cells with indistinct cell borders (syncytial = cells merge into a sheet)
2. Pushing (not infiltrative) margins
3. Dense lymphoplasmacytic infiltrate at the periphery — this is the immune response that limits spread
4. No tubule formation and no in situ component
Medullary carcinoma is associated with BRCA1 germline mutations. Triple-negative (ER−/PR−/HER2−).
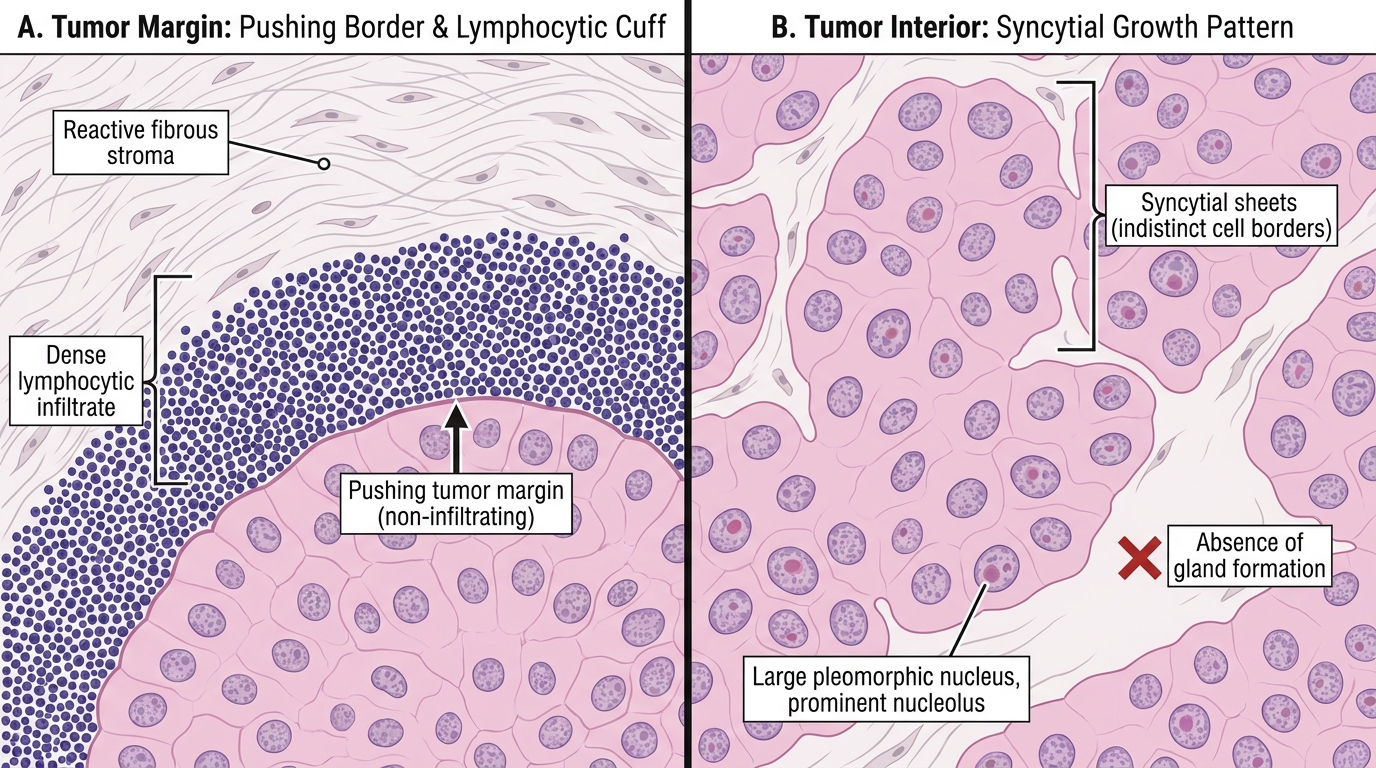
Medullary Carcinoma — Medium-Power (10×) Histological Features
Tubular carcinoma:
Well-differentiated, best prognosis of all invasive types. Tumor forms open, round to oval tubules with a single layer of cells and angulated ('teardrop') lumens — the angulated lumens are the key diagnostic feature. Cells are low-grade with open, pale nuclei. Myoepithelial layer is absent (unlike benign adenosis). Almost always ER-positive, HER2-negative.
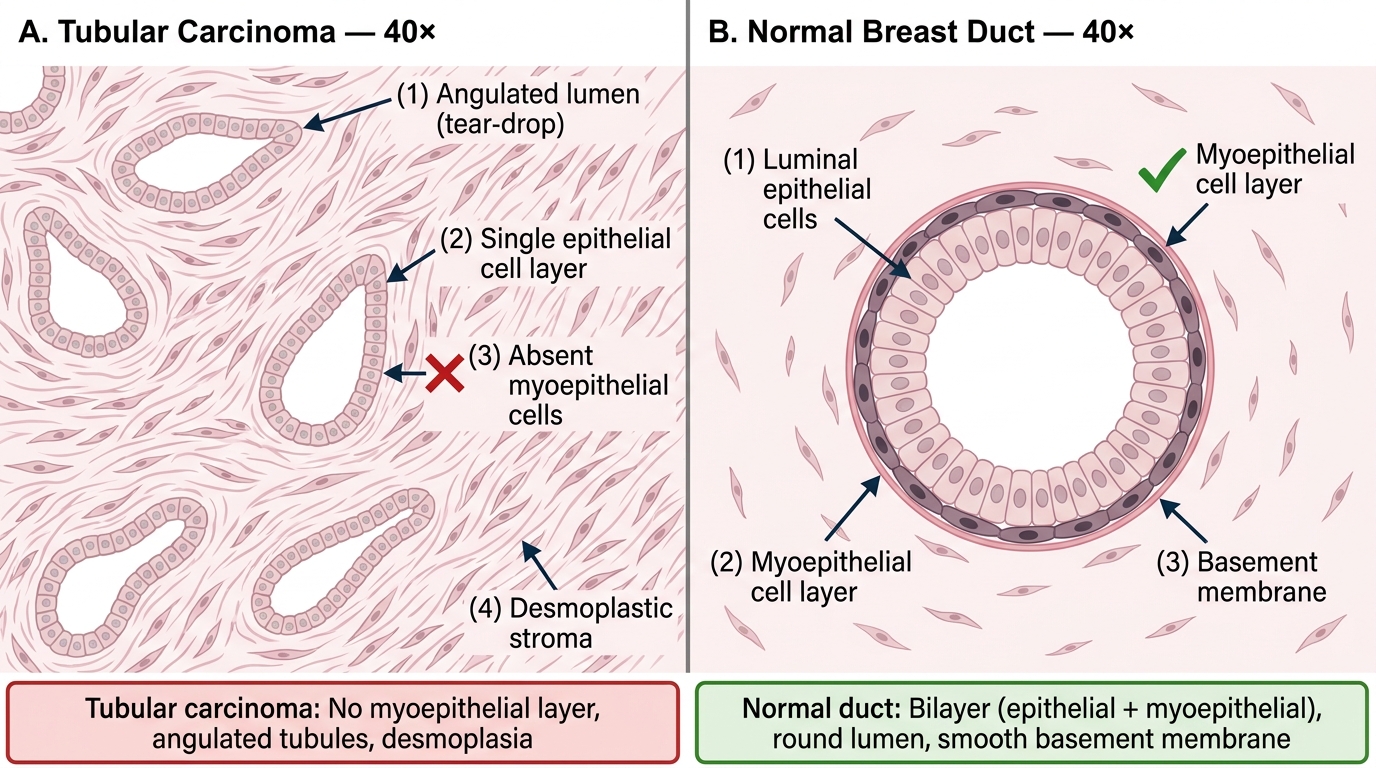
Tubular Carcinoma vs Normal Duct — 40× Histology
CLINICAL PEARL
The desmoplasia clue: When you pick up a breast specimen in the gross lab and it feels unusually hard and gritty — like cutting unripe pear or pencil eraser — think invasive carcinoma with desmoplasia. This physical hardness, combined with the spiculated white stellate appearance on cut section, is pathognomonic of invasive ductal NST. Soft, gelatinous, scoopable tissue = mucinous carcinoma. Hard, gritty, spiculated = NST. This distinction is testable in the viva as 'describe the gross cut section.'