Page 11 of 20
PA32.5-7 | Arthritis (RA, OA, Gout) & Bone Morphology — SDL Guide
Learning Objectives
- Classify rheumatoid arthritis and describe its etiology, immunological basis (RF, anti-CCP, HLA-DR4, TNF/IL-1 pathway), pathogenesis, pannus formation, morphology, radiologic and laboratory features, ACR/EULAR diagnostic criteria, and extra-articular complications
- Classify and describe osteoarthritis and gouty arthritis — including their etiology, pathogenesis, gross and microscopic morphology, radiologic features, diagnostic criteria, and complications
- Contrast RA, OA, and gout across key clinical and pathological dimensions
- Identify and describe the gross and microscopic morphological features of major bone lesions — osteomyelitis, Paget disease, osteosarcoma, giant-cell tumour, Ewing sarcoma, and bone metastases — as required for practical examination
INSTRUCTIONS
Joints and bones together form about 15–18% of Pathology exam marks in Year-2 MBBS and appear frequently in both theory and practicals. This SDL takes you from the immunological storm inside a rheumatoid synovium, through the grinding cartilage loss of osteoarthritis, to the glittering urate crystals of gout — and then anchors those concepts by walking you through the gross and microscopic patterns you must recognise at the microscope table. Read each section actively: pause at the comparison tables, test yourself on the micro-quizzes, and keep asking 'What would I see on the slide?' By the end, you should be able to look at any bone or joint biopsy and generate a differential diagnosis from first principles.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 26 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 42-year-old woman presents with morning stiffness lasting more than an hour, symmetric swelling of her metacarpophalangeal and proximal interphalangeal joints, and a positive anti-CCP antibody. Her neighbour — a 68-year-old retired farmer — has bony, pain-free swellings at his distal interphalangeal joints that have grown slowly over decades. A third patient, a 55-year-old man with chronic kidney disease, is rushed in at midnight with a red-hot, agonisingly tender first metatarsophalangeal joint.
Three patients. Three different types of arthritis. Three completely different mechanisms, morphologies, and treatments. Your ability to distinguish them at the bedside — and on the slide — begins today.
WHY THIS MATTERS
Why this matters for your career:
- Rheumatoid arthritis affects ~1% of the global population and is the most common inflammatory arthritis encountered in medicine and surgery.
- Osteoarthritis is the leading cause of disability in adults over 65 and the most common indication for joint replacement surgery.
- Gout is the most common cause of acute monoarthritis in adult men and is frequently mismanaged — misdiagnosis costs kidneys.
- For your practical examination, you must be able to identify six bone lesion patterns under the microscope; these slides recur year after year in university and board exams.
Understanding the pathogenesis — not just the buzzwords — lets you predict clinical features, interpret reports, and select the right investigation.
RECALL
Before continuing, activate what you already know:
- Autoimmunity basics — What is the difference between a Type II and Type III hypersensitivity reaction? Which cytokines are produced by activated T-helper-1 (Th1) cells?
- Cartilage biology — What type of collagen is in articular cartilage? Who synthesises it, and what degrades it?
- Uric acid metabolism — Where does uric acid come from? What enzyme is deficient or overwhelmed in hyperuricemia? (Hint: think purine catabolism.)
- Bone cells — Name the cell type responsible for bone resorption and the one responsible for bone formation. What stimulates each?
If any of these feel uncertain, a quick 5-minute look at your Biochemistry or Physiology notes now will make everything in this SDL click into place.
Rheumatoid Arthritis — Etiology, Immunology & Pathogenesis
Rheumatoid arthritis (RA) is a chronic, systemic, autoimmune inflammatory arthritis characterised by symmetric inflammation of synovial joints, with progressive cartilage and bone destruction.
Etiology — multifactorial:
• Genetic: HLA-DR4 (and HLA-DR1) alleles — present in ~70% of seropositive RA. These MHC class-II molecules present arthritogenic peptides (possibly citrullinated self-peptides) to CD4+ T cells.
• Environmental: Cigarette smoke is the strongest environmental trigger — it induces protein citrullination in lung tissue, priming the anti-CCP response. Periodontitis (Porphyromonas gingivalis) similarly citrullinates proteins.
• Hormonal: Female predominance (3:1) suggests oestrogen modulation of immune response.
Immunological cascade:
- Antigen-presenting cells in genetically susceptible individuals present citrullinated peptides via HLA-DR4 → activation of CD4+ Th1 and Th17 cells in the synovium.
- Activated T cells release IFN-γ (Th1) and IL-17 (Th17) → activate macrophages and synovial fibroblasts.
- Macrophages and fibroblasts produce TNF-α, IL-1, and IL-6 — the master cytokine triad driving inflammation, synoviocyte proliferation, and osteoclast activation.
- B cells are activated (partly via T-cell help, partly via cytokines) → produce rheumatoid factor (RF) — IgM antibody against the Fc portion of IgG — and anti-CCP (anti-citrullinated protein antibody). Immune complexes (RF + IgG) deposit in synovium and activate complement (Type III hypersensitivity component).
- RANKL upregulation by synovial fibroblasts activates osteoclasts → periarticular bone erosion.
Key lab markers:
• RF — positive in 70–80% of RA (but not specific; also positive in SLE, Sjögren's, normal elderly).
• Anti-CCP — sensitivity ~70%, specificity ~95% — the most specific serological test for RA.
• ESR / CRP — elevated (nonspecific markers of inflammation).
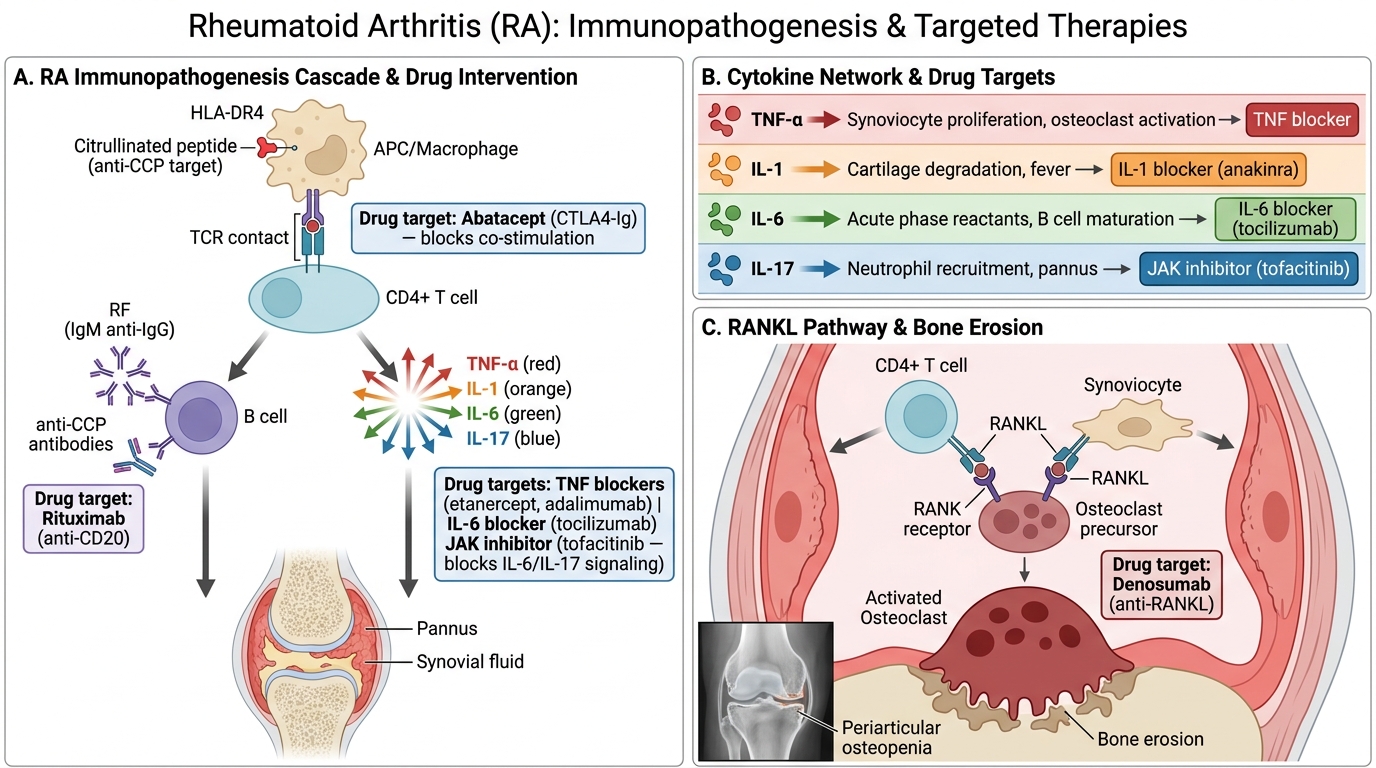
Immunopathogenesis of Rheumatoid Arthritis and Therapeutic Targets
Rheumatoid Arthritis — Morphology, Radiology & Diagnosis
Gross morphology of the synovium:
Early RA shows synovial hyperemia, edema, and villous hypertrophy. The hallmark lesion is pannus — a destructive sheet of proliferating synoviocytes (synovial fibroblasts), inflammatory cells (CD4+ T cells, plasma cells, macrophages), and granulation tissue that spreads over and destroys the articular cartilage and subchondral bone.
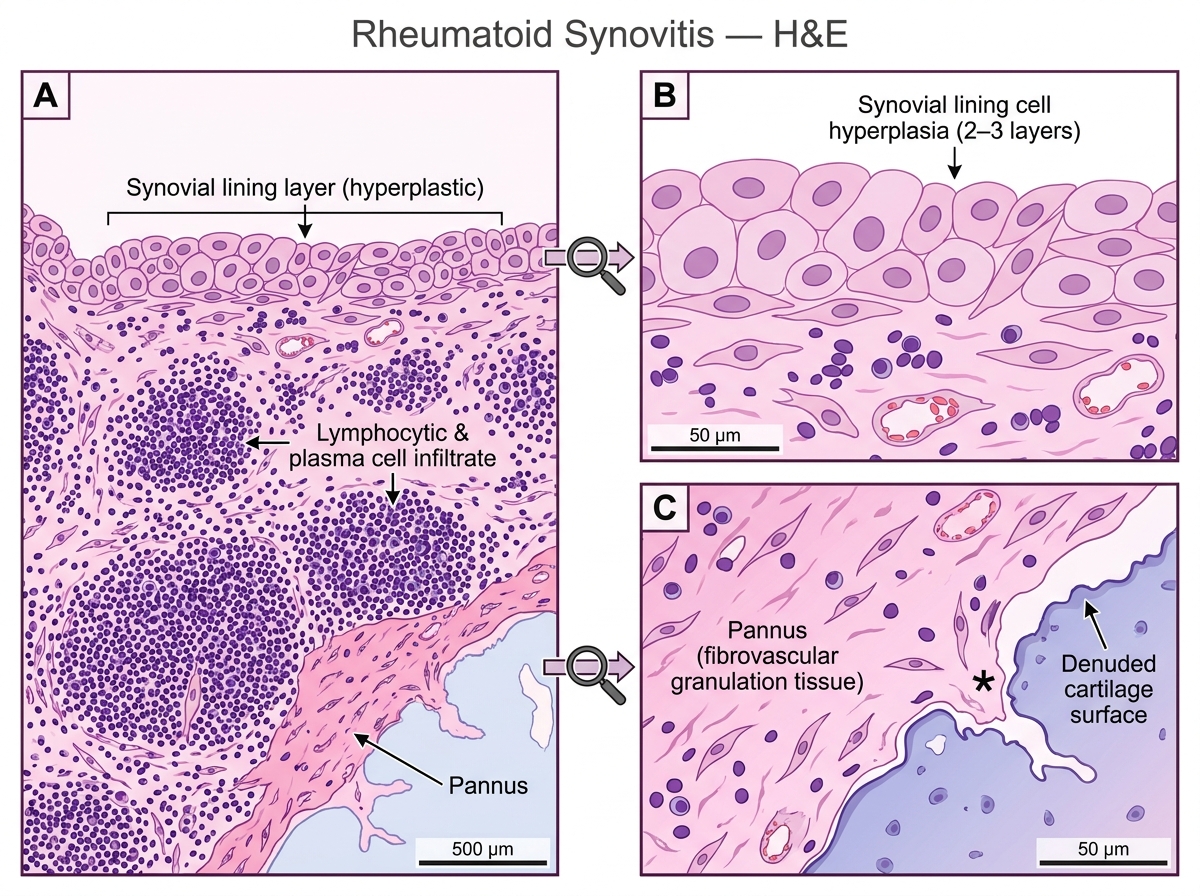
Histopathology of Rheumatoid Synovitis (H&E, Low and High Power)
Microscopic features:
• Synovial lining hyperplasia (normally 1–3 cells thick → 8–10 layers)
• Dense lymphocytic infiltrate (CD4+ T cells + B cells + plasma cells); may form germinal centres (tertiary lymphoid tissue)
• Fibrin deposition on synovial surface
• Pannus invading and eroding cartilage
Distribution: Classically symmetric, small-joint, bilateral — MCPs, PIPs, wrists, knees; DIP joints are typically SPARED (contrast with OA and psoriatic arthritis).
Radiologic features:
• Juxta-articular osteopenia — periarticular bone loss early, from hyperaemia and disuse
• Marginal (bare-area) erosions — where pannus contacts bone, typically at the joint margins
• Joint-space narrowing — from cartilage destruction
• Subluxation and deformity — late (ulnar deviation of fingers, swan-neck, boutonnière)
• No osteophytes (contrast OA)
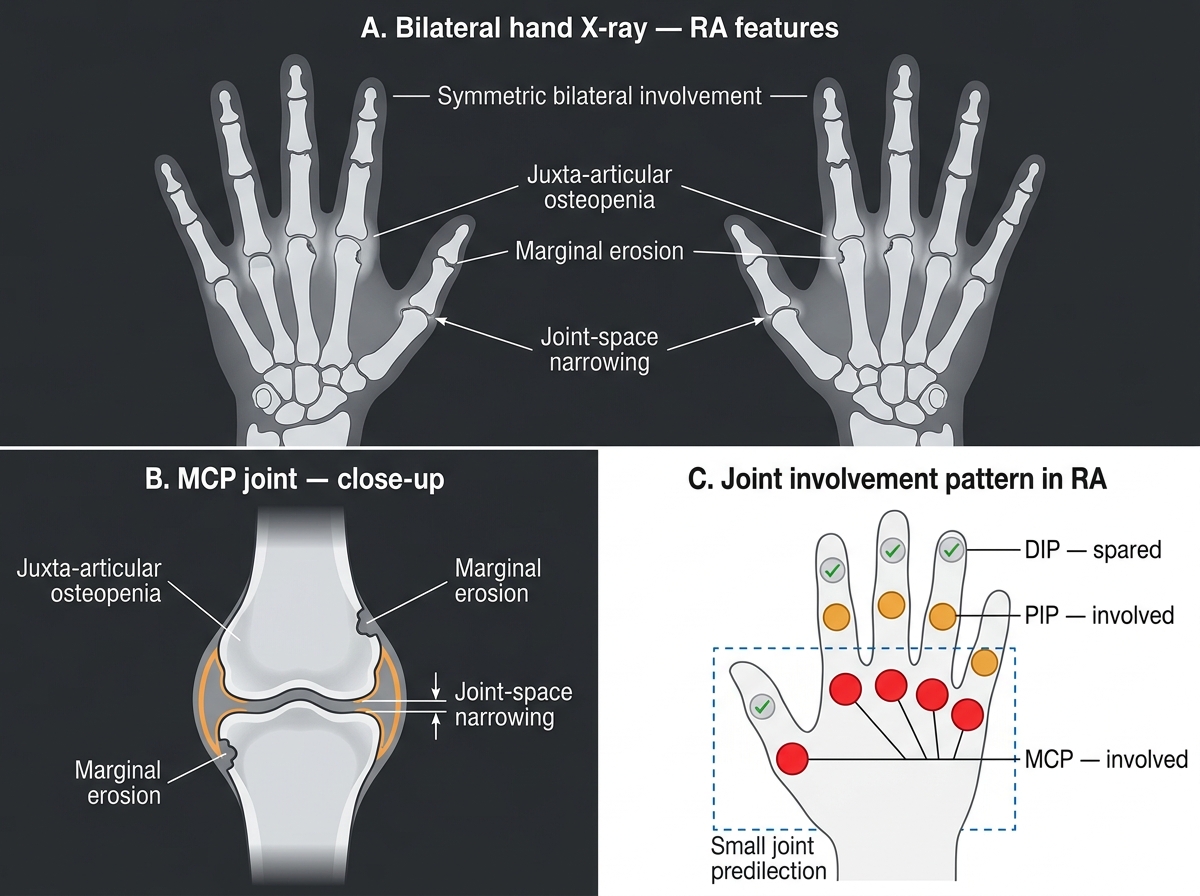
Radiographic Features of Rheumatoid Arthritis in the Hands
ACR/EULAR 2010 Diagnostic Criteria (score ≥6/10 = definite RA):
| Domain | Score |
|---|---|
| Joint involvement: 1 large joint | 0 |
| 2–10 large joints | 1 |
| 1–3 small joints | 2 |
| 4–10 small joints | 3 |
| >10 joints (at least 1 small) | 5 |
| Serology: RF and anti-CCP negative | 0 |
| Low positive RF or anti-CCP | 2 |
| High positive RF or anti-CCP | 3 |
| Acute phase: normal CRP and ESR | 0 |
| Abnormal CRP or ESR | 1 |
| Duration: <6 weeks | 0 |
| ≥6 weeks | 1 |
Extra-articular complications:
• Rheumatoid nodules — firm, subcutaneous nodules over bony prominences (elbows, occiput); microscopically show central fibrinoid necrosis surrounded by palisading macrophages and peripheral chronic inflammatory cells — a classic granuloma-like structure.
• Secondary amyloidosis (AA amyloidosis) — from chronic elevation of SAA; deposits in kidney → nephrotic syndrome, renal failure.
• Vasculitis, pericarditis, pleural effusion, Felty syndrome (RA + splenomegaly + neutropenia), atlanto-axial subluxation (C1-C2 — danger in intubation), scleritis.
Juvenile RA (JIA/Still's disease): Onset <16 years; systemic form has quotidian fever, salmon-pink rash, hepatosplenomegaly; RF often negative; prognosis variable by subtype.
CLINICAL PEARL
The DIP rule: RA classically SPARES the distal interphalangeal joints. If a patient has DIP involvement, think OA (Heberden's nodes), psoriatic arthritis, or reactive arthritis — not RA. Anti-CCP antibodies can appear up to 10 years before clinical RA and predict a more erosive disease course — a positive anti-CCP in an asymptomatic person warrants close follow-up.
Osteoarthritis — Pathogenesis & Morphology
Osteoarthritis (OA) is a degenerative joint disease characterised by progressive loss of articular cartilage, reactive bone changes, and secondary mild synovial inflammation. Unlike RA, it is not primarily autoimmune — it is driven by mechanical and biochemical cartilage failure.
Pathogenesis:
1. Initiation: Mechanical overload, aging, obesity, or prior injury damages chondrocytes → they release matrix metalloproteinases (MMPs) and ADAMTS enzymes that degrade type II collagen and aggrecan.
2. Cartilage breakdown: Loss of proteoglycans → cartilage becomes less resilient → fibrillation (superficial cracks) → fissuring → full-thickness loss ("eburnation").
3. Subchondral response: Exposed subchondral bone is polished to ivory-like hardness (eburnation) and develops cysts from synovial fluid forced into microfractures (subchondral cysts).
4. Reparative reaction: Bone at joint margins reacts with osteophyte formation — outgrowths of fibrocartilage and bone that restrict movement and cause pain.
5. Synovial inflammation is secondary and mild (compare RA where it is the primary driver).
Risk factors: Age (most important), female sex, obesity, prior joint injury, occupational overuse, developmental dysplasia.
Gross morphology:
• Fibrillation — earliest; cartilage surface develops vertical clefts like a worn tyre tread
• Eburnation — bone-on-bone, glistening, ivory appearance of subchondral bone
• Osteophytes — bony spurs at joint margins
• Subchondral cysts — fluid-filled spaces just below the articular surface
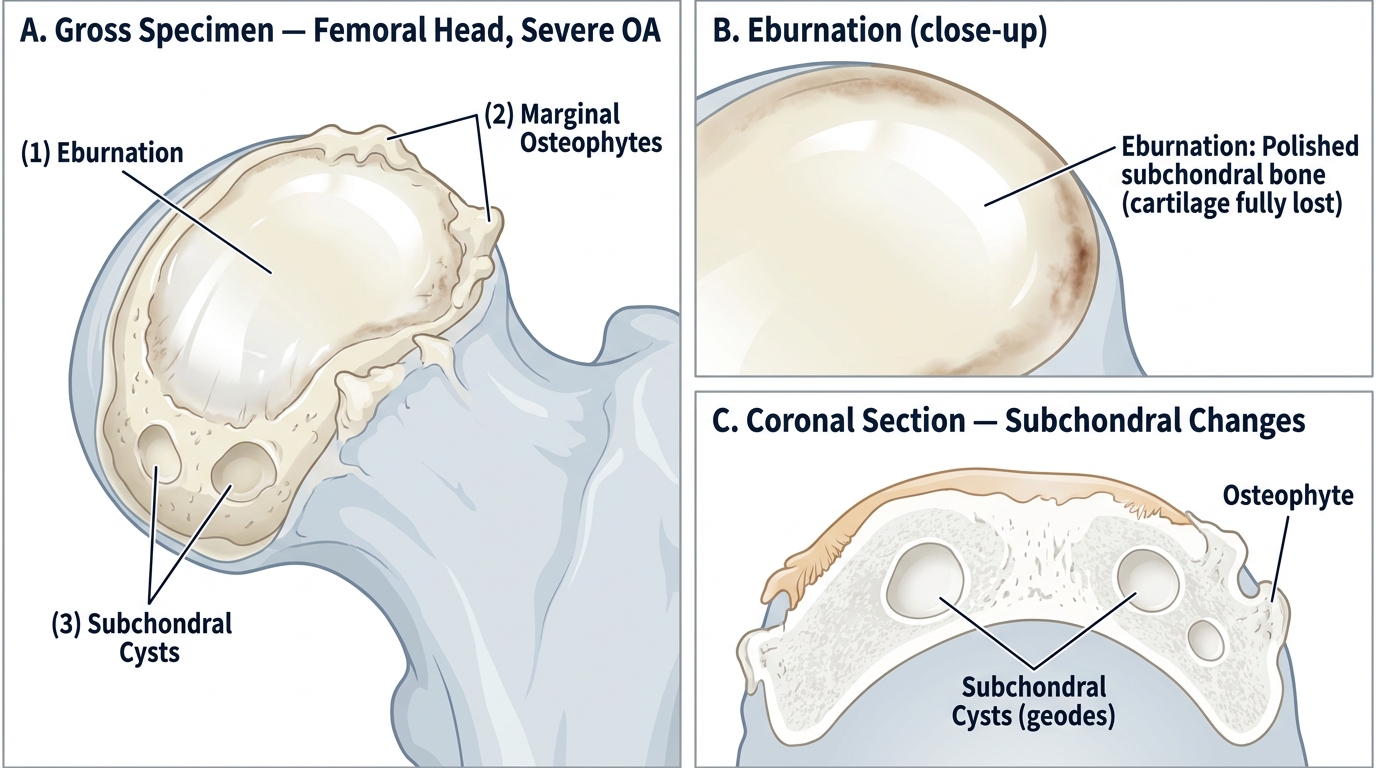
Gross Pathology of the Femoral Head in Severe Osteoarthritis
Microscopic features:
• Superficial fibrillation of cartilage with vertical cleft formation
• Loss of chondrocyte nuclear staining (ghost cells) in denuded zones
• Chondrocyte clusters (brood capsules) — reactive chondrocyte proliferation in viable areas (pathognomonic feature)
• Subchondral bone shows microfracture, sclerosis, and cyst formation
• Mild, patchy synovial inflammation with fibrous loose bodies
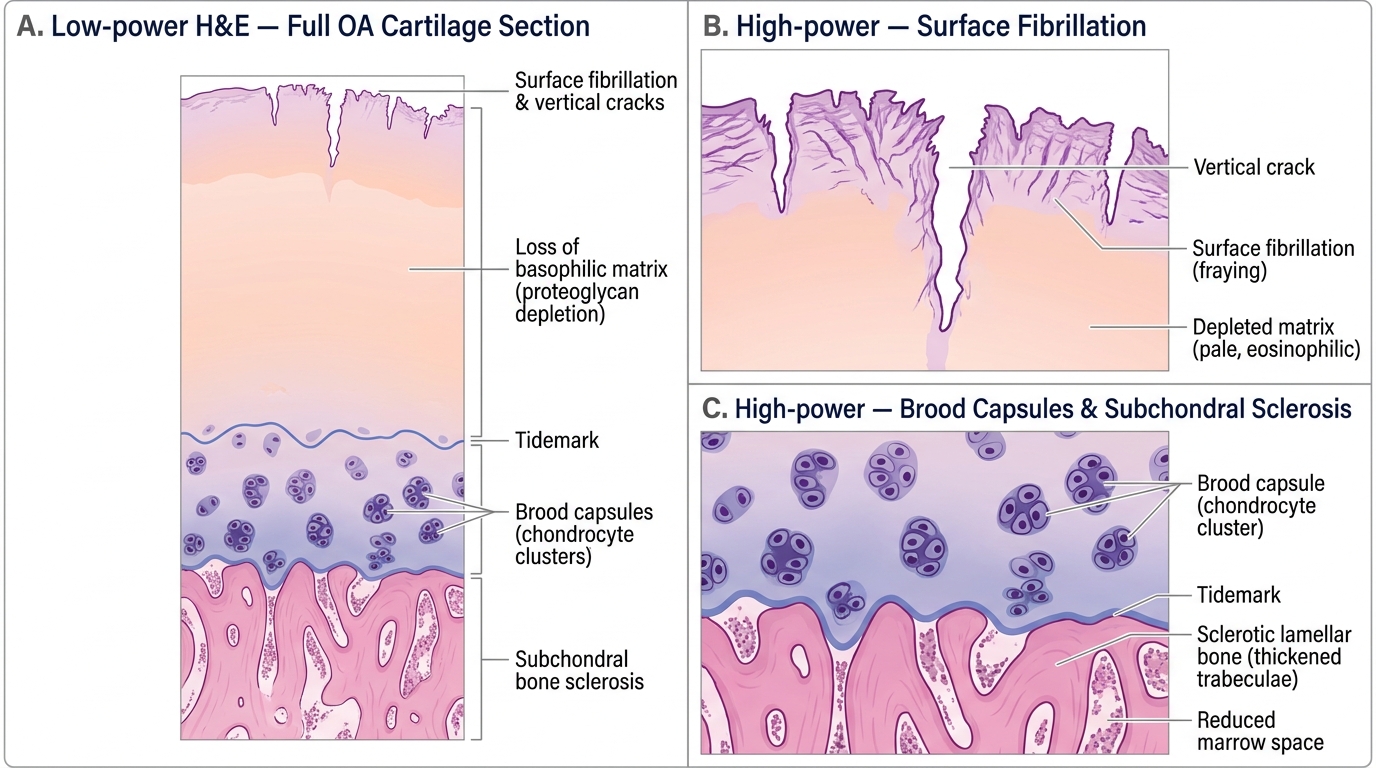
Histopathology of Osteoarthritic Cartilage (H&E)
Distribution: Weight-bearing joints — hips, knees, cervical/lumbar spine; DIP and PIP joints of hands (contrast: RA spares DIP).
Clinical nodes:
• Heberden's nodes — bony osteophytes at DIP joints (hard, non-tender in established disease)
• Bouchard's nodes — osteophytes at PIP joints
Radiologic features:
• Asymmetric joint-space narrowing (affects weight-bearing compartment, e.g., medial > lateral in knee)
• Osteophytes — marginal bony spurs (absent in RA)
• Subchondral sclerosis (increased bone density)
• Subchondral cysts (geode formation)
• No periarticular osteopenia, no erosions (contrast RA)