Page 12 of 20
PA32.5-7 | Arthritis (RA, OA, Gout) & Bone Morphology — SDL Guide (Part 2)
Gouty Arthritis — Pathogenesis, Morphology & Complications
Gout is caused by hyperuricemia and the deposition of monosodium urate (MSU) crystals in joints and soft tissues, triggering intense acute inflammation.
Pathogenesis of hyperuricemia:
• Primary gout (90%): Idiopathic, usually underexcretion of uric acid by the kidney; predominantly middle-aged men.
• Secondary gout: Overproduction (myeloproliferative disorders, tumour lysis syndrome, enzyme defects — HGPRT deficiency in Lesch-Nyhan syndrome) or underexcretion (renal failure, diuretics, low-dose aspirin, cyclosporin).
• Uric acid = end product of purine catabolism via xanthine oxidase.
How crystals cause disease:
1. MSU crystals deposit in synovial fluid and are phagocytosed by neutrophils → NLRP3 inflammasome activation → IL-1β release → explosive neutrophilic inflammation.
2. Crystals are needle-shaped, negatively birefringent under polarised light (appear yellow when parallel to the slow ray of the compensator).
3. Compare: Calcium pyrophosphate crystals (pseudogout) are rhomboid/rod-shaped and positively birefringent (blue when parallel to slow ray).
Clinical phases:
- Asymptomatic hyperuricemia — elevated serum uric acid without symptoms; most people with hyperuricemia never develop gout.
- Acute gouty arthritis — sudden-onset, exquisitely tender, red, hot, swollen joint; podagra (first MTP joint) in 50% of initial attacks; self-limiting (resolves in days–weeks); triggered by alcohol, dietary purine load, dehydration, trauma, surgery.
- Intercritical gout — asymptomatic intervals between attacks (may last years).
- Chronic tophaceous gout — persistent hyperuricemia leads to tophi deposition in soft tissues (ears, Achilles tendon, bursae, finger pads, extensor surfaces); persistent low-grade joint inflammation.
Morphology:
Tophus — a collection of MSU crystals surrounded by a granulomatous reaction: foreign-body type giant cells, macrophages, fibroblasts, and chronic inflammatory cells encircling the needle-like crystal deposits.
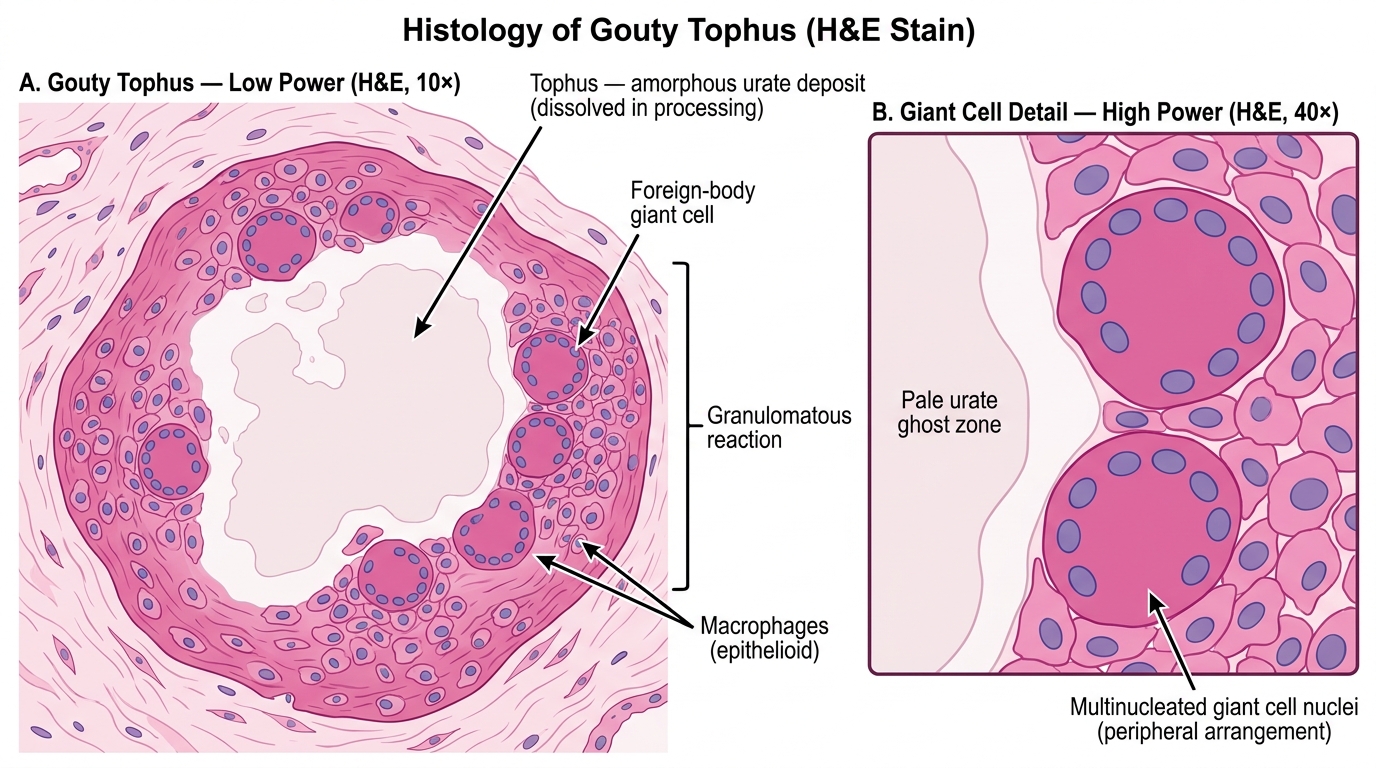
Histology of Gouty Tophus — H&E Stain (Low & High Power)
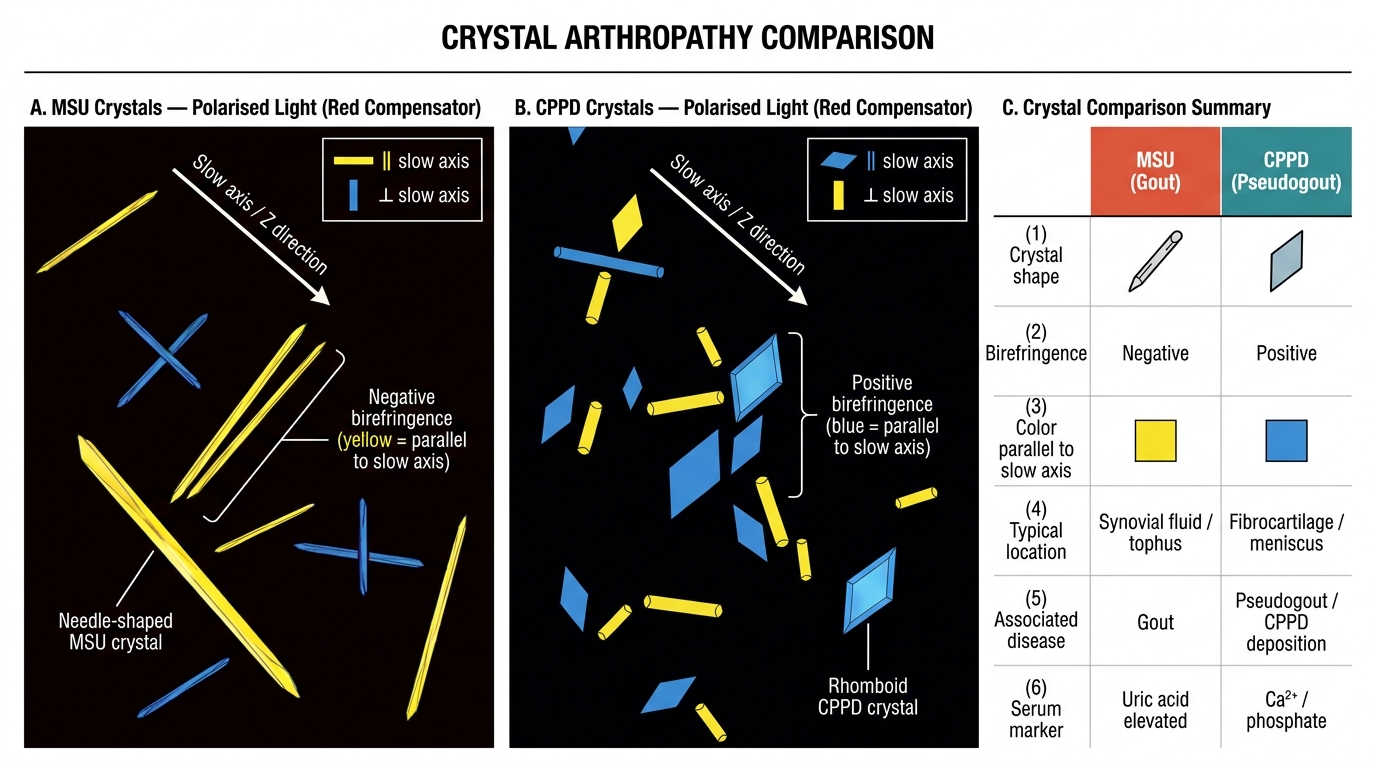
Synovial Crystal Identification Under Polarised Light with Red Compensator: MSU vs CPPD
Complications:
• Urate nephropathy — MSU crystal deposition in renal medullary interstitium → tubular obstruction, inflammation, chronic renal failure ("gouty nephropathy").
• Uric acid nephrolithiasis — radiolucent renal stones (unlike calcium oxalate/phosphate stones which are radio-opaque).
• Acute uric acid nephropathy — massive crystal precipitation in collecting ducts during tumour lysis → acute oliguric renal failure.
Acute attack: aspiration findings — cloudy fluid, WBC >20,000 (predominantly neutrophils), negatively birefringent needle crystals; uric acid often not elevated during acute attack (crystals deposit as levels fall).
SELF-CHECK
A 55-year-old woman has symmetric swelling of her MCP and PIP joints with morning stiffness >1 hour. Serology shows high-positive anti-CCP. X-ray shows juxta-articular osteopenia with marginal erosions but NO osteophytes. Her DIP joints are NORMAL. What is the most likely diagnosis and which joint-sparing pattern clinches it?
A. Osteoarthritis — Heberden's nodes at DIPs are the hallmark
B. Rheumatoid arthritis — DIP sparing with symmetric MCP/PIP involvement and erosions
C. Gout — negatively birefringent crystals in joint fluid confirm it
D. Psoriatic arthritis — DIP involvement distinguishes it from RA
Reveal Answer
Answer: B. Rheumatoid arthritis — DIP sparing with symmetric MCP/PIP involvement and erosions
RA classically spares the DIP joints and involves MCPs, PIPs, and wrists symmetrically. The anti-CCP is highly specific (95%), juxta-articular osteopenia and marginal erosions without osteophytes are characteristic radiologic findings. OA affects DIPs (Heberden's nodes) and is not erosive. Gout is typically monoarticular initially and confirmed by crystal analysis. Psoriatic arthritis involves DIPs (the opposite of RA).
RA vs OA vs Gout — Comparison Table
This table is high-yield for theory and clinical exams. Memorise the contrasting columns.
| Feature | Rheumatoid Arthritis | Osteoarthritis | Gout |
|---|---|---|---|
| Type | Autoimmune/inflammatory | Degenerative | Crystal-induced inflammatory |
| Age / Sex | 30–50 yrs; F > M (3:1) | >65 yrs; F > M | 40–60 yrs; M > F (95%) |
| Joints | Symmetric; MCPs, PIPs, wrists | Asymmetric; hips, knees, DIPs | First MTP (podagra); acute monoarthritis |
| DIP involvement | Spared | Heberden's nodes (DIP), Bouchard's (PIP) | Can be affected in tophaceous stage |
| Onset | Gradual; morning stiffness >1 hr | Gradual; stiffness <30 min; worse with use | Acute, sudden, nocturnal; exquisitely tender |
| Synovium | Hyperplastic; pannus; lymphocytic infiltrate | Mild secondary inflammation | Acute: neutrophilic; Chronic: granulomatous tophus |
| Cartilage loss | Pannus-mediated; enzymatic | Mechanical/biochemical; fibrillation | Secondary to crystal-induced inflammation |
| X-ray | Osteopenia, erosions, no osteophytes | Osteophytes, sclerosis, subchondral cysts | Punched-out erosions ("rat-bite") with overhanging edges in chronic |
| Serology | RF +, anti-CCP + | Negative | Serum uric acid elevated (not always during attack) |
| Key lab/aspiration | Anti-CCP, ↑ESR, ↑CRP | Usually normal | Negatively birefringent needle crystals; WBC >20,000 |
| Extra-articular | Nodules, amyloidosis, vasculitis, ILD | Local (subchondral cysts, loose bodies) | Tophi, urate nephropathy, nephrolithiasis |
| Treatment target | TNF-α, IL-6, JAK (DMARDs) | Symptom management; joint replacement | Colchicine (acute); allopurinol (chronic) |
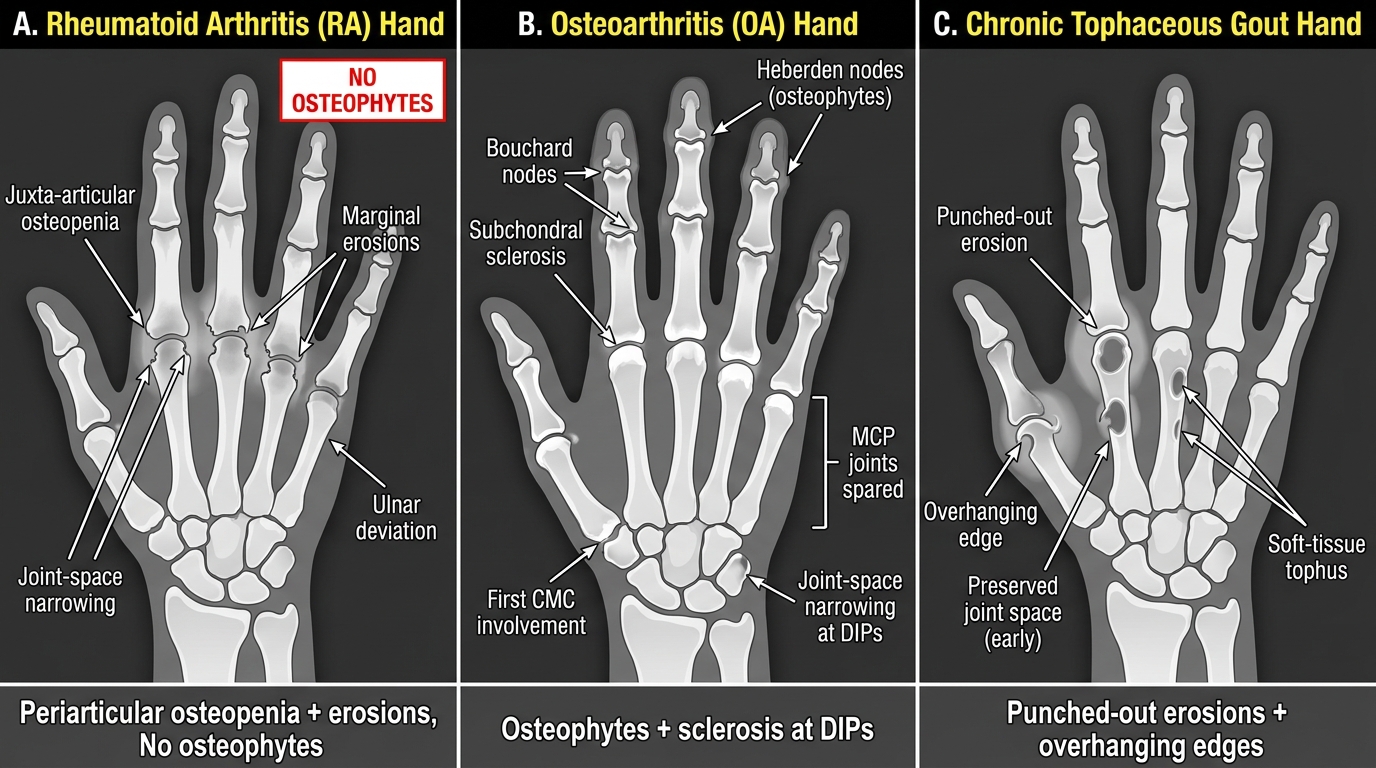
Radiographic Comparison: RA vs OA vs Gout — Hand Arthropathy Patterns
CLINICAL PEARL
The 'treat-to-target' trap in gout: Serum uric acid is often normal or even low during an acute gouty attack because crystals are precipitating out of solution as levels fall — do NOT use a normal uric acid to rule out gout acutely. The target for chronic gout management is uric acid <6 mg/dL (below the saturation point for MSU crystal formation). Allopurinol paradoxically can trigger acute attacks when first started (by mobilising crystals) — always co-prescribe prophylactic colchicine for 3–6 months when initiating allopurinol.
SELF-CHECK
During microscopic examination of a joint aspirate from a 60-year-old man with acute knee swelling, you see rhomboid/rod-shaped crystals that appear BLUE when aligned parallel to the slow axis of the compensator under polarised light. What is the diagnosis?
A. Gout — monosodium urate crystals showing negative birefringence
B. Pseudogout — calcium pyrophosphate crystals showing positive birefringence
C. Septic arthritis — gram-positive cocci confirmed by culture
D. RA — fibrin crystals in the synovial fluid
Reveal Answer
Answer: B. Pseudogout — calcium pyrophosphate crystals showing positive birefringence
Calcium pyrophosphate dihydrate (CPPD) crystals in pseudogout are rhomboid-shaped and POSITIVELY birefringent (blue when parallel to the slow axis, yellow when perpendicular). Monosodium urate crystals in gout are needle-shaped and NEGATIVELY birefringent (yellow when parallel, blue when perpendicular). The shape and birefringence pattern here — rhomboid + blue (positive) — diagnose pseudogout (chondrocalcinosis), often affecting the knee in elderly patients.
Bone Morphology Practical — Systematic Pattern Recognition
PA32.7 requires you to identify bone lesions morphologically. The practical examiner will give you a slide — you must name the lesion and justify it from the features you see. This section walks through the six patterns you must own.
Approach every bone slide in this order: (1) Is there normal bone? (2) What is the cellular infiltrate or matrix abnormality? (3) Is there destruction, new bone formation, or both? (4) What pattern does that make?
1. Acute Osteomyelitis / Sequestrum
Etiology: Haematogenous spread (children: metaphysis; Staphylococcus aureus ~80%); or contiguous spread.
Gross key features:
• Involucrum — reactive new bone shell surrounding the infected area
• Sequestrum — devitalised, dead bone fragment within the abscess cavity (avascular, no cells, basophilic outlines)
• Cloaca — opening in involucrum through which pus drains
Microscopic key features:
• Acute: neutrophilic infiltrate, bone necrosis (empty lacunae, basophilic dead bone)
• Chronic: lymphocytes, plasma cells, fibrosis, new bone formation
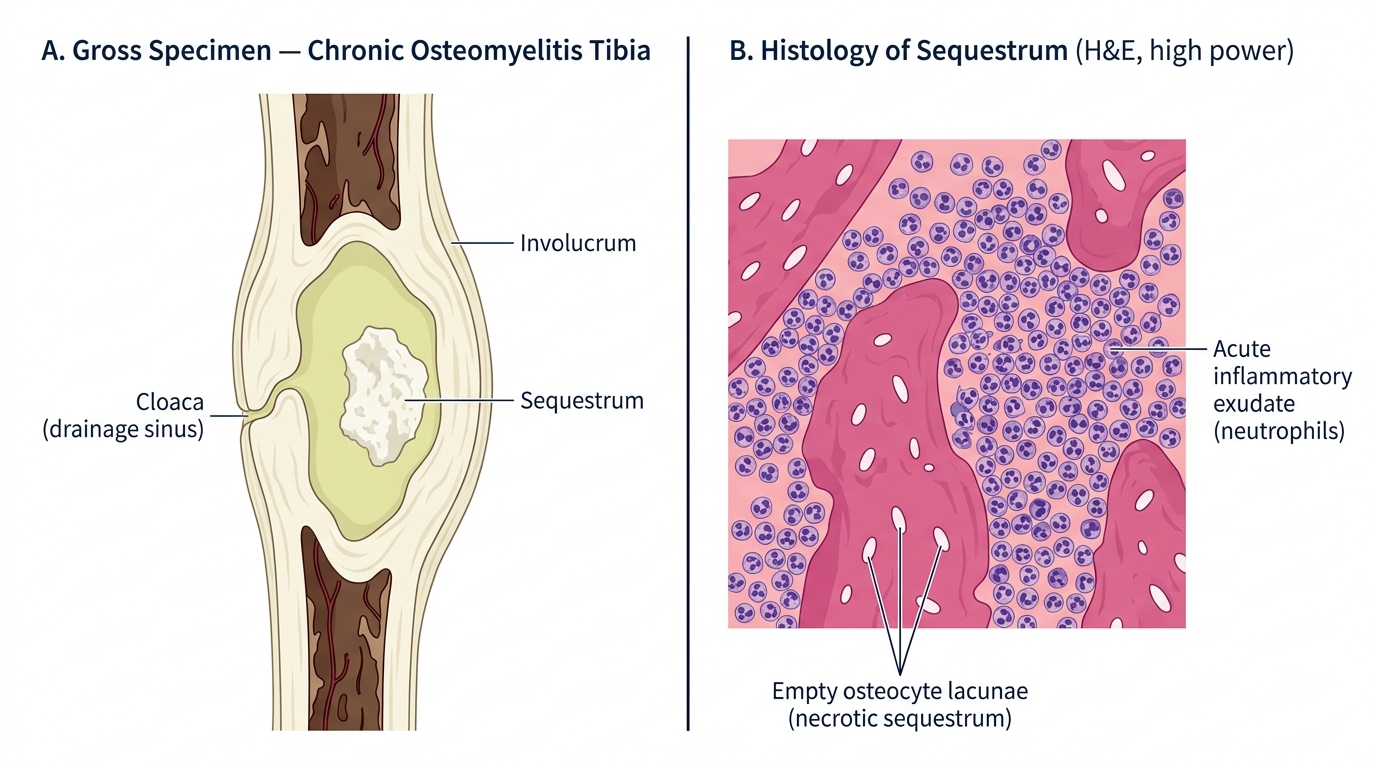
Chronic Osteomyelitis — Gross and Microscopic Features
2. Paget Disease — Mosaic Pattern
Etiology: Probable paramyxoviral trigger + RANK pathway dysregulation; older adults.
Gross: Enlarged, deformed bone — hat size increases, "chalk-stick" fractures; skull enlargement.
Microscopic hallmark: Mosaic (jigsaw) pattern — irregular cement lines in lamellar bone giving the appearance of a crazy-paving or mosaic; both osteoblasts and osteoclasts are increased (alternating phases of resorption and chaotic deposition).
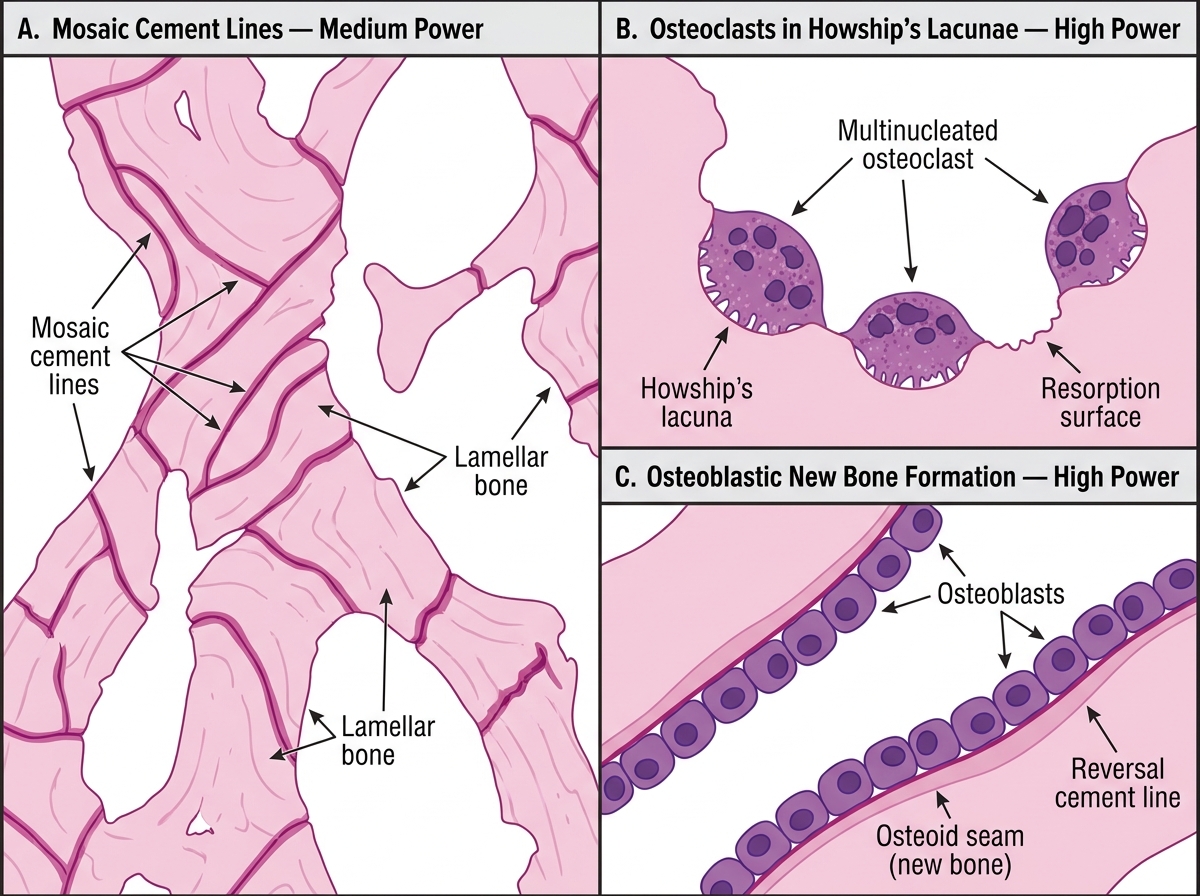
Paget Disease of Bone — H&E Histological Features
3. Osteosarcoma — Malignant Osteoid
Definition: Malignant tumour in which the tumour cells directly produce osteoid (unmineralised bone matrix). Most common primary malignant bone tumour in children/adolescents; metaphysis of distal femur or proximal tibia.
Gross: Metaphyseal destructive mass; Codman's triangle (periosteal elevation); sunburst pattern on X-ray.
Microscopic hallmark: Malignant osteoid — pink, homogeneous, amorphous matrix directly produced by pleomorphic, hyperchromatic malignant osteoblasts. The key question: "Are these atypical cells making bone?" Yes → osteosarcoma.
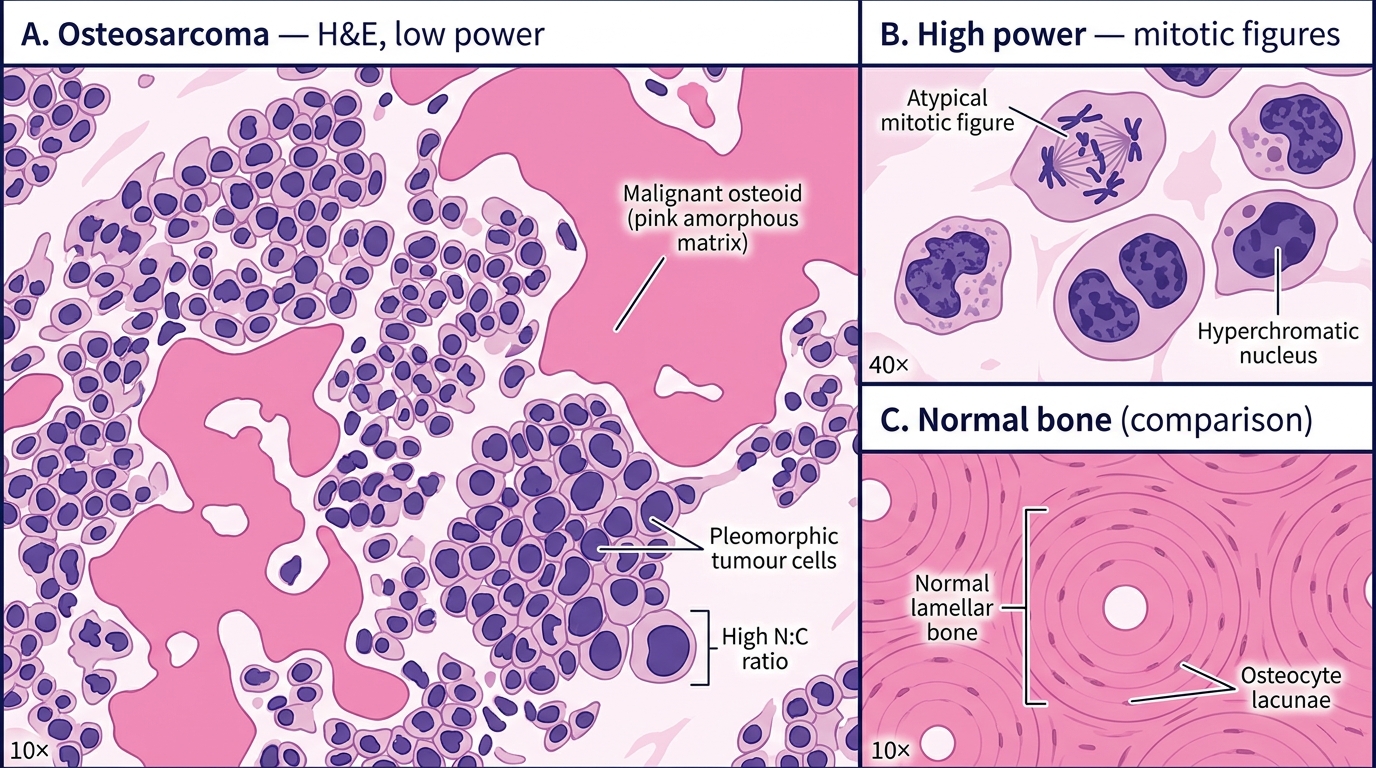
Osteosarcoma — H&E Histology: Malignant Osteoid Production and Cellular Pleomorphism
4. Giant-Cell Tumour (GCT) — Osteoclast-Type Giant Cells
Definition: Locally aggressive tumour of the epiphysis (young adults, 20–40 years); distal femur, proximal tibia most common.
Gross: Epiphyseal, eccentric, soap-bubble lytic lesion on X-ray.
Microscopic hallmark: Uniformly distributed osteoclast-type multinucleated giant cells (may contain 50–100 nuclei) in a background of ovoid to spindle mononuclear stromal cells; nuclei of giant cells and stromal cells look similar (same appearance — key feature).
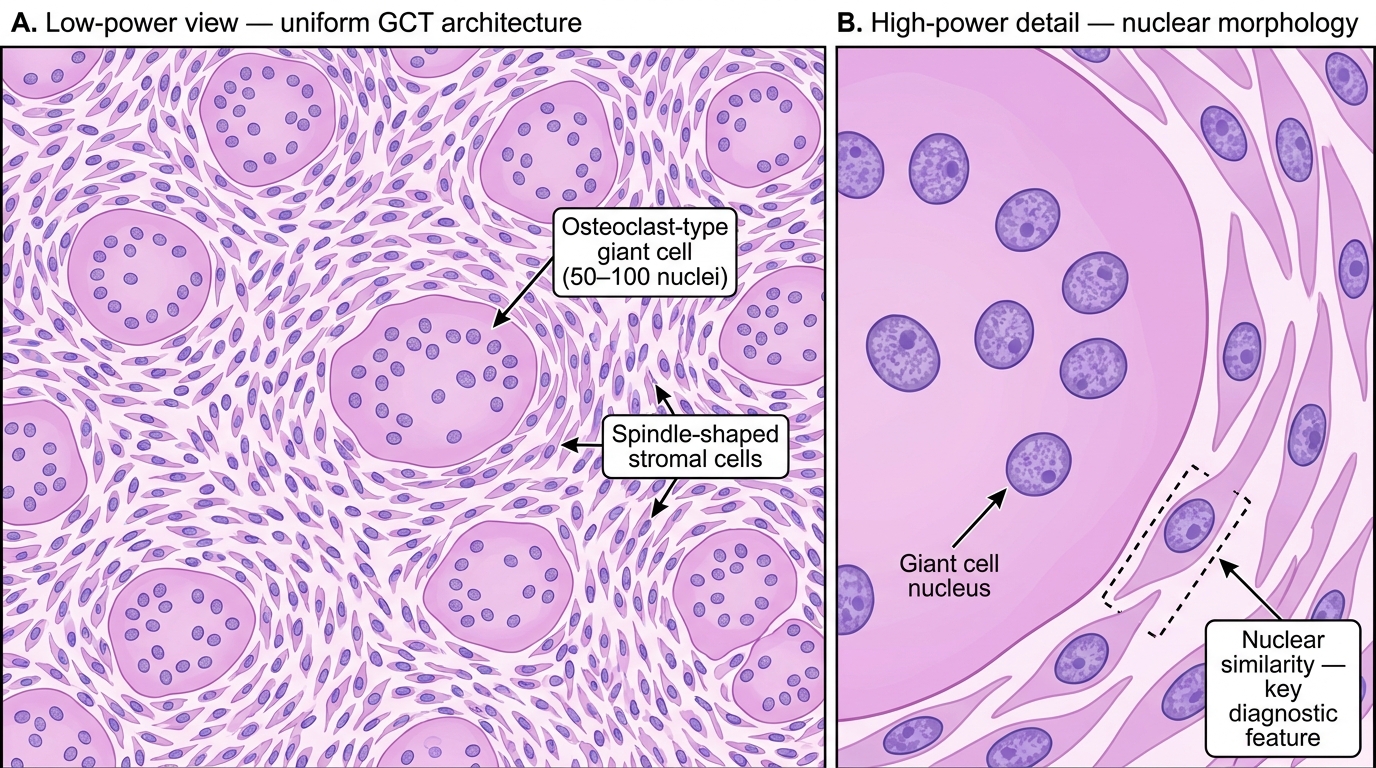
Giant-Cell Tumour (GCT) of Bone — H&E Photomicrograph
5. Ewing Sarcoma — Small Round Blue Cells
Definition: Malignant tumour of bone (and soft tissue); children/adolescents; diaphysis (contrast GCT = epiphysis, osteosarcoma = metaphysis).
Genetics: t(11;22)(q24;q12) → EWSR1-FLI1 fusion; CD99 positive (MIC-2 antigen).
Gross: Diaphyseal, onion-skin periosteal reaction on X-ray; can mimic osteomyelitis clinically (fever, ↑WBC).
Microscopic hallmark: Sheets of uniform small, round, blue cells with scant cytoplasm and round nuclei; no matrix production; PAS-positive glycogen granules in cytoplasm; CD99 strongly positive on IHC.
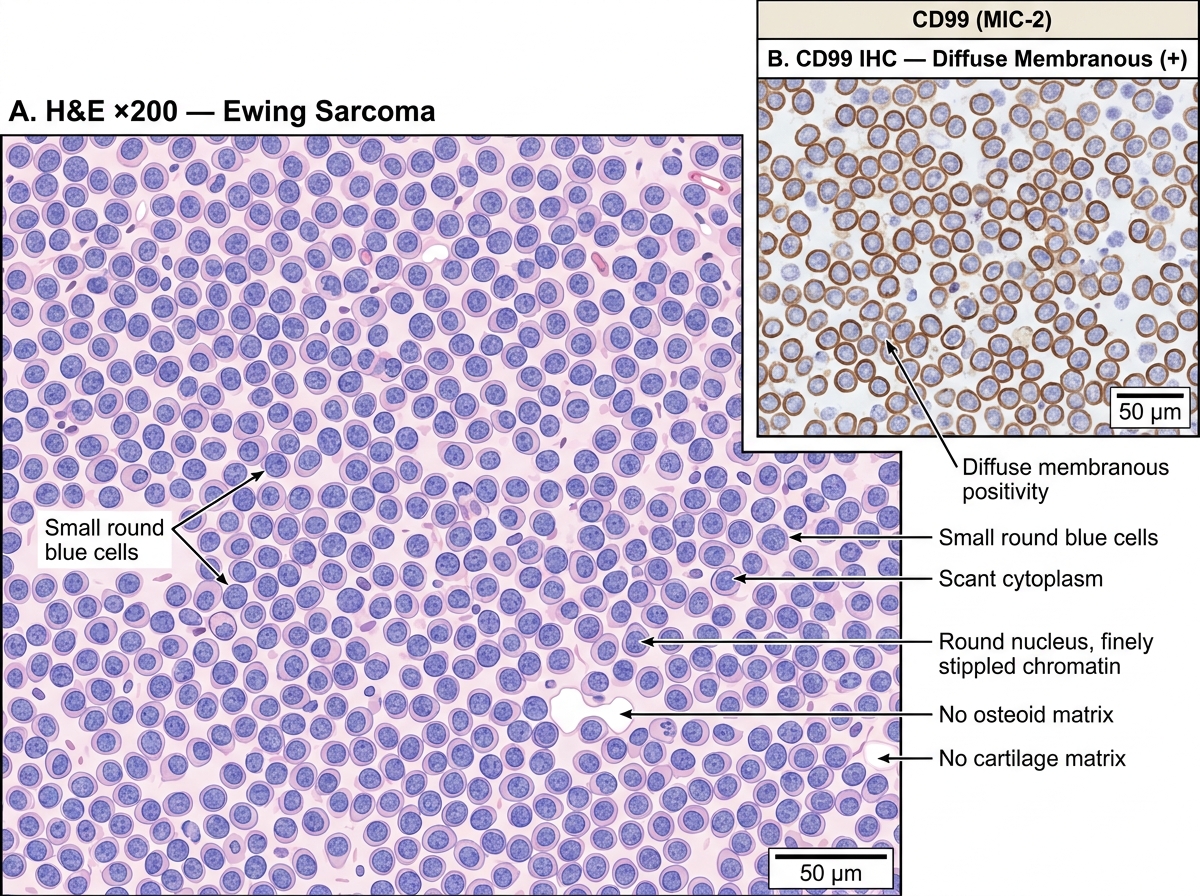
Ewing Sarcoma — H&E Morphology and CD99 Immunohistochemistry
6. Bone Metastases
Context: Most common malignant bone tumour overall (more common than primary tumours). Common primaries: Breast, Lung, Prostate, Kidney, Thyroid (mnemonic: BLPKiT; or Breast Likes Killing Prostate/Thyroid).
Pattern:
• Lytic (osteoclast activation dominant): lung, kidney, thyroid, myeloma
• Sclerotic/blastic (osteoblast stimulation): prostate, carcinoid
• Mixed: breast
Microscopic key: Clusters or sheets of cohesive epithelial cells (carcinoma cells forming glands, nests, or solid sheets) in a fibrotic stroma — within a background of normal or reactive bone. The 'wrong' cell in bone tissue.