Page 13 of 20
PA32.5-7 | Arthritis (RA, OA, Gout) & Bone Morphology — SDL Guide (Part 3)
Master Bone Lesion Recognition Table
Use this table as a quick-reference before practicals.
| Lesion | Location | Age | Key Micro Feature | X-ray Clue | Marker/IHC |
|---|---|---|---|---|---|
| Osteomyelitis | Metaphysis (child), any (adult) | Any | Empty lacunae, neutrophils, sequestrum | Lytic + periosteal reaction | Culture (Staph aureus) |
| Paget disease | Skull, pelvis, femur | >60 yrs | Mosaic cement lines, ↑osteoclasts + osteoblasts | Cotton-wool skull, cortical thickening | ↑↑ Alkaline phosphatase |
| Osteosarcoma | Metaphysis (distal femur/prox tibia) | 10–20 yrs | Malignant osteoid from pleomorphic cells | Sunburst + Codman's triangle | Vimentin, SATB2 |
| GCT | Epiphysis (distal femur/prox tibia) | 20–40 yrs | Osteoclast-type giant cells + similar stromal nuclei | Soap-bubble, eccentric, no sclerosis | H3.3 G34W mutation |
| Ewing sarcoma | Diaphysis | 5–20 yrs | Sheets of small round blue cells, PAS+ glycogen | Onion-skin periosteal reaction | CD99 (MIC-2) |
| Metastases | Vertebra, pelvis, ribs, prox long bones | >40 yrs (usually) | Cohesive epithelial cells in fibrous stroma within bone | Lytic (lung/kidney) or blastic (prostate) | CK+, organ-specific (PSA, TTF-1, GATA3) |
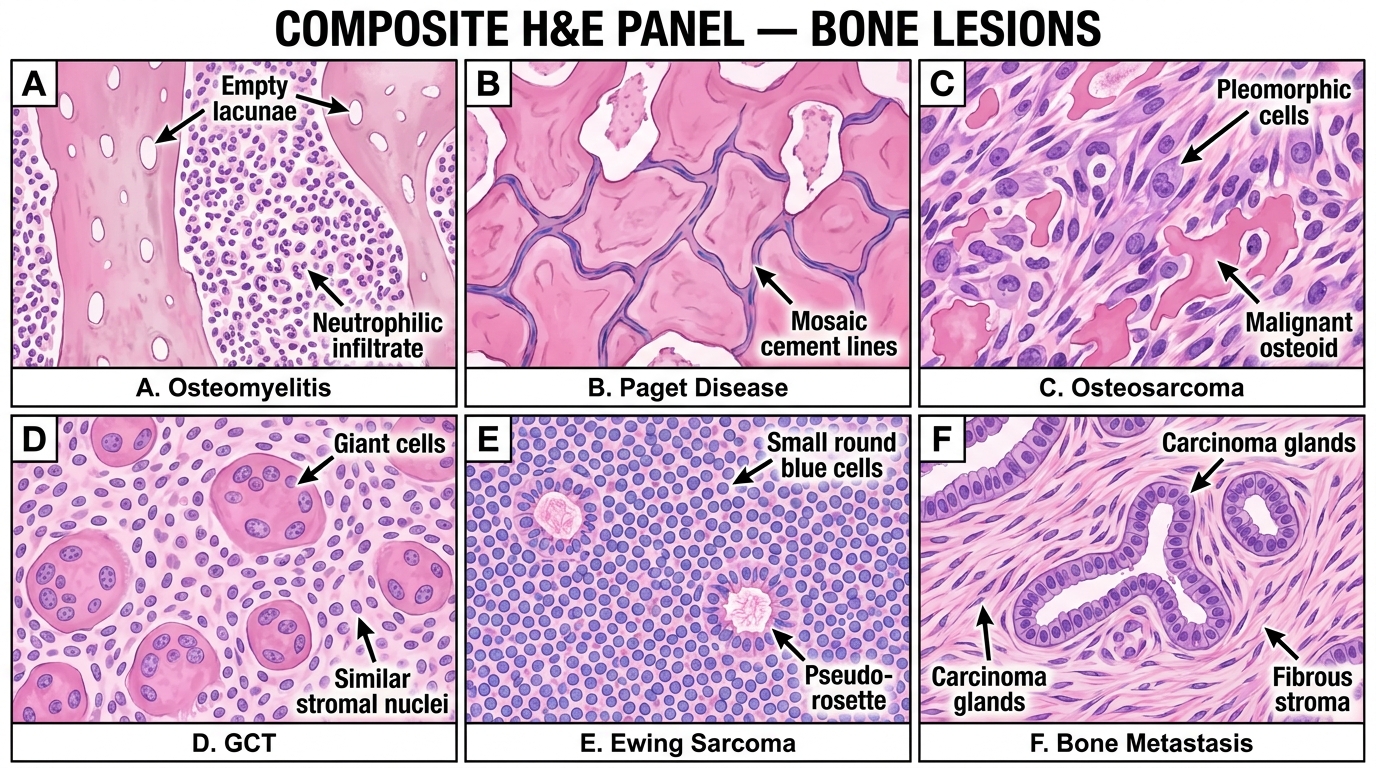
Composite H&E Panel — Diagnostic Bone Lesion Recognition (A–F)
SELF-CHECK
A 14-year-old boy presents with a 3-month history of fever, bone pain, and a tender swelling over the diaphysis of his right femur. X-ray shows an 'onion-skin' periosteal reaction. Biopsy shows sheets of uniform small round blue cells with scant cytoplasm; PAS stain is positive. Which genetic translocation is most likely present?
A. t(9;22) BCR-ABL — Philadelphia chromosome of CML
B. t(11;22)(q24;q12) EWSR1-FLI1 fusion — Ewing sarcoma
C. t(11;14) CCND1-IGH — Mantle cell lymphoma
D. t(14;18) BCL2-IGH — Follicular lymphoma
Reveal Answer
Answer: B. t(11;22)(q24;q12) EWSR1-FLI1 fusion — Ewing sarcoma
The diaphyseal location, onion-skin periosteal reaction, small round blue cells on H&E, and PAS-positive glycogen are the classic quartet for Ewing sarcoma. The characteristic translocation is t(11;22)(q24;q12), creating the EWSR1-FLI1 fusion oncogene. CD99 (MIC-2) would also be strongly positive on IHC. Osteosarcoma occurs at the metaphysis, has malignant osteoid (no small round cells), and has no characteristic translocation. The other translocations are haematological.