Page 9 of 20
PA32.2-3 | Bone & Soft Tissue Tumors — SDL Guide (Part 4)
Rhabdomyosarcoma, Leiomyosarcoma, Fibrosarcoma
Rhabdomyosarcoma (RMS) — most common soft tissue sarcoma in children and adolescents.
- Origin: skeletal muscle (striated) precursors.
- Sites: head and neck (orbit, nasopharynx), genitourinary tract (bladder, vagina — "botryoid" variant), and extremities.
- Embryonal RMS (most common subtype): children <10 years; spindle cells + rhabdomyoblasts (strap cells); botryoid variant has grape-like polypoid growth pattern; favorable prognosis.
- Alveolar RMS: adolescents and young adults; defining molecular marker: t(2;13) PAX3-FOXO1 or t(1;13) PAX7-FOXO1; cells arranged in alveolar spaces (like lung); aggressive, worse prognosis.
- Pleomorphic RMS: rare, adults; highly malignant.
- Histology: cells with deeply eosinophilic cytoplasm, cross-striations (visible in well-differentiated areas — confirm with desmin, myogenin, myoD1 immunostains).
- Spread: both hematogenous (lung) AND lymphatic (unlike most other sarcomas).
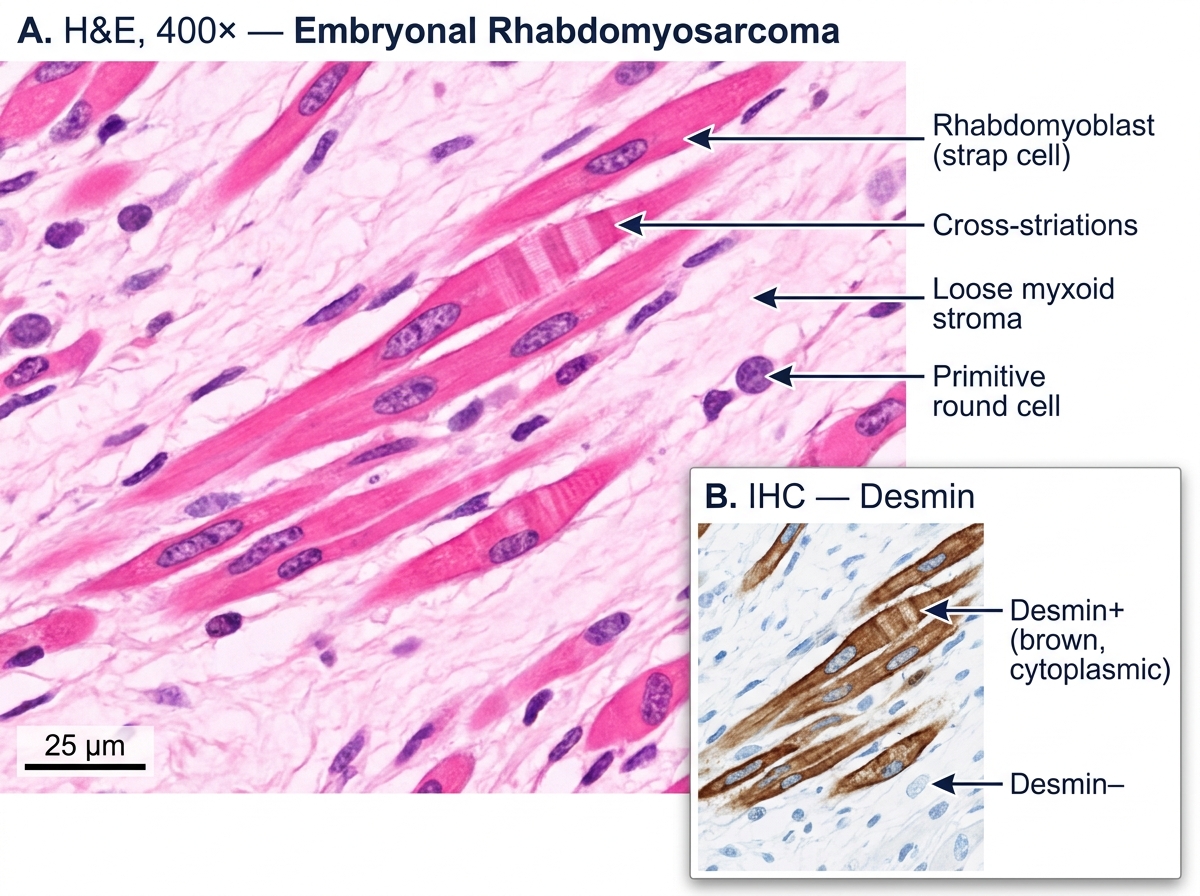
Embryonal Rhabdomyosarcoma — H&E and Desmin IHC (400×)
Leiomyosarcoma (LMS) — malignant smooth muscle tumor; one of the most common soft tissue sarcomas in adults.
- Sites: retroperitoneum, uterus (most common soft tissue sarcoma in women), inferior vena cava, and deep extremities.
- Histology: interlacing bundles of elongated spindle cells with blunt-ended ("cigar-shaped") nuclei and eosinophilic fibrillary cytoplasm. Mitotic figures are key to diagnosis (≥5 mitoses/10 HPF for uterine LMS).
- IHC: smooth muscle actin (SMA) positive, desmin positive, CD117 negative (distinguishes from GI stromal tumor).
- Prognosis: variable; retroperitoneal LMS has poor prognosis due to late detection and large size.
Fibrosarcoma — malignant tumor of fibroblasts.
- Rare in pure form today (most tumors previously called fibrosarcoma are now reclassified with molecular tools).
- Histology: herringbone (fascicular) pattern — interlacing bundles of atypical spindle cells in a chevron arrangement, with scant collagen between cells. No osteoid, no chondroid, no cross-striations.
- Prognosis: intermediate; treatment is wide surgical excision.
Fibrosarcoma Histology — Herringbone Pattern, Spindle Cell Atypia, and Mitosis (H&E)
Synovial Sarcoma
Synovial sarcoma is a high-grade soft tissue sarcoma that deserves separate emphasis because it has a distinctive age group, translocation, and morphology.
Key facts
- Despite the name, it does not arise from synovial cells but from an unspecified mesenchymal precursor that differentiates along synovioblastic lines.
- Age: adolescents and young adults (15–35 years).
- Site: typically around large joints — knee, ankle, and foot; also found in the thigh, paravertebral region, and pleuropulmonary locations.
- Does not arise within the joint cavity — it arises near joints in periarticular soft tissues.
Molecular hallmark: t(X;18)(p11;q11) — SYT-SSX fusion gene; present in >95% of cases; diagnostic by FISH or RT-PCR.
Radiology: soft tissue mass near a joint, often with calcification (30% of cases — a distinguishing feature from most other sarcomas of this age group).
Histology
- Biphasic pattern (classic): two components:
1. Epithelial-like cells — form glands or tubules, resemble carcinoma.
2. Spindle cells — sarcomatous component.
- Monophasic pattern (more common): only spindle cells, no glandular differentiation.
- IHC: TLE1 positive (highly sensitive marker), EMA and CK positive (epithelial markers — unusual for a sarcoma), CD34 negative.
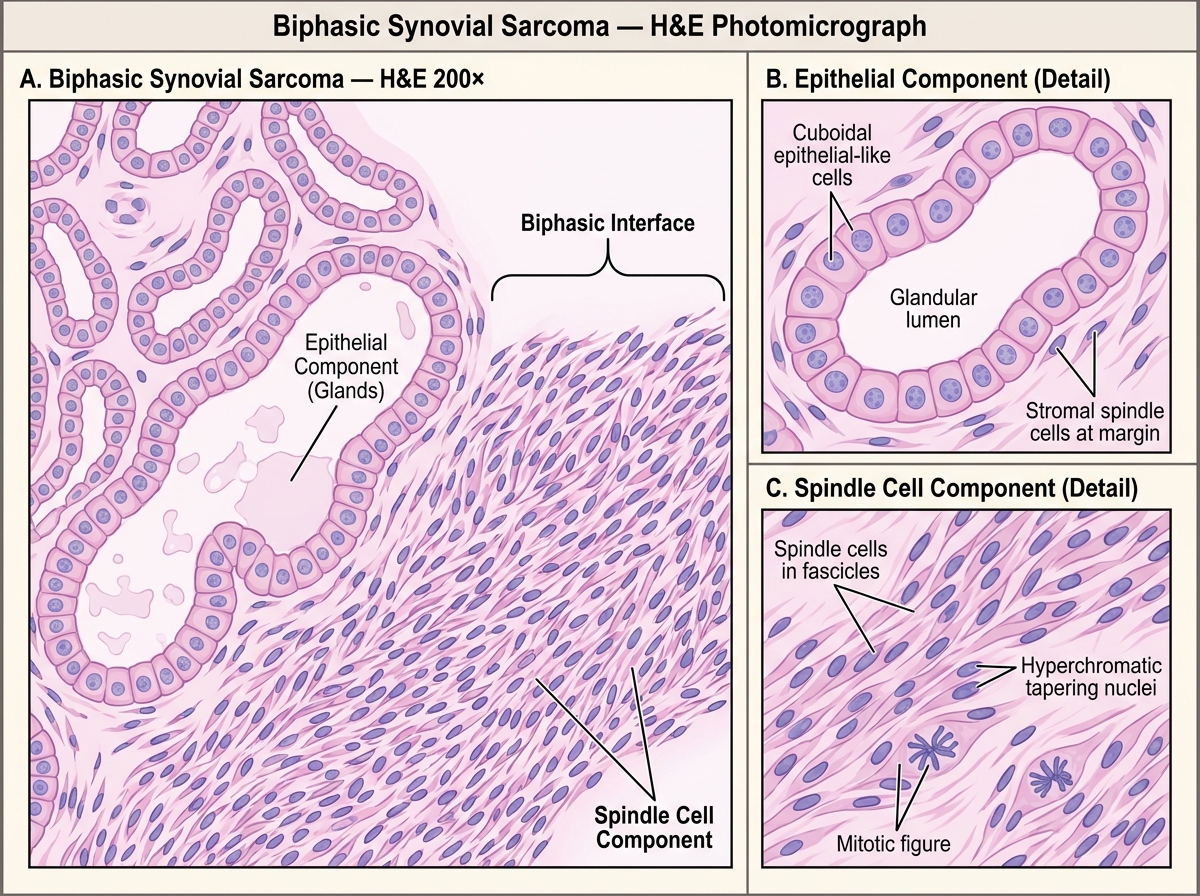
Biphasic Synovial Sarcoma — H&E, 200×: Epithelial and Spindle Cell Components
Spread and prognosis
- Hematogenous spread to lungs; lymph node metastasis in ~20% (unusual for sarcomas).
- 5-year survival ~50–70% for localized disease; poor if metastatic.
- Treatment: wide resection + adjuvant radiation ± chemotherapy (ifosfamide-based).
CLINICAL PEARL
Hematogenous spread to lungs is the rule for sarcomas. Nearly all bone and soft tissue sarcomas — osteosarcoma, Ewing, chondrosarcoma, liposarcoma, leiomyosarcoma, fibrosarcoma — spread primarily via blood to the lungs, NOT to lymph nodes. The exceptions you must memorize for MCQs: rhabdomyosarcoma and synovial sarcoma both spread to lymph nodes (as well as to lungs). When an exam question says 'a soft tissue sarcoma that spreads to lymph nodes', the answer is one of these two. This explains why regional lymph node dissection is considered for RMS and synovial sarcoma but not for most other sarcomas.
SELF-CHECK
A 25-year-old man has a soft tissue mass near his left knee. X-ray shows a periarticular soft-tissue mass with focal calcification. Histology reveals a biphasic pattern with glandular spaces lined by epithelial-like cells embedded in a spindle cell stroma. Which chromosomal translocation confirms this diagnosis?
A. t(11;22) EWSR1-FLI1
B. t(X;18) SYT-SSX
C. t(2;13) PAX3-FOXO1
D. t(12;16) FUS-DDIT3
Reveal Answer
Answer: B. t(X;18) SYT-SSX
Biphasic histology (glandular epithelial + spindle cell components) + periarticular location in a young adult + calcification = synovial sarcoma, defined by t(X;18)(p11;q11) SYT-SSX fusion in >95% of cases. t(11;22) EWSR1-FLI1 = Ewing sarcoma. t(2;13) PAX3-FOXO1 = alveolar rhabdomyosarcoma. t(12;16) FUS-DDIT3 = myxoid liposarcoma.