Page 8 of 20
PA32.2-3 | Bone & Soft Tissue Tumors — SDL Guide (Part 3)
Metastatic Bone Disease
Metastatic bone disease is the most common malignancy involving bone — far more frequent than all primary bone tumors combined. This is a critical epidemiologic fact.
Sources (the 'BBC KT' mnemonic)
The five primary tumors that most commonly metastasize to bone are:
1. Breast cancer (most common in women — osteolytic and mixed lesions)
2. Bladder / Bronchus (lung cancer — usually osteolytic)
3. Colon — rare bony mets in late disease
4. Kidney (renal cell carcinoma — highly vascular, osteolytic, may bleed on biopsy)
5. Thyroid (follicular carcinoma — osteolytic, expansile, "pulsatile bone tumor")
Add prostate cancer — the classic source of osteoblastic (sclerotic) metastases. "Ivory vertebra" (uniformly dense vertebral body) on X-ray in an elderly man = prostatic metastasis until proved otherwise.
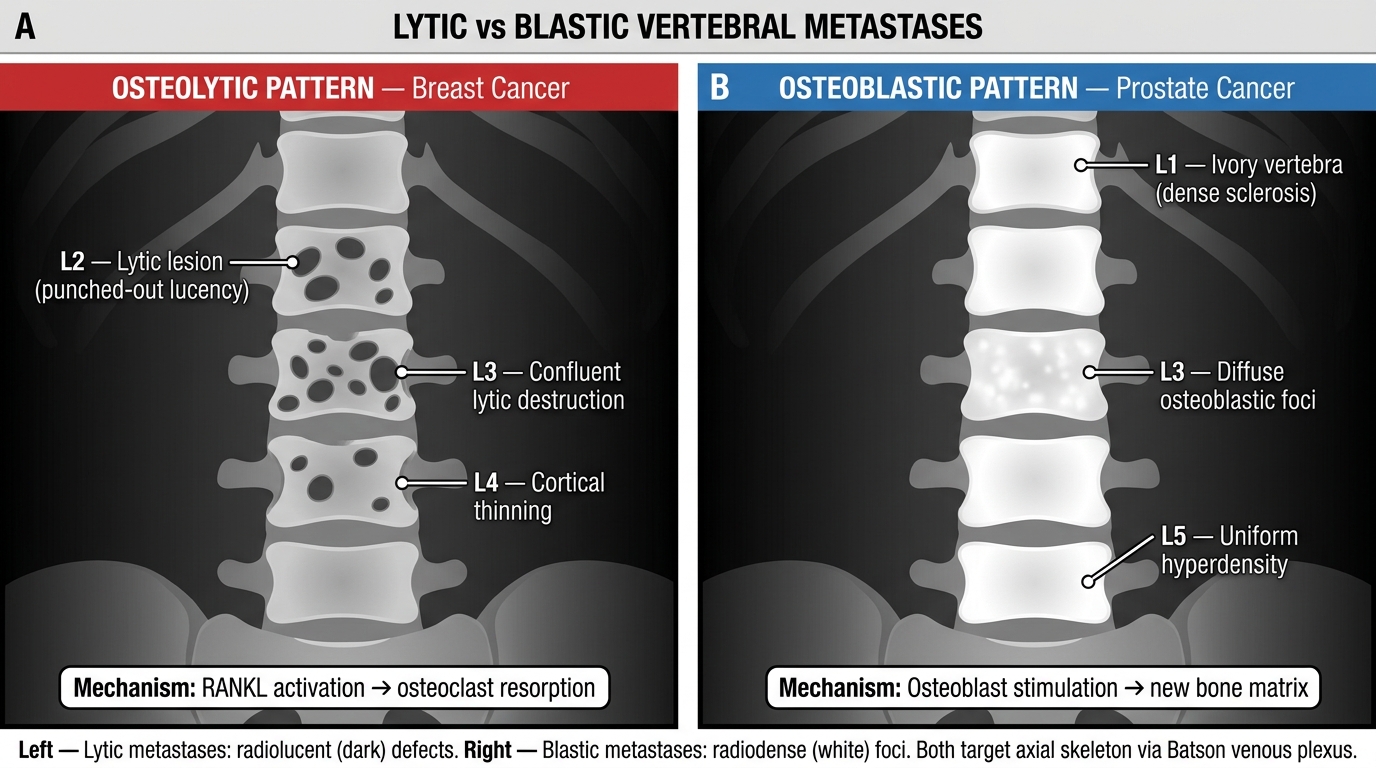
Lytic vs Blastic Vertebral Metastases — Plain X-Ray Comparison
Lytic vs blastic metastases
- Osteolytic: tumor cells destroy bone by activating osteoclasts via RANKL and other cytokines. Appear as punched-out lucencies. Common in: breast, lung, kidney, thyroid, multiple myeloma.
- Osteoblastic: tumor cells stimulate osteoblasts. Appear as dense sclerotic foci. Classic in: prostate cancer.
- Mixed lytic-blastic: breast cancer (most common cause of mixed pattern in women).
Mechanism of spread to bone
- Hematogenous (arterial); Batson's vertebral venous plexus (valveless, low-pressure) explains the predilection for the axial skeleton — vertebrae (especially lumbar), pelvis, ribs, sternum, proximal femur, skull.
Clinical consequences
- Bone pain (the most common symptom of advanced cancer).
- Pathological fracture — especially through lytic lesions in weight-bearing bones (vertebral crush fractures → paraplegia; femoral neck fracture after trivial fall).
- Hypercalcemia — from extensive osteolysis → nausea, confusion, polyuria, constipation ("bones, groans, moans, stones").
- Spinal cord compression from epidural extension of vertebral metastasis — an oncological emergency.
Histology: metastatic deposits typically retain the morphology of the primary — acinar glands (breast or prostate carcinoma), clear cells (renal cell carcinoma), follicular thyroid tissue. Immunohistochemistry (CK7, CK20, PSA, TTF-1, PAX8, GATA3) helps identify the primary.
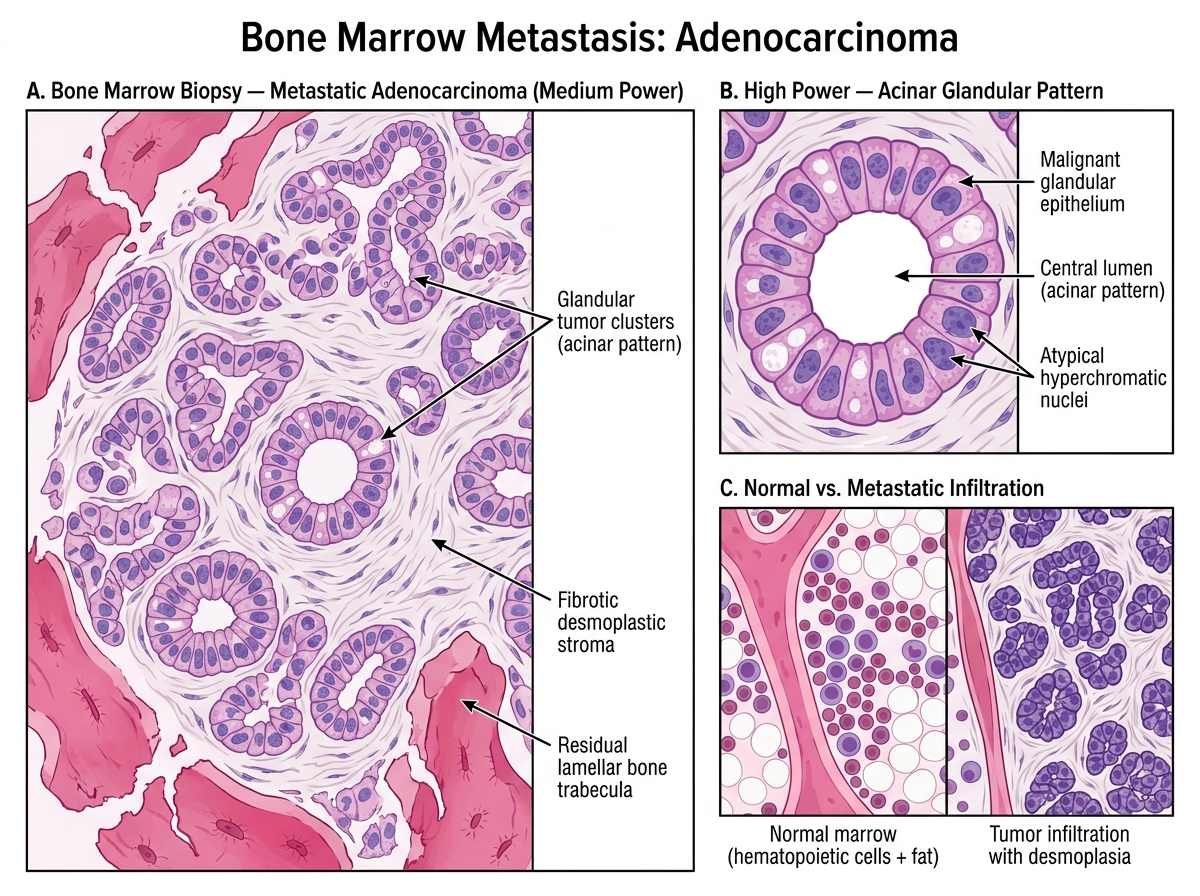
Bone Marrow Biopsy: Metastatic Adenocarcinoma with Acinar Pattern
Soft Tissue Tumors: Principles and Classification
Soft tissue tumors (PA32.3) arise from mesenchymal tissues outside the skeleton — fat, skeletal muscle, smooth muscle, fibrous tissue, synovium, blood vessels, and peripheral nerves.
General principles — apply these to every soft tissue sarcoma:
- Benign soft tissue tumors are far more common than malignant ones — the ratio is approximately 100:1. Every lump is not a sarcoma.
2. Grading (FNCLCC system): sarcomas are graded 1–3 based on:
- Differentiation (how closely the tumor resembles normal tissue)
- Mitotic count (mitoses per 10 high-power fields)
- Necrosis (percentage of tumor showing necrosis)
Higher grade = more aggressive = worse prognosis.
- Staging: TNM (tumor size, lymph node, metastasis) + grade. Size >5 cm and deep location (beneath deep fascia) = higher risk.
4. Routes of spread:
- Primary route: hematogenous to the lungs (most soft tissue sarcomas bypass lymph nodes and go directly to lung).
- Lymph node spread is unusual — exceptions: synovial sarcoma, rhabdomyosarcoma (embryonal), epithelioid sarcoma (these do spread to lymph nodes).
- Local recurrence after inadequate excision is common — margin status is critical.
- Radiology: MRI is the modality of choice for soft tissue sarcomas — delineates tissue planes, extension, and compartment involvement.
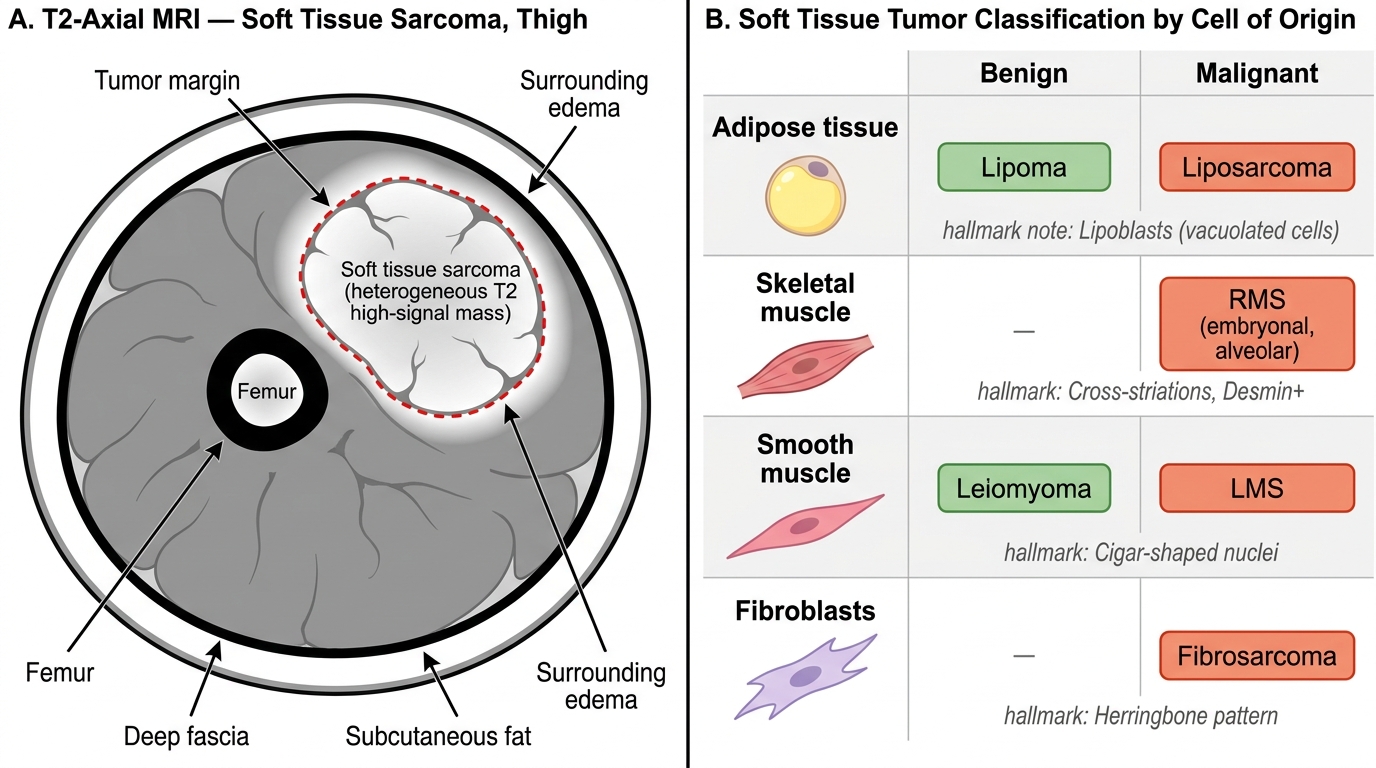
T2 MRI Features of Soft Tissue Sarcoma & Tumor Classification by Cell of Origin
| Tumor | Origin | Benign | Malignant | Hallmark feature |
|---|---|---|---|---|
| Lipoma / Liposarcoma | Adipose tissue | Lipoma | Liposarcoma | Lipoblasts (malignant) |
| Rhabdomyosarcoma | Skeletal muscle | — | RMS (embryonal, alveolar) | Cross-striations, desmin+ |
| Leiomyosarcoma | Smooth muscle | Leiomyoma | LMS | Cigar-shaped nuclei |
| Fibrosarcoma | Fibroblasts | — | Fibrosarcoma | Herringbone pattern |
| Synovial sarcoma | Synovioblasts | — | Synovial sarcoma | Biphasic pattern, t(X;18) |
Lipoma and Liposarcoma
Lipoma — the most common benign soft tissue tumor of adults.
- Lobulated mass of mature adipocytes; well-encapsulated, soft, mobile, non-tender.
- Sites: subcutaneous tissue of trunk, neck, and proximal extremities.
- Radiologic: homogeneous fat-signal mass (similar to adjacent subcutaneous fat on MRI).
- Histology: mature lipocytes, uniform, no atypia, thin fibrous septa.
- Treatment: excision if symptomatic; no malignant potential for ordinary lipoma.
Liposarcoma — the most common soft tissue sarcoma in adults (along with leiomyosarcoma, competing for this position; liposarcoma is first in many classifications).
- Sites: retroperitoneum (most common site, often very large at presentation) and deep thigh.
- Identifying feature on histology: lipoblasts — cells with multiple lipid vacuoles that scallop the hyperchromatic nucleus ("spider-cell" or "signet-ring" with fat vacuoles). The lipoblast is the morphologic hallmark of liposarcoma at any grade.
Histologic subtypes and their prognosis:
| Subtype | Histology | Molecular | Prognosis |
|---|---|---|---|
| Well-differentiated (WDLPS) | Resembles lipoma + scattered atypical stromal cells | MDM2/CDK4 amplification (12q13-15) | Good (locally aggressive, rarely mets) |
| Dedifferentiated | WDLPS + non-lipogenic high-grade sarcoma | MDM2/CDK4 amp | Intermediate |
| Myxoid / round cell | Lipoblasts in myxoid stroma | t(12;16) FUS-DDIT3 | Intermediate to poor |
| Pleomorphic | Marked pleomorphism + lipoblasts | Complex | Poor |
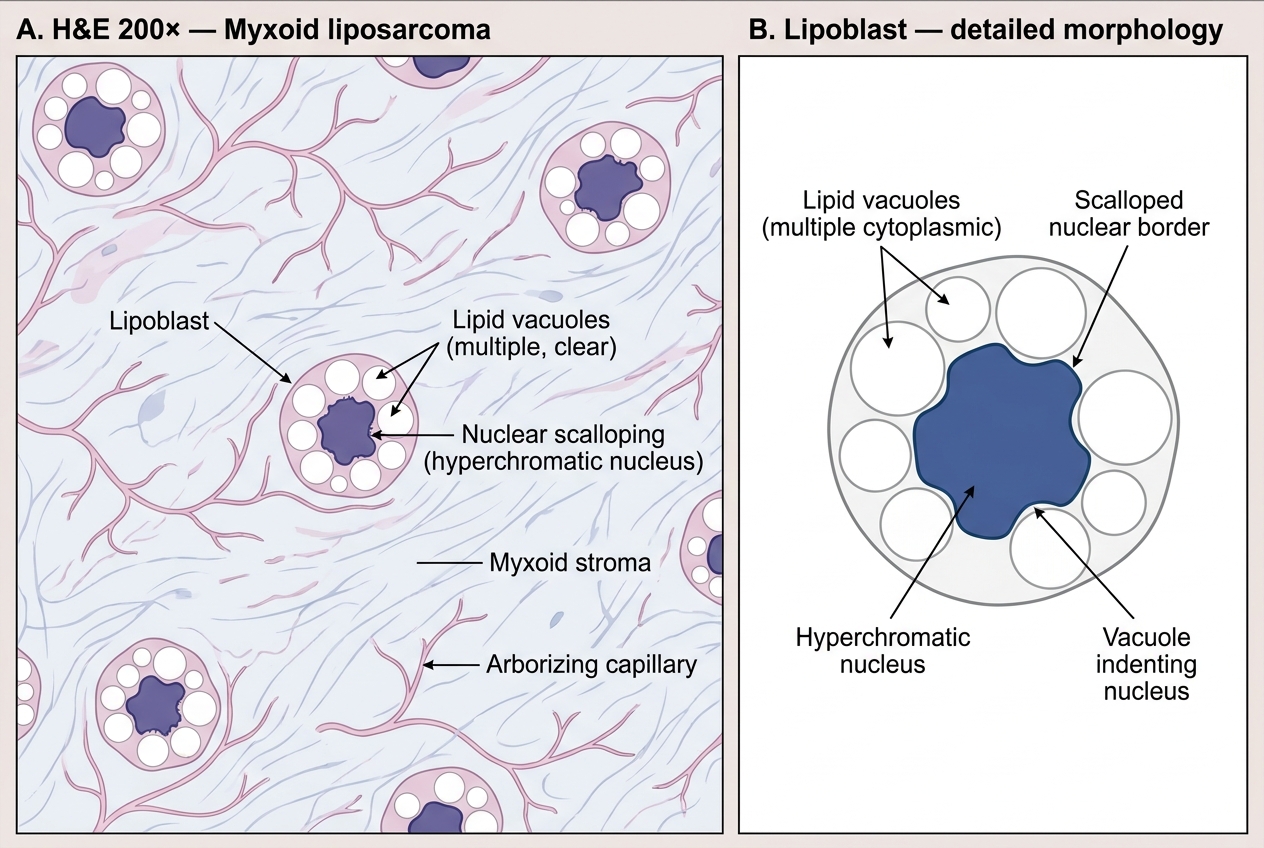
Myxoid Liposarcoma — H&E Histology and Lipoblast Morphology