Page 1 of 20
PA32.{1,4} | Osteomyelitis & Paget Disease of Bone — SDL Guide
Learning Objectives
- Classify osteomyelitis by route of infection (hematogenous vs contiguous) and by organism (pyogenic vs tuberculous)
- Describe the pathogenesis of hematogenous osteomyelitis — explaining why the metaphysis of long bones is the preferential site in children
- Define and distinguish sequestrum, involucrum, cloaca, and Brodie abscess — the hallmark morphological features of pyogenic osteomyelitis
- Identify the radiological features of acute and chronic osteomyelitis
- List the complications of chronic osteomyelitis, including secondary amyloidosis, sinus tract, Marjolin ulcer, and septic arthritis
- Describe Pott disease (tuberculous spondylitis) — the most clinically important form of TB osteomyelitis in the Indian context
- Explain the etiology and pathogenesis of Paget disease of bone (osteitis deformans), including the viral hypothesis and SQSTM1 mutations
- Describe the three phases of Paget disease (osteolytic → mixed → osteosclerotic) and their distinctive radiological and morphological correlates
- Identify the mosaic/jigsaw cement-line pattern as the pathognomonic microscopic feature of Paget disease
- List the complications of Paget disease — fractures, nerve compression, high-output cardiac failure, and osteosarcoma transformation
INSTRUCTIONS
Bone infections and bone remodeling disorders are among the most clinically significant lesions you will encounter in surgical pathology and radiology. Osteomyelitis remains a leading cause of long-term disability in children across India — and Paget disease, though more common in the elderly in Western countries, presents with deceptive complications that kill or maim if missed. This module builds from normal bone biology, through the pathogenesis of infection and abnormal remodeling, to the morphological and radiological patterns you will be tested on in exams and expected to recognise in clinical practice. Approach each section with the question: how does the structural disruption I am learning about explain the sign, symptom, or X-ray finding in front of me?
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 26 — Bones, Joints & Soft Tissue Tumors (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-year-old boy is brought to the casualty with high fever and a swollen, tender right thigh for three days. He refuses to walk. X-ray is normal. You send him home with antibiotics. A week later he's back — now there's a discharging sinus from his thigh. The X-ray now shows a dense white fragment of bone floating free inside a cavity. You've missed the window to cure him with antibiotics alone.
Meanwhile, in the geriatric ward: an 82-year-old retired teacher is found to have a serum alkaline phosphatase four times the upper limit of normal on a routine screen. His skull X-ray looks like someone scattered cotton wool across it. He is told he has "Paget disease" — a name that means almost nothing to him and too little to the junior doctor ordering the test.
These two patients — decades apart in age, entirely different diseases — share one common thread: the pathologist who understands what is happening inside their bone is the one who can connect the gross, the microscopic, the radiological, and the clinical into a single coherent story. That is what this module teaches.
WHY THIS MATTERS
Osteomyelitis and Paget disease are core NMC CBUC competencies (PA32.1 and PA32.4) and appear in both written and viva examinations at SBV. Beyond exams, these conditions matter in daily practice:
- Osteomyelitis is a surgical emergency when caught early (IV antibiotics cure it), a chronic disability when missed (sequestrum, sinus tract, amputation). In India, post-traumatic and post-surgical osteomyelitis is rising with road traffic injuries. Haematogenous OM in children is a paediatric urgency you will see in casualty.
- Pott disease (spinal TB) is directly relevant to our patient population — India bears 26% of global TB burden; spinal TB is the commonest extra-pulmonary skeletal TB and a preventable cause of paraplegia.
- Paget disease may present first to a pathologist (via raised ALP on a blood panel), then to a radiologist (incidental X-ray finding), then to an orthopaedic surgeon (pathological fracture or sarcoma). Knowing the three phases means you can interpret ALP trends and bone scan findings — skills that bridge laboratory and clinical medicine.
These are also patterns you will see in histopathology practical sessions, so linking the gross description to the slide is a direct exam benefit.
RECALL
Before we dive into infection and disease, anchor yourself to normal bone biology — we will return to every concept below when we explain why disease disrupts it.
Normal bone structure (brief anchor):
• Bone is a connective tissue with an organic matrix (osteoid — mainly type I collagen) and an inorganic mineral phase (hydroxyapatite — calcium phosphate crystals)
• Three cell types maintain bone: osteoblasts (form bone — lay down osteoid), osteoclasts (resorb bone — multinucleated giant cells from monocyte lineage), osteocytes (maintain matrix, mechanosensing)
• Normal bone is lamellar — collagen fibres arranged in parallel sheets, giving it tensile strength. Under polarised light, lamellar bone shows alternating bright and dark bands (birefringence).
• Woven bone is the rapidly-formed, mechanically inferior type: collagen fibres run in random directions. It is normal in the foetus and in fracture callus; its presence in an adult is a red flag for pathological bone turnover.
• Bone remodeling — osteoclast resorption followed by osteoblast deposition — is a continuous, tightly coupled process. Normal serum alkaline phosphatase (ALP) reflects osteoblast activity; abnormal elevation signals excessive bone formation.
• Blood supply: the metaphysis of long bones has rich, slow-flowing sinusoidal vascular loops — important in the next section.
Hold these concepts. They directly explain the pathogenesis of what follows.
Osteomyelitis: Classification & Overview
Osteomyelitis (from Greek osteon = bone + myelos = marrow + itis = inflammation) is infection of bone and bone marrow. It is classified by two independent axes:
Axis 1 — Route of infection:
| Route | Typical age/setting | Key pathogens |
|---|---|---|
| Hematogenous | Children (long bone metaphysis) | S. aureus (most common overall) |
| Contiguous spread | Adults (post-trauma, post-surgery, diabetic foot) | Polymicrobial, Pseudomonas, anaerobes |
| Direct inoculation | Any age (open fracture, surgery) | S. aureus, gram-negatives |
Axis 2 — Causative organism:
• Pyogenic — Staphylococcus aureus accounts for 80–90% of all cases. Other agents: Streptococcus, E. coli, Pseudomonas, Klebsiella.
• Special hosts: Sickle cell disease → Salmonella typhi osteomyelitis (classic viva question). IV drug users → Pseudomonas aeruginosa (vertebrae).
• Granulomatous — Mycobacterium tuberculosis (covered separately as Pott disease), rarely fungi.
Temporal classification:
• Acute (< 6 weeks) — active suppurative infection; responds to antibiotics if caught early
• Subacute (6 weeks – 3 months) — indolent; includes Brodie abscess
• Chronic (> 3 months) — devitalised bone + sinus tracts; requires surgical debridement
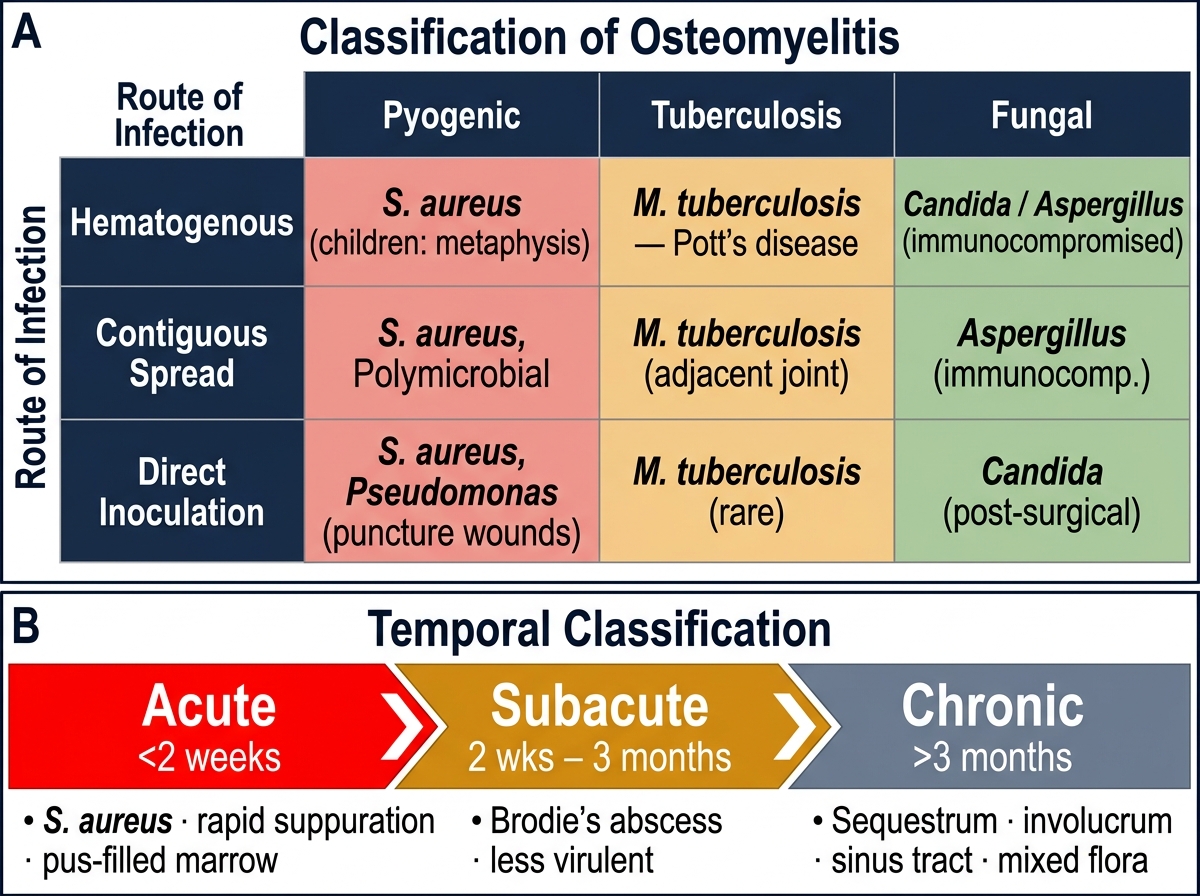
Classification of Osteomyelitis: Route, Organism, and Temporal Axes
Hematogenous Osteomyelitis: Pathogenesis in Children
Hematogenous osteomyelitis is the classic childhood form. Understanding why infection lodges in the metaphysis requires you to trace the sequence from bacteremia to bone destruction.
Step 1 — Bacteremia. A transient bacteremia (following a skin pustule, upper respiratory infection, or minor trauma) seeds the bloodstream with bacteria, most often S. aureus.
Step 2 — Metaphyseal lodgment. The metaphysis of long bones (distal femur > proximal tibia > proximal humerus) has unique vascular anatomy:
• Terminal sinusoidal vascular loops slow blood flow dramatically
• Phagocytic activity is relatively reduced here (few local macrophages)
• The sinusoids lack tight junctions, allowing bacteria to extravasate easily
Result: bacteria seed the metaphysis preferentially — this explains the clinical and radiological predilection site.
Step 3 — Suppuration. Bacteria multiply → acute inflammatory response → neutrophil exudate fills the marrow space → suppurative (pus-forming) osteomyelitis.
Step 4 — Pressure buildup. Bone is a rigid container. Pus has nowhere to go:
• Pressure rises → ischemic necrosis of surrounding bone
• Pus burrows under the periosteum (subperiosteal abscess) → strips it away → cuts off periosteal blood supply → more necrosis
• In children < 1 year, vessels cross the epiphyseal plate → pus can spread to joint → septic arthritis (important complication)
Step 5 — Sequestrum formation. The segment of bone that loses blood supply becomes a sequestrum — dead, necrotic bone that cannot be resorbed by osteoclasts (they need living bone).
Step 6 — Involucrum. Surviving periosteum responds by forming new bone around and outside the infected zone — this reactive shell is the involucrum (Latin: involucrum = wrapping).
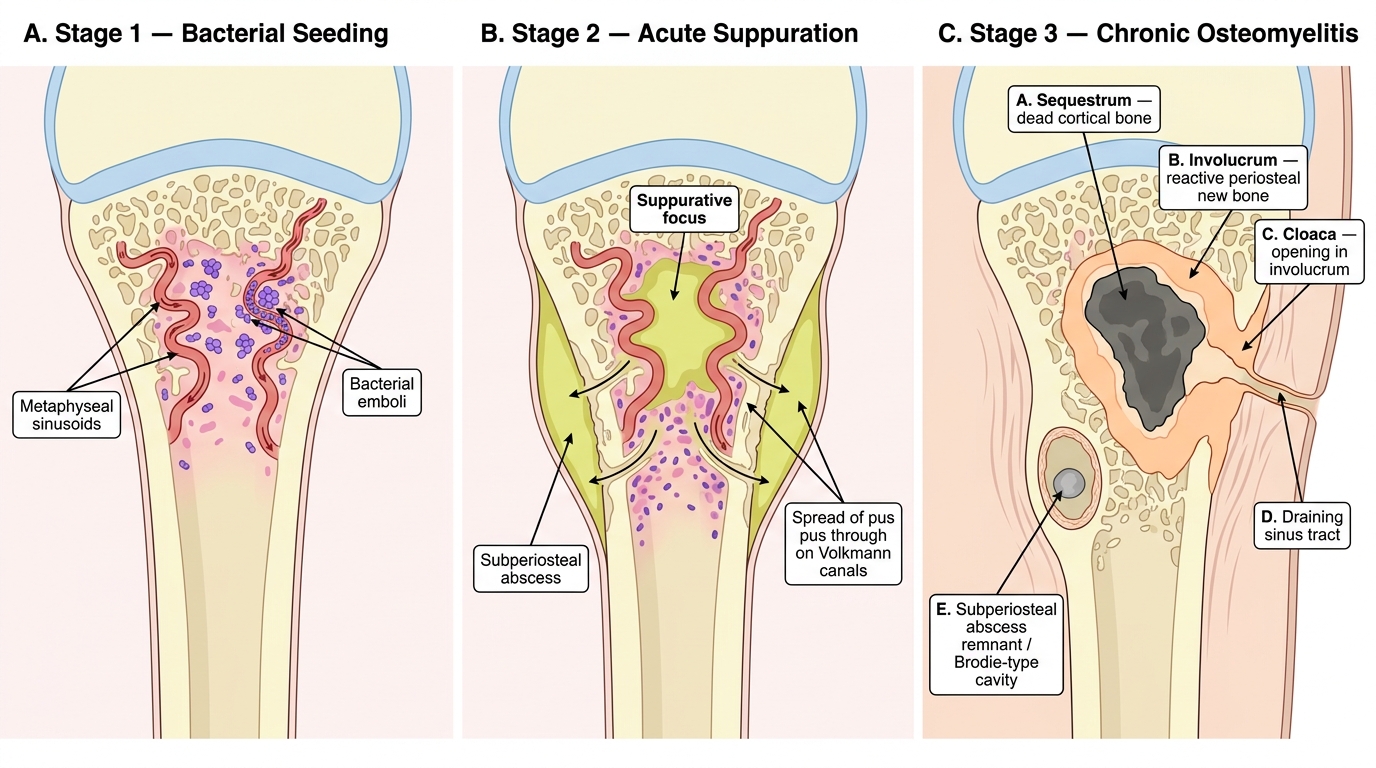
Pathogenesis of Hematogenous Osteomyelitis in the Paediatric Long Bone (Three Stages)
Morphology of Pyogenic Osteomyelitis: The Key Landmarks
Five morphological terms are essential and high-yield for examinations:
1. Sequestrum
• Fragment of dead (necrotic) cortical bone surrounded by pus or granulation tissue
• Appears pale, devitalised; osteocytes are absent (empty lacunae)
• Cannot be resorbed — acts as a permanent nidus of infection
• On X-ray: dense white fragment floating inside a lytic cavity (high-density because necrotic bone does not remodel)
2. Involucrum
• Reactive new bone shell formed by the stripped periosteum encasing the sequestrum
• Histologically: woven bone (rapid formation) initially, later remodels to lamellar bone
• On X-ray: thick, irregular, periosteal new bone formation surrounding the infection
3. Cloaca
• Opening in the involucrum (and periosteum) through which pus and small fragments of sequestrum can be discharged
• Connects the focus to the skin surface via a sinus tract
• Latin: cloaca = sewer
4. Brodie abscess
• A walled-off, subacute/chronic lytic cavity — usually in the cancellous bone of the metaphysis (distal tibia is classic)
• Lined by granulation tissue; may contain a small sequestrum
• Organism is S. aureus; the abscess forms when host defences partially contain the infection
• X-ray: well-defined oval lytic lesion with a sclerotic rim in the metaphysis — can mimic an osteoid osteoma or Ewing sarcoma on imaging
5. Sinus tract (discharging sinus)
• Epithelialised channel from the sequestrum/involucrum through soft tissue to the skin
• Chronically discharges pus — the body's way of draining what it cannot resorb
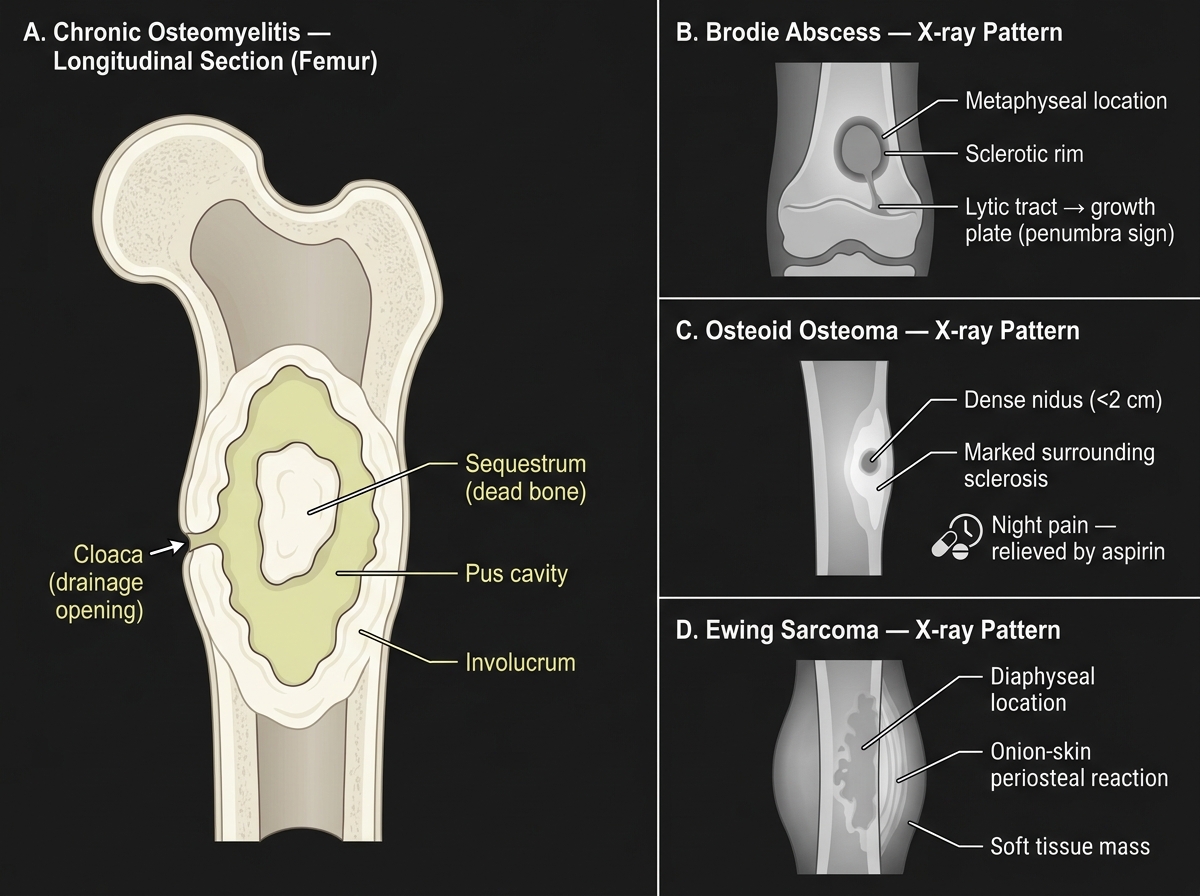
Chronic Osteomyelitis — Gross Anatomy and Differential Diagnosis
CLINICAL PEARL
Brodie abscess vs bone tumour on X-ray — this causes diagnostic panic because a well-defined lytic lesion with sclerotic rim in a teenager looks like it could be a primary bone tumour (Ewing sarcoma, osteoid osteoma). The distinguishing features:
• Brodie abscess: metaphyseal location, sclerotic rim, often with a 'tongue' of lytic tract heading toward the growth plate (the "penumbra" sign on MRI)
• Osteoid osteoma: dense nidus (<2 cm) with marked surrounding sclerosis; intense night pain relieved by aspirin
• Ewing sarcoma: diaphyseal, aggressive periosteal reaction ("onion-skin"), soft tissue mass
When in doubt: MRI + bone biopsy. Do not treat a Brodie abscess as a tumour — you will miss a curable infection.