Page 2 of 20
PA32.{1,4} | Osteomyelitis & Paget Disease of Bone — SDL Guide (Part 2)
Radiological Features of Osteomyelitis
Radiology follows a temporal sequence that directly mirrors the pathology:
Acute phase (days 1–10 — X-ray may be NORMAL)
• X-rays: soft tissue swelling only; bone changes appear only after 30–50% of bone is destroyed — this is the clinical trap from the opening story
• Bone scan (Tc-99m) is positive within 24–48 hours — the gold standard for early detection
• MRI is the most sensitive early imaging: marrow edema (T2 hyperintense signal) before X-ray changes
Subacute to chronic phase
• Periosteal reaction — new bone laid down by the periosteum (involucrum) appears as a thin or thick line parallel to the cortex
• Lytic lesion — focal area of bone destruction within the metaphysis
• Dense sequestrum — high-density dead bone fragment within the lytic cavity (pathognomonic when present)
• Cortical thickening and sclerosis — in chronic disease, reactive bone formation predominates
CT scan is excellent for detailing sequestrum morphology and planning surgery (debridement, sequestrectomy).
| Feature | Acute OM | Chronic OM |
|---|---|---|
| X-ray | Normal or soft tissue swelling | Lytic cavity + dense sequestrum + sclerosis |
| Periosteum | Early elevation | Thick involucrum |
| Bone scan | Positive early | Positive (less specific) |
| MRI | Marrow edema (T2↑) | Complex mixed signal, sinus tracts |
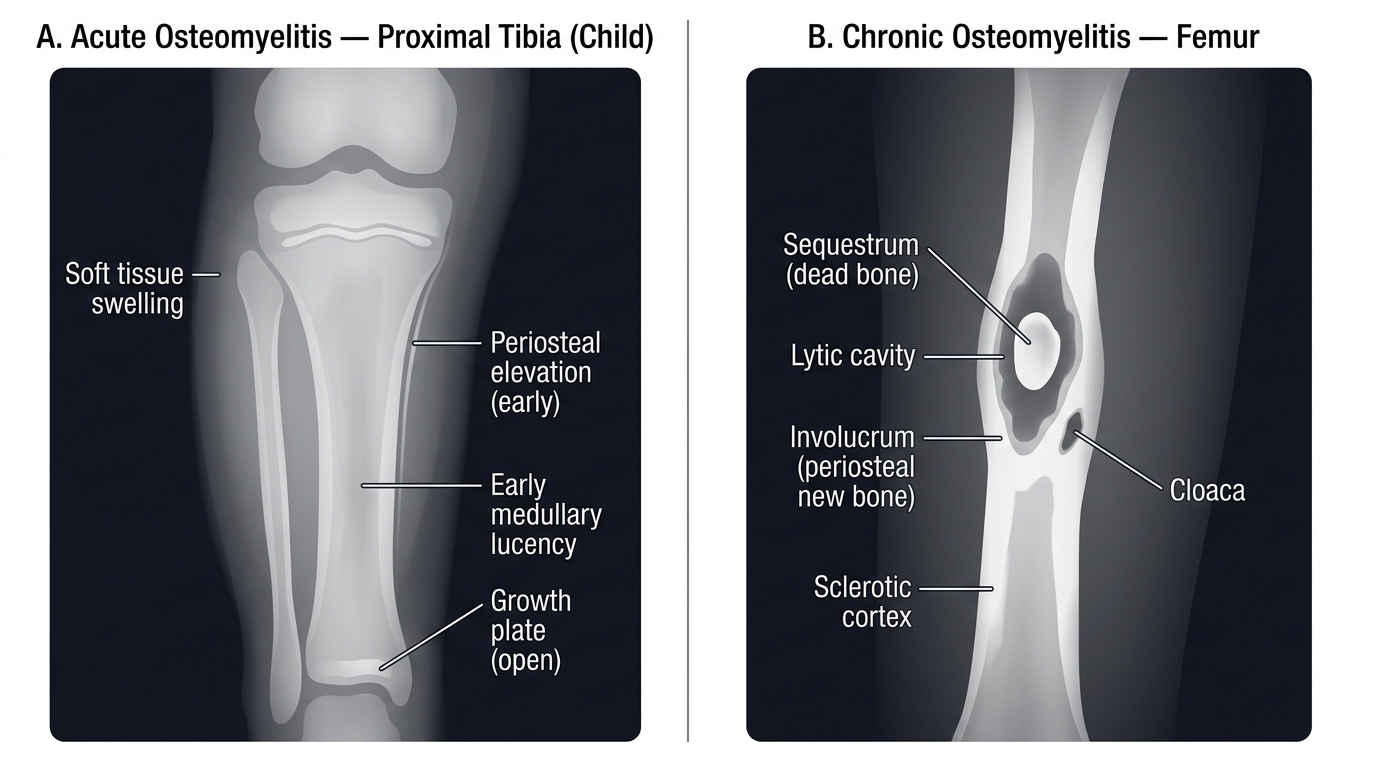
Radiological Features of Acute vs Chronic Osteomyelitis
Complications of Osteomyelitis
Missed or inadequately treated osteomyelitis carries serious long-term consequences:
Local complications:
• Chronic osteomyelitis — the most common complication; persistent infection with intermittent flares; difficult to eradicate without surgical removal of the sequestrum
• Septic arthritis — pus breaches the joint; common in infants where metaphyseal vessels cross the epiphyseal plate; also at hip (where metaphysis is intracapsular)
• Pathological fracture — weakened bone fractures through the infected zone
• Growth disturbance — infection at or near the growth plate → premature fusion → limb length discrepancy in children
Sinus tract complications:
• Secondary (AA) amyloidosis — chronic suppuration drives sustained acute-phase response → overproduction of serum amyloid A (SAA) → SAA deposits as amyloid fibrils in kidney, liver, spleen → proteinuria, nephrotic syndrome, renal failure
• Marjolin ulcer — squamous cell carcinoma (SCC) arising in the chronically inflamed, epithelialised sinus tract; latency period 20–40 years; highly aggressive, metastasises early. This is a classic "chronic wound → malignancy" transformation and a high-yield exam question.
Systemic:
• Septicaemia and septic shock — in acute, inadequately treated cases
• Endocarditis, meningitis, pneumonia — via hematogenous seeding from the infected focus
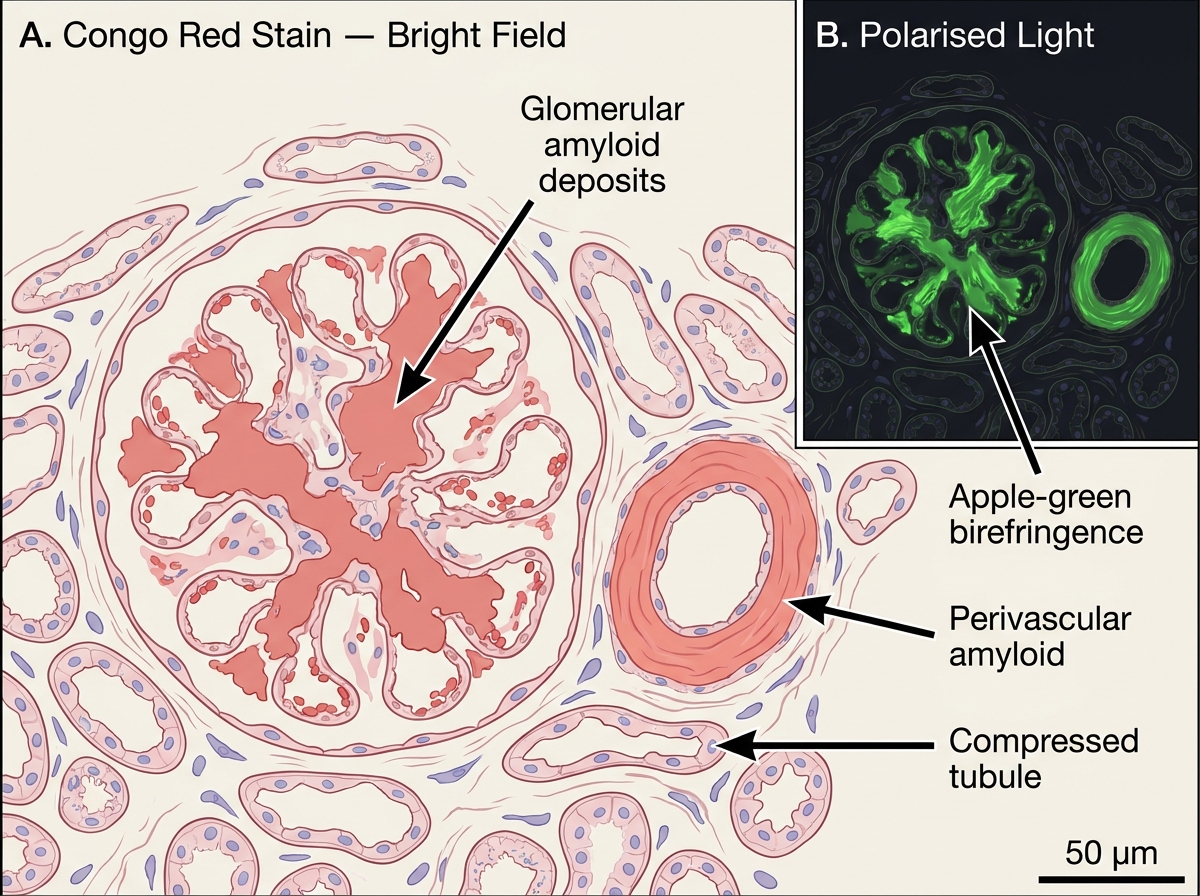
Renal AA Amyloidosis — Congo Red Stain (Bright Field and Polarised Light)
Tuberculous Osteomyelitis: Pott Disease of the Spine
Tuberculous osteomyelitis is caused by Mycobacterium tuberculosis reaching bone via hematogenous spread from a primary (usually pulmonary) focus. In India, it is the most important form of bone TB and a major cause of preventable paraplegia.
Site predilection: Vertebral column — thoracolumbar junction (T10–L2) is most commonly affected, though any vertebra can be involved. This is "Pott disease" (named after Percivall Pott, 1779).
Pathogenesis:
1. Bacteria seed the anterior subchondral bone of a vertebral body via arterial supply
2. Caseating granulomatous inflammation destroys vertebral bone — note: no sequestrum (TB causes caseation, not pus; organisms survive in caseous material)
3. Infection spreads under the anterior longitudinal ligament to adjacent vertebrae → characteristic involvement of two or more adjacent vertebral bodies ("skip lesions" are unusual in TB, unlike pyogenic OM)
4. Infected caseous material tracks along fascial planes → cold (paraspinal) abscess — "cold" because there is no heat, redness, or tenderness (granulomatous inflammation, not acute suppuration)
Morphology:
• Caseating granulomas — central caseous necrosis surrounded by epithelioid macrophages, Langhans giant cells, lymphocytes
• No sequestrum; the destroyed bone is replaced by caseous material
• Intervertebral disc destruction — unlike pyogenic vertebral OM, which often spares the disc early; TB destroys the disc along with bone
Radiological features:
• Anterior vertebral body erosion → vertebral collapse → wedge deformity
• "Gibbus" deformity — sharp angular kyphosis at the site of collapse ("hunchback" — historic term)
• Paraspinal cold abscess — fusiform soft-tissue shadow beside the spine on AP chest X-ray ("psoas abscess" at lumbar levels)
• Disc space loss (early, distinguishes from metastasis)
Complications: Paraplegia ("Pott paraplegia") from cord compression by abscess or bone collapse; sinus tract; secondary amyloidosis in prolonged cases.
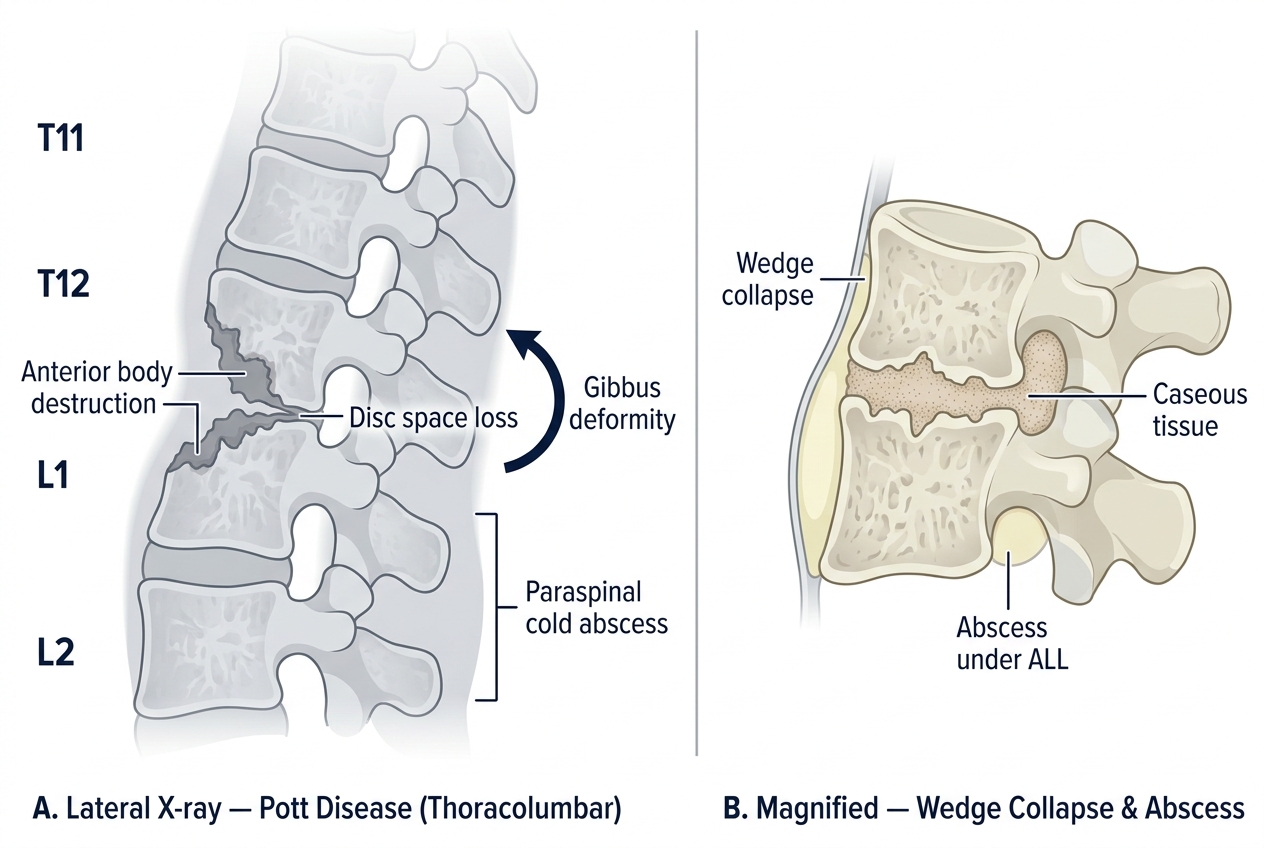
Pott Disease — Lateral Spinal X-ray Features & Wedge Collapse Mechanism
SELF-CHECK
A 7-year-old boy with fever and knee pain for 5 days has a normal X-ray but a strongly positive bone scan. Blood culture grows Staphylococcus aureus. Which anatomical feature of this site best explains why bacteria preferentially lodge here in children?
A. Thin cortex in the epiphysis allows easy bacterial penetration
B. Metaphyseal sinusoidal loops with slow flow and reduced phagocytic activity
C. Direct continuity of the metaphysis with the joint space
D. High osteoclast activity in the metaphysis dissolves bacterial capsules
Reveal Answer
Answer: B. Metaphyseal sinusoidal loops with slow flow and reduced phagocytic activity
The metaphyseal sinusoidal vascular loops are the key. They have markedly slowed blood flow, lack tight junctions (allowing bacterial extravasation), and have relatively reduced local phagocytic activity — creating a perfect nidus for bacterial seeding during bacteremia. This explains why hematogenous OM in children targets the metaphysis of long bones (distal femur, proximal tibia). Option A is wrong — the epiphysis is not the preferential site. Option C describes septic arthritis risk (when metaphysis is intracapsular — e.g., the hip), not the reason bacteria lodge there. Option D is false.
CLINICAL PEARL
Sickle cell disease → Salmonella osteomyelitis. This is one of the most reliably tested associations in pathology examinations. In sickle cell disease:
• Vaso-occlusive crises cause repeated infarcts of the intestinal mucosa → transient bacteremia with gut organisms (especially Salmonella typhi and non-typhi Salmonella)
• Splenic autoinfarction removes the spleen's bacteremia-clearing function
• Result: Salmonella species are the most common cause of OM in sickle cell patients (in the general population S. aureus dominates)
Remember the mnemonic: Sickle = Salmonella (both start with S).
Second pearl: Pseudomonas aeruginosa is the organism to remember in two other special settings — (1) IV drug users (vertebral OM), and (2) puncture wounds through the sole of a sneaker (implantation).