Page 3 of 20
PA32.{1,4} | Osteomyelitis & Paget Disease of Bone — SDL Guide (Part 3)
Paget Disease of Bone: Etiology & Pathogenesis
Paget disease of bone (osteitis deformans) is a focal disorder of bone remodeling characterised by markedly increased but chaotic bone turnover, producing structurally disorganised, enlarged, and mechanically weakened bone.
Epidemiology:
• Affects 1–3% of adults over 55 years in Western countries; less common in Asia (but seen in India)
• Polyostotic (multiple bones) in 70%; monostotic in 30%
• Most commonly: pelvis > lumbar spine > skull > femur > tibia
Etiology (two hypotheses, both partially supported):
1. Viral hypothesis — slow virus infection of osteoclast precursors
• Nuclear and cytoplasmic inclusions in Pagetic osteoclasts resemble paramyxovirus nucleocapsids
• Measles virus RNA and respiratory syncytial virus (RSV) antigens have been detected in Pagetic osteoclasts
• However, causal proof remains elusive and Paget disease has declined in incidence in countries with measles vaccination — indirectly supportive
2. Genetic hypothesis
• SQSTM1 gene mutations (sequestosome-1, also called p62) are found in 30–50% of familial Paget disease
• SQSTM1/p62 is a scaffold protein in the NF-κB signalling pathway — mutations make osteoclasts hyperresponsive to RANKL, causing excessive osteoclast activation
• Autosomal dominant inheritance
Pathogenesis (the common final pathway, regardless of trigger):
1. Osteoclast hyperactivation — Pagetic osteoclasts are giant, hypernucleated (up to 100 nuclei; normal = 3–5) and extremely active
2. Massive bone resorption → marrow replaced by fibrovascular stroma
3. Osteoblasts respond vigorously to the resorption signal → rapid new bone formation
4. But the new bone is woven (disorganised) → progressively replaced by lamellar bone laid down in irregular patterns
5. Result: enlarged, structurally disorganised bone — strong in bulk, but brittle and prone to fracture
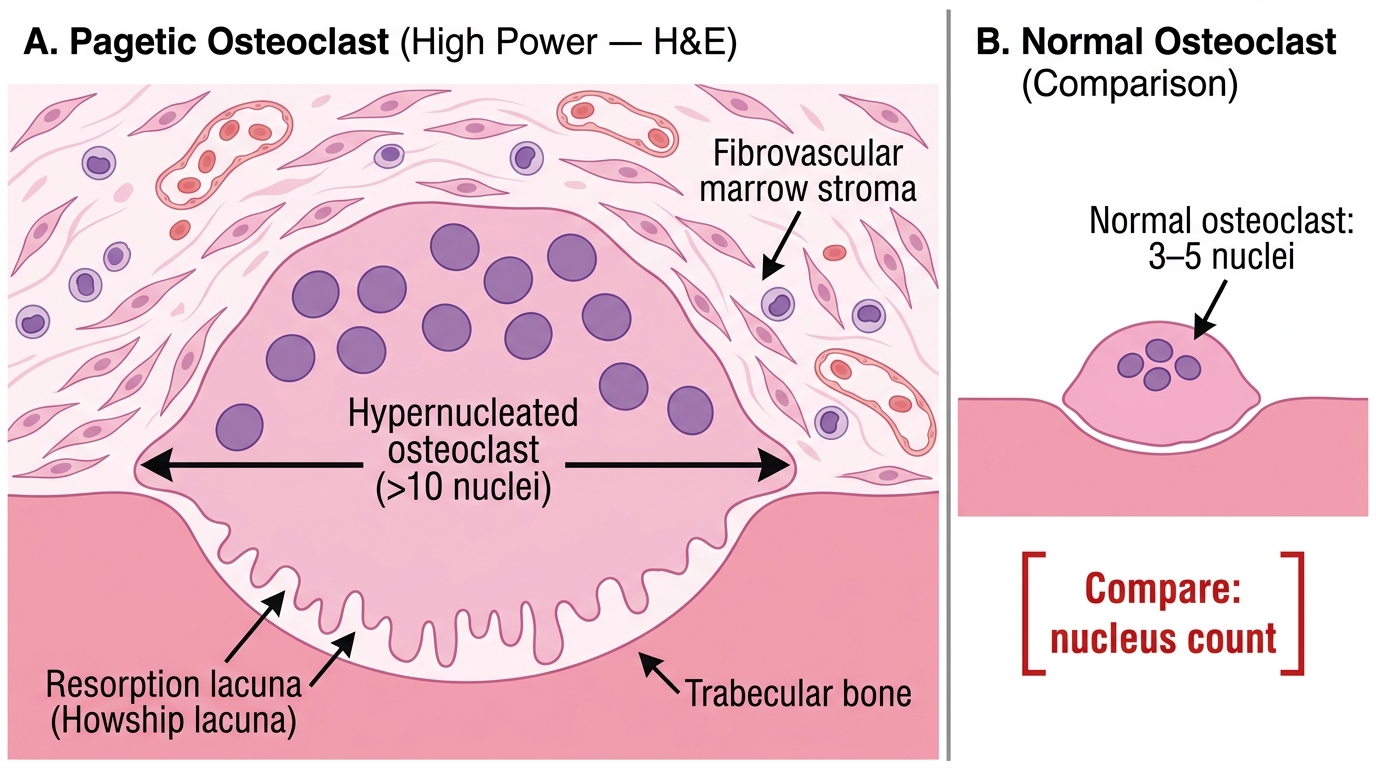
Pagetic Osteoclast: Hypernucleation and Resorption Lacuna (H&E, High Power)
Paget Disease: Three Phases — Radiological & Pathological Correlates
Paget disease evolves through three sequential phases, each with distinct pathological and radiological signatures:
Phase 1 — Osteolytic ("hot" phase)
• Pathology: Dominant osteoclast activity; bone resorption exceeds formation; marrow replaced by hypervascular fibrous stroma
• Radiology: Advancing lytic front ("blade of grass" or "V-shaped" osteolysis in long bones; "osteoporosis circumscripta" — well-defined lytic lesion — in skull)
• Serum markers: Elevated urinary hydroxyproline (collagen breakdown product)
Phase 2 — Mixed (active, transitional) phase
• Pathology: Both osteoclasts AND osteoblasts hyperactive simultaneously; disorganised woven and lamellar bone laid down; mosaic/jigsaw cement-line pattern begins to emerge
• Radiology: Combined lytic and sclerotic areas in the same bone; cortical thickening; bone enlargement
• Serum markers: Markedly elevated serum alkaline phosphatase (ALP) — reflects intense osteoblast activity; highest levels in this phase
Phase 3 — Osteosclerotic ("burnt-out") phase
• Pathology: Osteoclast activity subsides; osteoblasts fill in with sclerotic, mosaic lamellar bone; hypervascular stroma replaced
• Radiology: Dense, thickened, enlarged bone; "cotton-wool" skull (patchy sclerosis over calvarium); "ivory vertebra" (uniformly dense vertebral body)
• Serum markers: ALP remains elevated but may plateau
Summary table:
| Phase | Dominant cell | Radiology | ALP |
|---|---|---|---|
| Osteolytic | Osteoclast | Osteoporosis circumscripta (skull); V-lysis (long bone) | Mildly ↑ |
| Mixed | Both | Combined lytic + sclerotic; bone enlargement | Markedly ↑ |
| Osteosclerotic | Osteoblast | Cotton-wool skull; ivory vertebra; expanded bone | ↑ (plateau) |
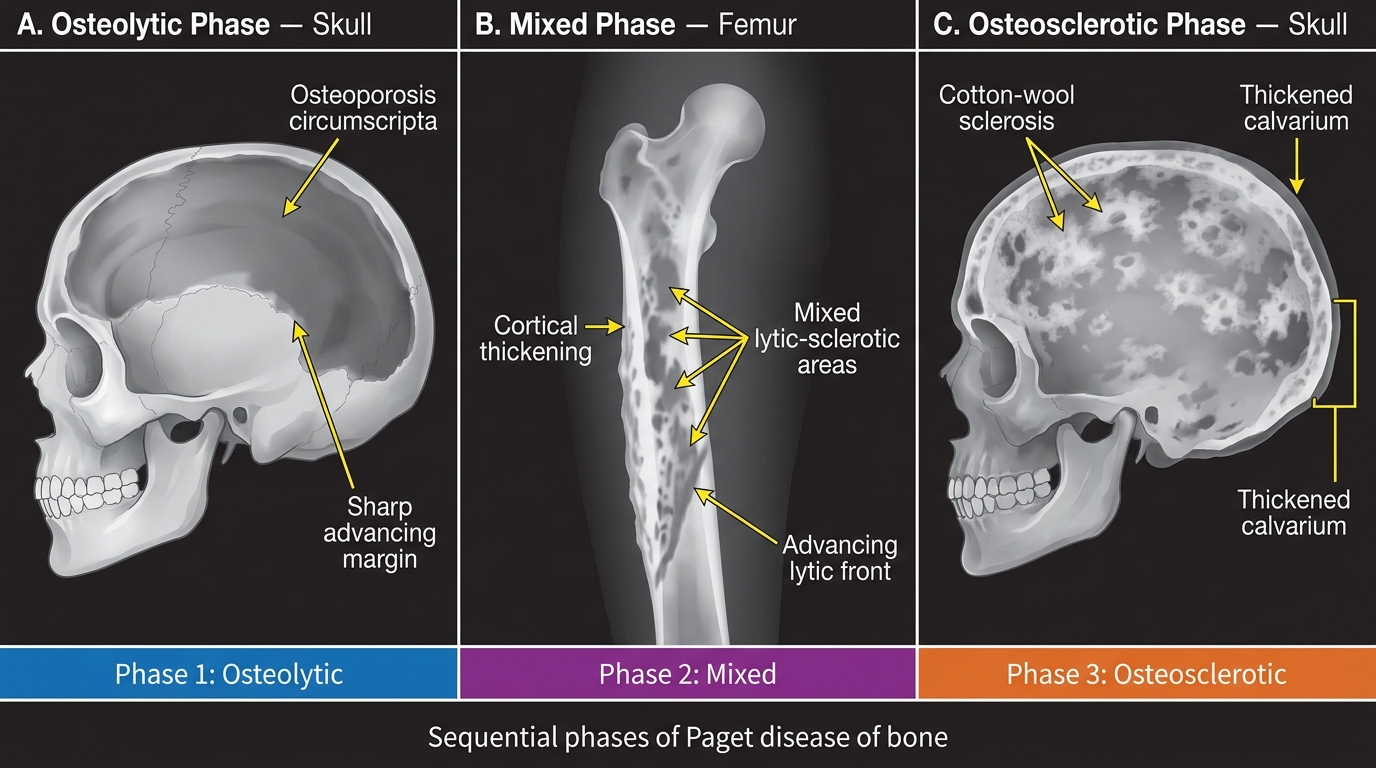
Paget Disease: Radiological Phases — Osteolytic, Mixed, and Osteosclerotic
Paget Disease: Pathognomonic Microscopic Feature — The Mosaic Pattern
The mosaic (jigsaw) cement-line pattern is the pathognomonic microscopic feature of Paget disease and an absolute must-know for histopathology practical examinations.
What you see:
• Bone trabeculae are composed of multiple irregular fragments of lamellar bone pieced together like a jigsaw puzzle
• The fragments are separated by prominent, irregular, basophilic cement lines (also called reversal lines or resting lines)
• These cement lines are the mineralised remnants of the original resorption lacunae — they demarcate where one phase of resorption ended and new bone was deposited
• The result is a characteristic "mosaic" or "crazy paving" pattern
Why does this happen?
Normal bone remodeling couples resorption and formation in organised packets — cement lines are present but sparse and regular. In Paget disease, the chaotic, asynchronous cycling of hyperactive osteoclasts and osteoblasts creates countless resorption-deposition cycles → cement lines accumulate densely and irregularly.
Other histological features:
• Pagetic osteoclasts — giant, hypernucleated (up to 100 nuclei), with viral inclusion-like bodies
• Woven bone in early phases; mosaic lamellar bone in later phases
• Hypervascular fibrous stroma in active phases (explains the hyperemia and AV shunting)
• In late phase: relative acellularity, mosaic pattern predominates
The ALP connection: Serum ALP is the osteoblast enzyme — it rises proportionally to osteoblast activity. In Paget disease, ALP can be 10–20× normal (vs. 2–3× in other bone diseases). Urinary hydroxyproline reflects collagen breakdown (osteoclast activity). Together, these are the biochemical fingerprint.
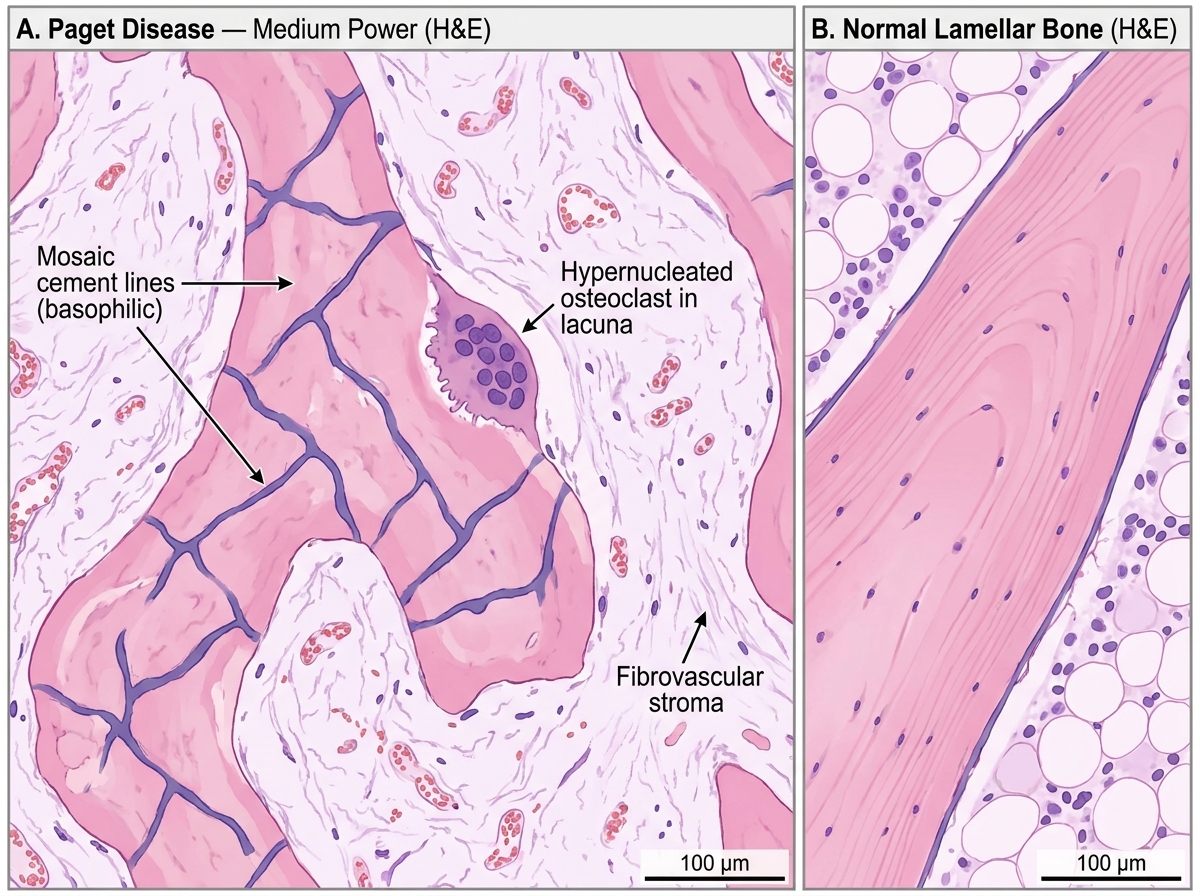
Histology of Paget Disease of Bone vs Normal Lamellar Bone (H&E, Medium Power)
SELF-CHECK
A 70-year-old man has a serum ALP of 480 U/L (normal < 120), normal calcium, normal phosphate, and no liver disease. Skull X-ray shows patchy sclerosis with a "cotton-wool" appearance. Bone biopsy is taken. Which histological pattern is PATHOGNOMONIC of his diagnosis?
A. Caseating granulomas with Langhans giant cells and central caseous necrosis
B. Irregular lamellar bone with multiple prominent basophilic cement lines creating a mosaic (jigsaw) pattern
C. Woven bone with osteosarcomatous spindle cells and abnormal mitoses
D. Parallel lamellar bone trabeculae with empty lacunae and absent osteocytes
Reveal Answer
Answer: B. Irregular lamellar bone with multiple prominent basophilic cement lines creating a mosaic (jigsaw) pattern
The mosaic/jigsaw cement-line pattern is pathognomonic of Paget disease of bone (osteitis deformans). The markedly elevated ALP (osteoblast hyperactivity), normal calcium and phosphate (unlike hyperparathyroidism), cotton-wool skull X-ray, and older male all fit perfectly. Option A describes TB (caseating granulomas). Option C describes osteosarcoma — a complication that can arise in Paget disease, but the biopsy at this stage does not show malignant features. Option D describes dead bone (a sequestrum in osteomyelitis — empty lacunae = absent osteocytes).