Page 4 of 20
PA32.{1,4} | Osteomyelitis & Paget Disease of Bone — SDL Guide (Part 4)
Paget Disease: Manifestations, Radiological Features & Complications
Clinical manifestations (often asymptomatic — incidental finding):
• Bone pain — dull aching in the affected bone, worse at rest and at night
• Bone deformity — bowing of the femur and tibia ("sabre tibia" — anterior bowing); skull enlargement (hat size increases); frontal bossing
• Warmth over bone — due to hypervascularity of active Pagetic bone
Radiological features by site:
• Skull: Cotton-wool sclerosis (mixed phase); osteoporosis circumscripta (lytic phase); basilar invagination
• Spine: Ivory vertebra (uniformly dense); vertebral expansion ("picture frame" vertebra — thickened cortex outline)
• Femur/Tibia: Cortical thickening, bowing, blade-of-grass lytic front progressing distally
• Pelvis: Thickened iliopectineal line ("pelvic brim" sign)
Complications (HIGH YIELD — know all five):
- Pathological fracture — "chalk-stick fracture": transverse fracture (unlike spiral fractures in normal bone) because Pagetic bone is brittle despite being sclerotic; common in femur
- Nerve compression — skull base thickening → cranial nerve palsies; most importantly VIII nerve compression → sensorineural deafness (common viva answer); also cranial nerve VII, visual disturbances
- High-output cardiac failure — Pagetic bone is extremely hypervascular, acting as a vast arteriovenous shunt; increased cardiac output over years → high-output cardiac failure; this is the systemic cardiovascular complication (not a primary cardiac disease)
4. Osteosarcoma transformation (~1% of polyostotic Paget disease)
• Most feared complication
• "Secondary osteosarcoma" arising in previously Pagetic bone
• Occurs in elderly patients (7th–8th decade)
• Very aggressive — worse prognosis than primary osteosarcoma
• Presents as: sudden increase in bone pain; rapid soft tissue swelling; new lytic-destructive lesion superimposed on Pagetic bone
• ALP rises sharply
- Basilar invagination / Platybasia — upward migration of upper cervical spine into skull base → compression of brainstem and cerebellum
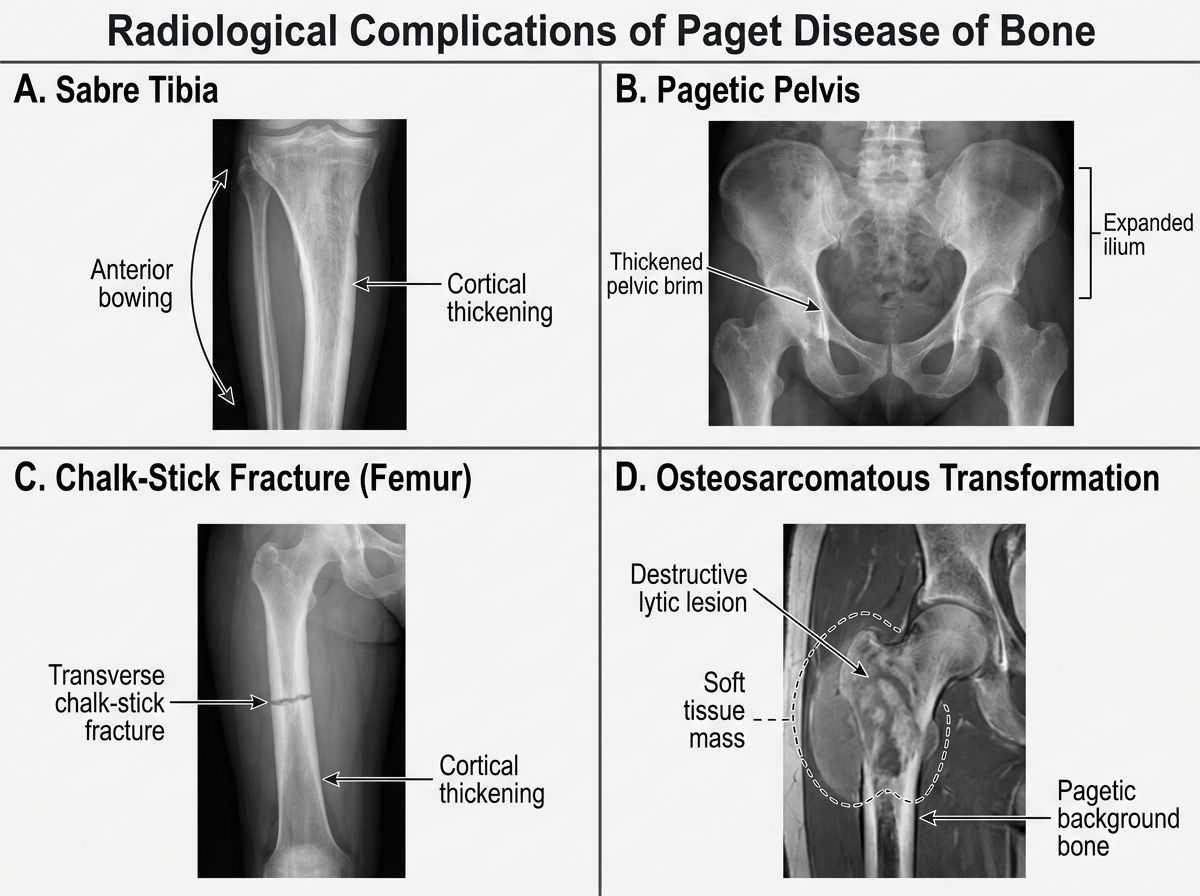
Radiological Complications of Paget Disease of Bone
CLINICAL PEARL
High-output cardiac failure in Paget disease — the pathophysiology in one sentence:
Pagetic bone is riddled with arteriovenous shunts through its hypervascular fibrous stroma. Blood is essentially short-circuited from arteries to veins within the bone without delivering oxygen to tissue. The heart must pump extra blood to compensate — over years, this sustained high cardiac output causes ventricular dilation and eventually biventricular failure.
How to remember this for the exam: "Paget's bone acts like a big AV fistula" — the same mechanism as a large arteriovenous malformation causing heart failure.
Practical point: a patient with Paget disease, a bounding pulse, high pulse pressure, and warm extremities likely has high-output failure — do NOT confuse it with the usual low-output (cold, clammy) cardiac failure picture.
SELF-CHECK
A 75-year-old woman with known polyostotic Paget disease (on bisphosphonate therapy for 4 years) presents with sudden worsening of right femur pain and a new soft tissue mass. X-ray shows a destructive lytic lesion superimposed on the previously sclerotic Pagetic bone. ALP has doubled since her last visit. What is the most likely complication?
A. Chalk-stick pathological fracture through Pagetic bone
B. Bisphosphonate-related osteonecrosis of the jaw
C. Secondary osteosarcoma transformation in Pagetic bone
D. High-output cardiac failure from increased AV shunting
Reveal Answer
Answer: C. Secondary osteosarcoma transformation in Pagetic bone
Secondary osteosarcoma arising in Pagetic bone is the most feared complication of Paget disease, occurring in approximately 1% of polyostotic cases. The red flags here are: (1) sudden increase in bone pain in previously stable disease, (2) new soft tissue mass, (3) new destructive lytic lesion superimposed on sclerotic Pagetic bone, and (4) sharply rising ALP. This is highly aggressive and has a poor prognosis. Chalk-stick fracture (option A) is transverse and would not produce a soft tissue mass or rising ALP. Bisphosphonate osteonecrosis (option B) affects the jaw. High-output cardiac failure (option D) does not produce a focal bone lesion.