Page 4 of 34
PA26.1-2 | Atherosclerosis & Aneurysms — SDL Guide (Part 4)
Berry Aneurysms and Other Aneurysm Types
Berry, Hypertensive, and Mycotic Aneurysms
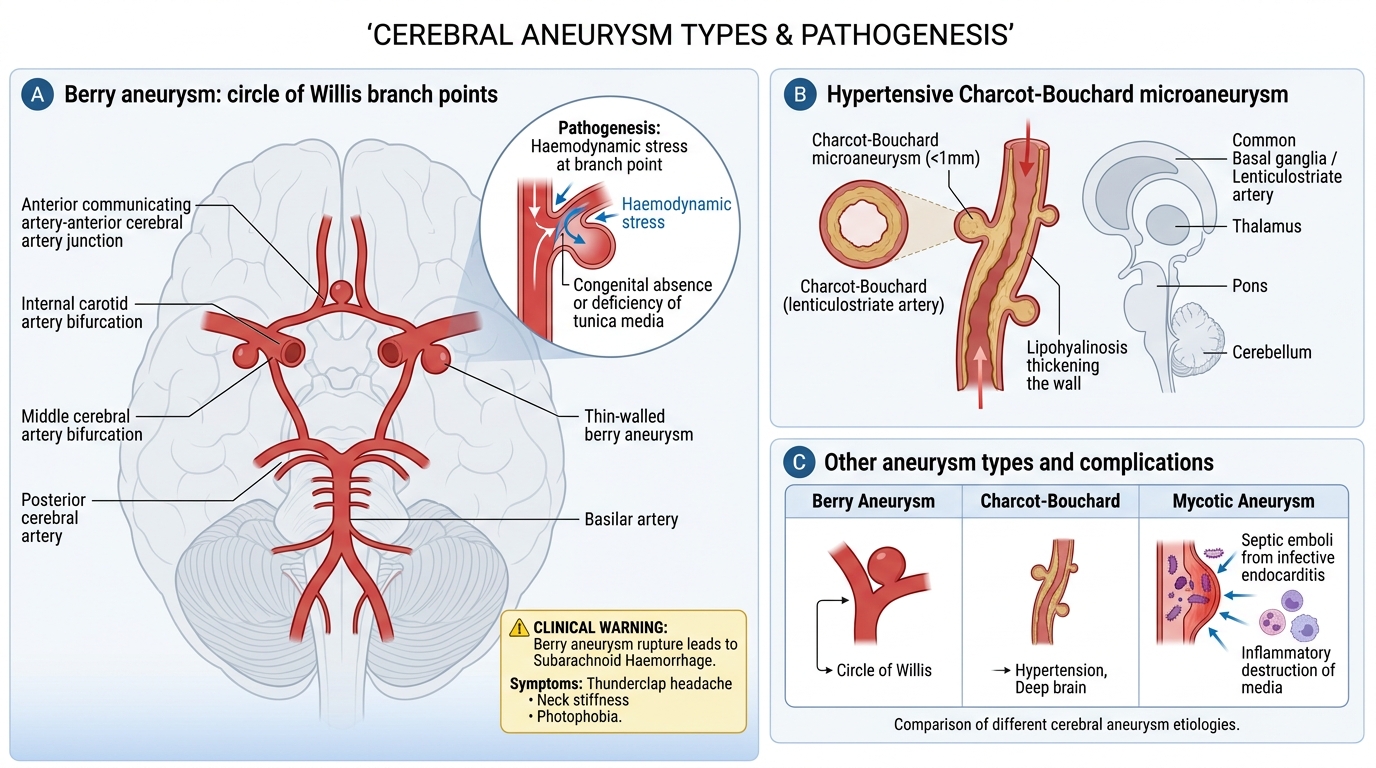
Berry (saccular cerebral) aneurysm:
• Small, rounded outpouchings at branch points of the circle of Willis (most common: junction of anterior communicating artery with anterior cerebral artery, internal carotid artery bifurcation, middle cerebral artery bifurcation)
• Pathogenesis: congenital absence/deficiency of the tunica media at arterial branch points + haemodynamic stress at bifurcations. Not atherosclerotic. Associated with: ADPKD (autosomal dominant polycystic kidney disease), connective tissue disorders, coarctation of aorta.
• Morphology: thin-walled saccular protrusion, 0.5–3 cm; contains no normal media
• Complication: subarachnoid haemorrhage (SAH) — sudden 'thunderclap' worst headache of life, neck stiffness, photophobia → high mortality and morbidity
Hypertensive (Charcot-Bouchard) microaneurysms:
• Tiny aneurysms (<1 mm) in small perforating arteries of the brain (lenticulostriate, thalamostriate, pons, cerebellum)
• Cause: chronic hypertension → lipohyalinosis of vessel wall → small outpouchings
• Consequence: hypertensive intracerebral haemorrhage (most common cause of ICH)
Mycotic aneurysms:
• Caused by septic emboli (infective endocarditis, bacteraemia) lodging in vasa vasorum or directly infecting the arterial wall → focal inflammatory destruction of the media
• Can affect any artery; often multiple
Summary table — aneurysm types:
| Type | Location | Aetiology | Shape | Complication |
|---|---|---|---|---|
| Atherosclerotic | Infrarenal aorta | Atherosclerosis, male>65 | Fusiform | Rupture, embolism |
| Dissecting | Ascending aorta | Cystic medial degen, HTN, Marfan | — | Tamponade, AR, stroke |
| Syphilitic | Thoracic aorta | Vasa vasorum endarteritis | Saccular | AR, coronary ostial stenosis |
| Berry | Circle of Willis | Congenital media defect | Saccular | SAH |
| Charcot-Bouchard | Brain perforators | Hypertension | Micro | ICH |
| Mycotic | Any | Septic embolus | Variable | Rupture, sepsis |
SELF-CHECK
A 38-year-old tall, thin man with arachnodactyly and lens dislocation is found on echocardiography to have a dilated aortic root (4.8 cm). Which underlying pathological process in the aortic wall BEST explains his risk for aortic dissection?
A. Atherosclerotic plaque causing medial ischaemia via vasa vasorum compression
B. Endarteritis obliterans of the vasa vasorum secondary to chronic infection
C. Cystic medial degeneration with loss of smooth muscle cells and elastic fibre fragmentation
D. Hyaline arteriolosclerosis of the aortic wall secondary to hypertension
Reveal Answer
Answer: C. Cystic medial degeneration with loss of smooth muscle cells and elastic fibre fragmentation
Marfan syndrome (FBN1 mutation → defective fibrillin-1) causes cystic medial degeneration (necrosis) — the hallmark histological lesion of the aortic media in Marfan patients. This manifests as loss of medial smooth muscle cells, fragmentation and loss of elastic fibres, and replacement by myxoid/mucoid ground substance. The weakened media cannot resist haemodynamic forces → progressive aortic root dilation → Type A dissection risk. Option A describes atherosclerotic AAA mechanism; option B is syphilitic aortitis; option D is arteriolosclerosis in hypertension (affects small vessels, not the aorta).