Page 3 of 34
PA26.1-2 | Atherosclerosis & Aneurysms — SDL Guide (Part 3)
Laplace's Law and Aneurysm Dynamics
Understanding why aneurysms enlarge progressively requires Laplace's Law:
> Wall tension (T) = Transmural pressure (P) × Radius (r) / Wall thickness (w)
In simplified form for a thin-walled cylinder: T ∝ P × r
Implications:
• Once an arterial segment begins to dilate, its radius increases → wall tension increases (for the same blood pressure).
• Increased tension causes further dilation → greater radius → even higher tension — a self-reinforcing progressive cycle.
• Simultaneously, the wall thins as it dilates (conservation of wall volume), further increasing tension (T = Pr/w).
• Rupture occurs when wall tension exceeds wall tensile strength.
Clinical application: This is why AAAs >5.5 cm diameter (or rapidly expanding) are referred for surgical repair — the risk of rupture rises exponentially with size. An AAA of 7 cm has ~20% annual rupture risk; one of 4 cm has ~1%.
The same principle explains why hypertension dramatically accelerates aneurysm growth (↑P → ↑T) and why BP control is critical in Marfan syndrome patients with dilated aortic roots.
Abdominal Aortic Aneurysm (AAA)
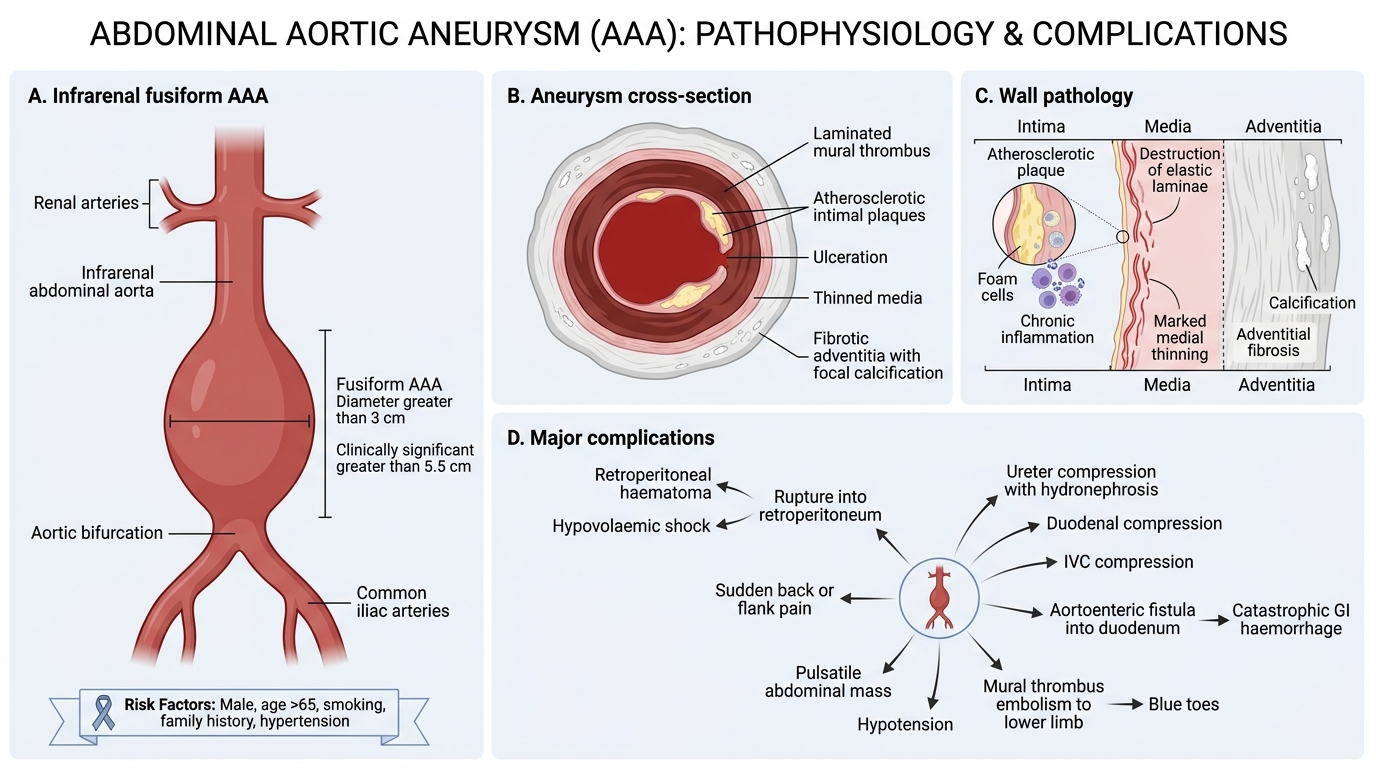
Abdominal Aortic Aneurysm: Anatomy, Pathology, and Complications
AAA is the prototype atherosclerotic aneurysm and the most common clinically significant aneurysm.
Key facts:
• Location: infrarenal abdominal aorta (below origin of renal arteries) in >90% of cases
• Shape: fusiform (most), occasionally saccular
• Size: >3 cm diameter by definition; clinically significant >5.5 cm
• Risk factors: male sex, age >65, smoking (strongest modifiable risk factor), family history, hypertension
Pathology:
• Intimal surface: atherosclerotic plaques, ulceration, mural thrombus layered concentrically ('onion-ring' thrombus)
• Media: marked thinning, destruction of elastic laminae, chronic inflammation, foam cells
• Adventitia: adventitial fibrosis, occasional calcification
Complications:
• Rupture → retroperitoneal haematoma → hypovolaemic shock → death (mortality ~80% of untreated ruptures). The classic triad: sudden severe back/flank pain, pulsatile abdominal mass, hypotension.
• Thrombosis and embolism: mural thrombus fragments → atheroembolism to lower limbs (blue toes, calf claudication)
• Compression of adjacent structures: ureter (hydronephrosis), duodenum, inferior vena cava
• Aortoenteric fistula: eroded AAA → fistula into duodenum → catastrophic GI haemorrhage
• Aortoiliac occlusion from progressive expansion
Aortic Dissection (Dissecting Aneurysm)
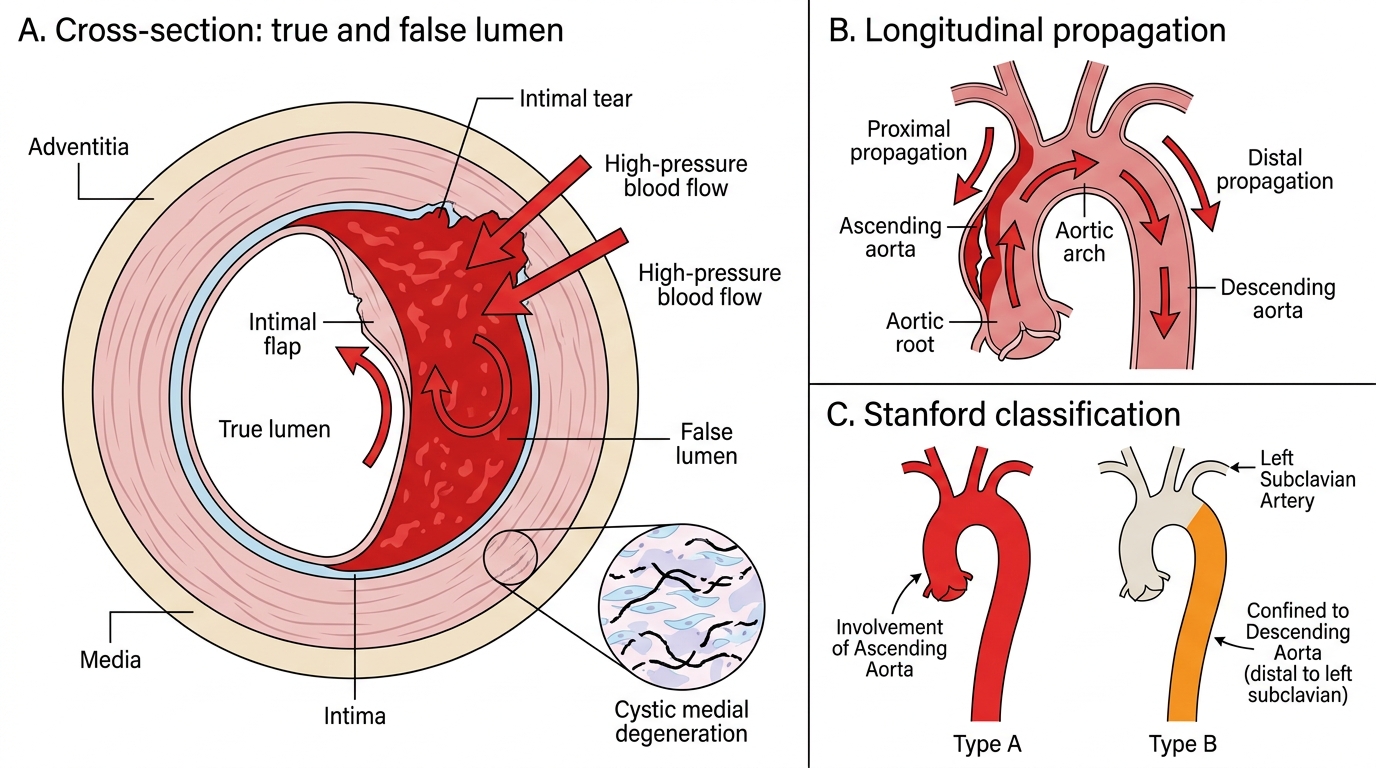
Aortic Dissection: False Lumen Formation and Stanford Classification
Aortic dissection is a catastrophic condition in which blood enters and tracks within the media, creating a false lumen — it is NOT primarily an aneurysm (though aortic root aneurysm predisposes to it).
Pathogenesis:
1. Underlying media disease: cystic medial degeneration (necrosis) — loss of smooth muscle cells, fragmentation of elastic fibres, replacement by myxoid (mucoid) material. Seen in: Marfan syndrome (FBN1 mutation → defective fibrillin-1 → TGF-β dysregulation → medial degeneration), Ehlers-Danlos syndrome, longstanding hypertension.
2. A transverse intimal tear (usually ascending aorta) allows blood under high arterial pressure to enter the degenerated media.
3. Blood dissects longitudinally through the media, creating a blood-filled cleavage plane — the false lumen — that can propagate proximally and/or distally.
Stanford Classification (surgical and prognostic):
• Type A — involves ascending aorta (±arch, ±descending); surgical emergency; highest mortality
• Type B — confined to descending aorta (distal to left subclavian); managed medically (BP control) unless complications arise
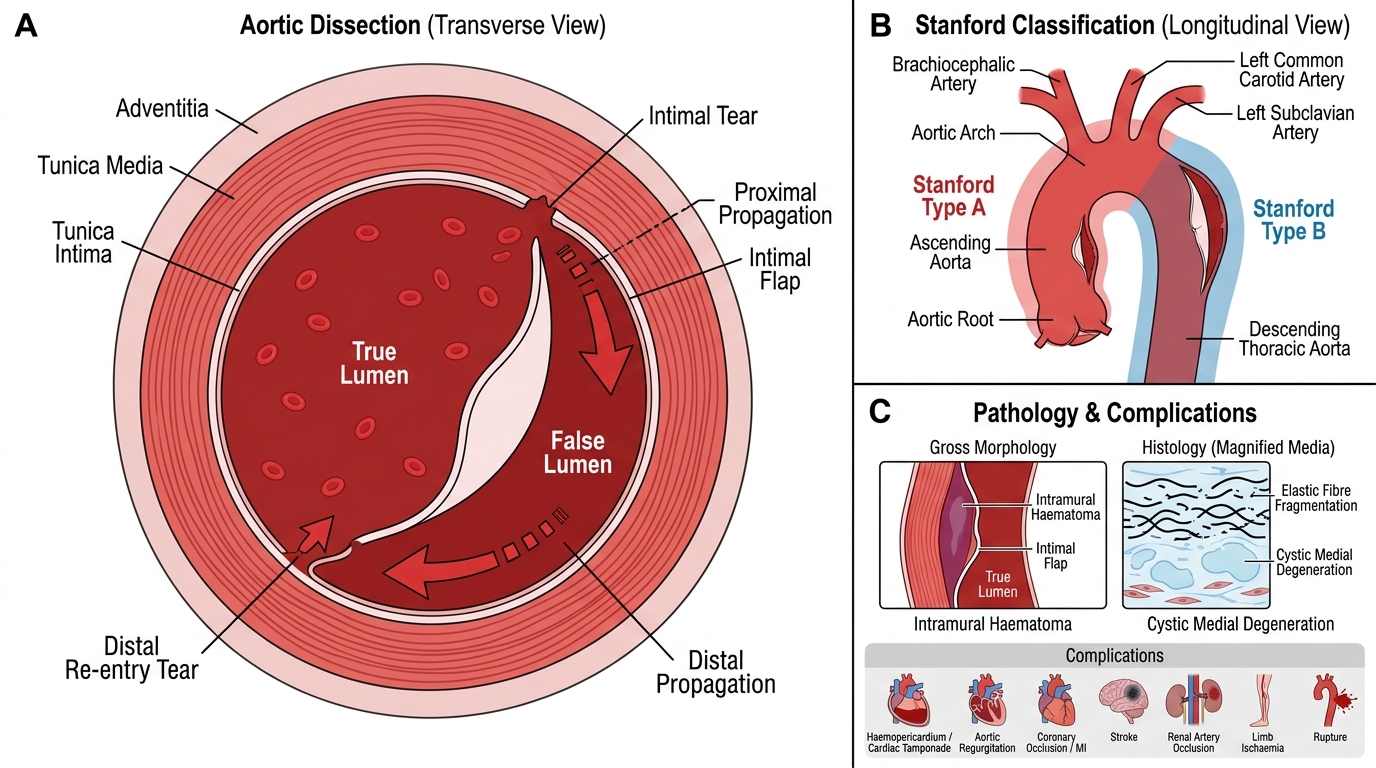
Aortic Dissection: Morphology and Stanford Classification
Morphology:
• Gross: longitudinal haematoma in the media; the intimal flap separates true lumen from false lumen; two openings (proximal tear, ± distal re-entry tear)
• Histology: elastic fibre fragmentation, myxoid change in media (cystic medial degeneration)
Complications:
• Cardiac tamponade (Type A: haemopericardium)
• Aortic regurgitation (dissection disrupts aortic root/valve annulus)
• Coronary artery occlusion → acute MI
• Stroke (carotid/vertebral occlusion)
• Renal failure (renal artery occlusion)
• Limb ischaemia (iliac artery occlusion)
• Rupture into mediastinum/pleural cavity → fatal haemorrhage
Key clinical sign: Pulse/BP differential between upper limbs (subclavian involvement) — as in our opening case.
CLINICAL PEARL
Syphilitic (luetic) aortitis — a reminder that tertiary syphilis (10-30 years after infection) causes an endarteritis obliterans of the vasa vasorum of the thoracic aorta. Loss of vasa vasorum → ischaemic necrosis of the media → weakened aortic wall → aneurysm. Location: ascending aorta and arch (unlike atherosclerotic AAA which is infrarenal). Complications: 'tree-bark' intimal wrinkling, aortic root dilation → aortic regurgitation ('tambour' heart sound), coronary ostial narrowing → angina. The Argyll Robertson pupil + aortic regurgitation murmur + widened mediastinum = classic viva presentation of tertiary cardiovascular syphilis.