Page 2 of 34
PA26.1-2 | Atherosclerosis & Aneurysms — SDL Guide (Part 2)
The Atheromatous Plaque: Morphology
Mature Atheromatous Plaque: Morphology and Clinical Significance
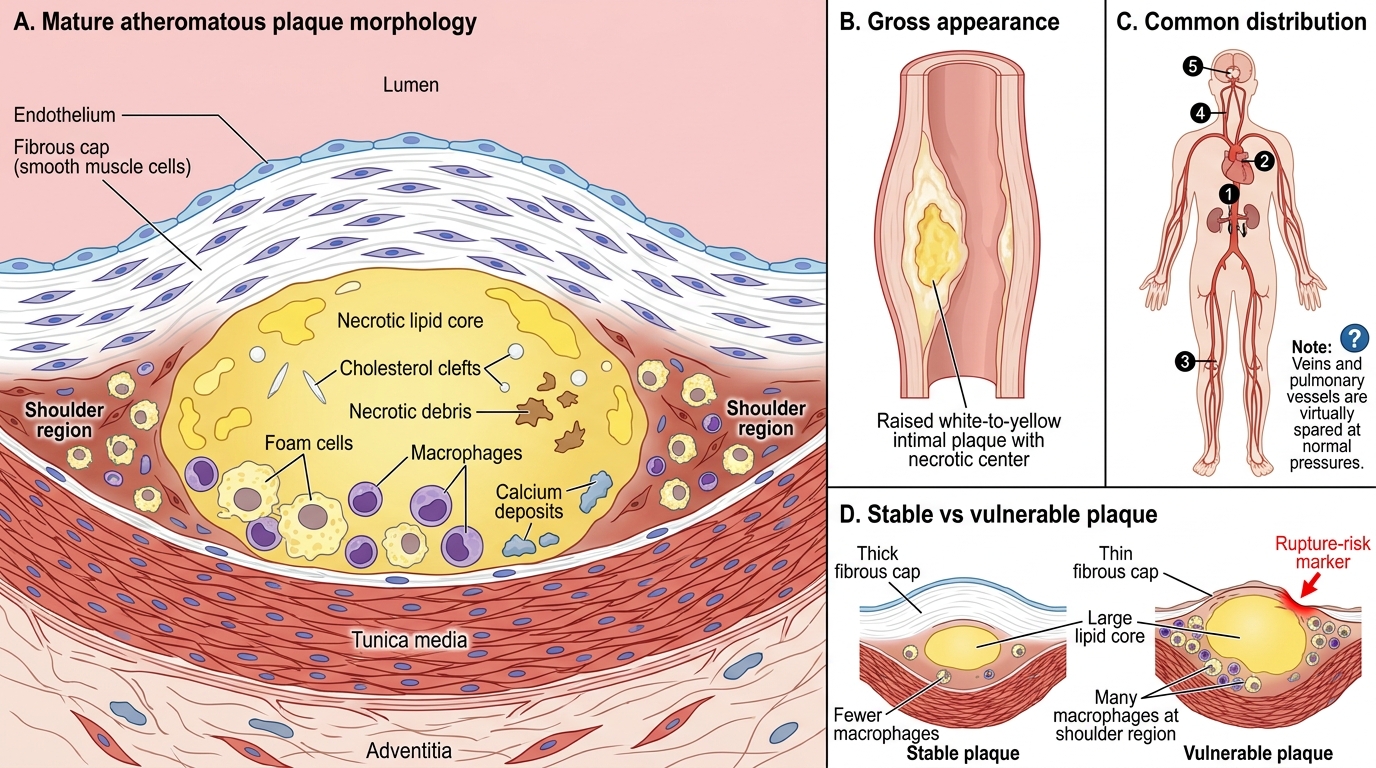
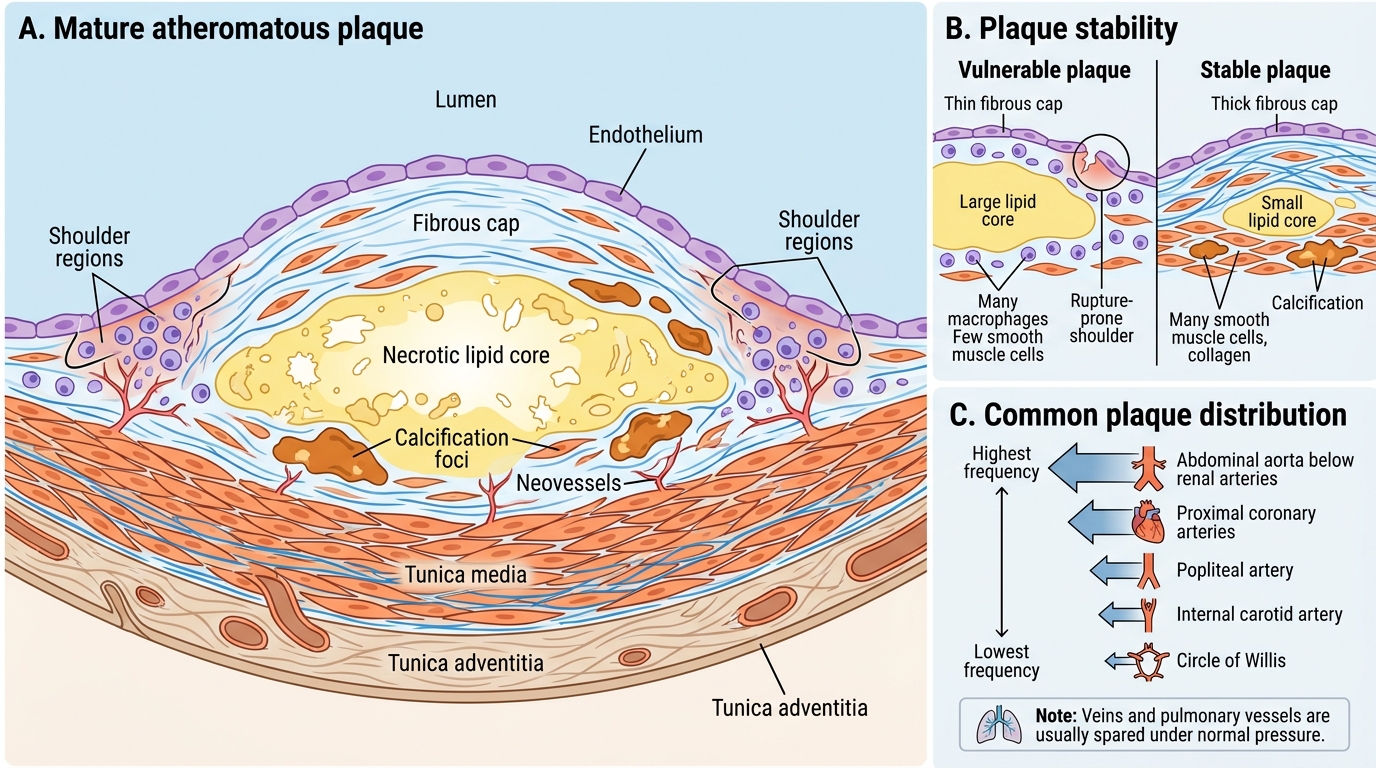
The mature atheromatous plaque (fibrous plaque, atheroma) is the signature lesion of atherosclerosis:
Gross appearance: white-to-yellow, raised intimal lesion; size from a few mm to several cm; may have yellowish, porridge-like necrotic centre ('atheroma' = Greek for gruel).
Microscopic components:
• Fibrous cap — superficial layer composed of SMCs, macrophages, foam cells, lymphocytes embedded in a dense collagen and proteoglycan matrix. Provides structural integrity.
• Necrotic lipid core — central acellular zone of cholesterol crystals, necrotic debris, foam cell remnants, calcium deposits.
• Shoulder region — lateral edges where active inflammation predominates; most vulnerable to rupture.
Mature Atheromatous Plaque: Structure, Stability, and Distribution
Distribution of plaques (highest to lowest frequency):
1. Abdominal aorta (below renal arteries) — most heavily affected
2. Coronary arteries (proximal segments)
3. Popliteal artery (claudication in peripheral arterial disease)
4. Internal carotid artery (stroke)
5. Circle of Willis
Note: Veins and pulmonary vessels are virtually never affected under normal (non-elevated) pressures — reinforcing the haemodynamic/pressure component of injury.
Plaque stability: A plaque with a thin fibrous cap + large lipid core + many macrophages/few SMCs is vulnerable (high rupture risk) even if it causes <50% stenosis. A thick cap + small core + heavy calcification is stable (less rupture risk, more stenosis).
CLINICAL PEARL
Thin-cap fibroatheroma (TCFA) is the pathological definition of the 'vulnerable plaque' responsible for most acute MI events. Paradoxically, many MI patients had <50% stenosis on their last angiogram — the plaque ruptured before it caused significant obstruction. This is why statin therapy (plaque stabilisation, not just cholesterol-lowering) reduces MI events even in patients without high-grade stenosis. The clinical lesson: don't wait for flow-limiting disease to start secondary prevention.
SELF-CHECK
In the response-to-injury hypothesis, which receptor on macrophages is primarily responsible for ox-LDL uptake leading to foam cell formation?
A. LDL receptor (LDLR / ApoB-100 receptor)
B. Scavenger receptor (SR-A / CD36)
C. VLDL receptor
D. Toll-like receptor 4 (TLR-4)
Reveal Answer
Answer: B. Scavenger receptor (SR-A / CD36)
Scavenger receptors (SR-A, CD36) on macrophages have low affinity for native LDL but high affinity for ox-LDL. Critically, scavenger receptors are NOT downregulated by cholesterol accumulation (unlike the LDL receptor which is downregulated by cellular cholesterol via SREBP), so macrophages continue engulfing ox-LDL until they are massively lipid-laden — this is the molecular basis for uncontrolled foam cell formation. TLR-4 also binds ox-LDL and triggers inflammatory signalling but is not the primary uptake receptor.
Complications of Atherosclerosis
Complications of Atherosclerosis
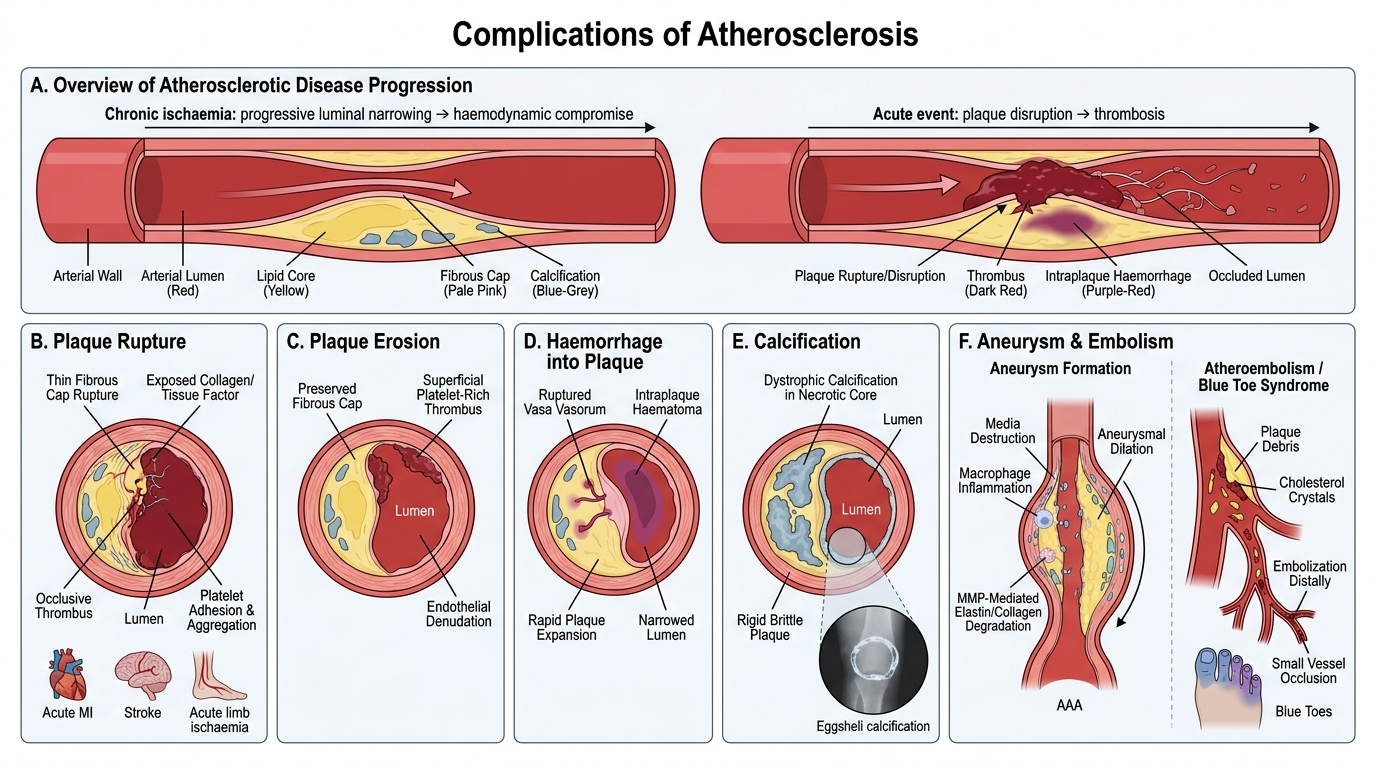
Atheromatous plaques cause disease through two broad mechanisms: chronic ischaemia (progressive luminal narrowing → haemodynamic compromise) and acute events (sudden plaque disruption → thrombosis).
1. Plaque rupture / erosion → thrombosis (most dangerous)
• Rupture: thin fibrous cap breaks (often at the shoulder); lipid core exposes collagen and tissue factor → platelet adhesion → thrombus.
• Result: acute MI (coronary), stroke (carotid), acute limb ischaemia (peripheral). Responsible for ~75% of fatal MIs.
• Plaque erosion (endothelial loss without frank rupture) causes remaining ~25%.
2. Haemorrhage into plaque
• Disruption of thin-walled vasa vasorum within the plaque → intraplaque haematoma → sudden plaque expansion → rapid luminal narrowing without rupture. Contributes to unstable angina and acute coronary syndromes.
3. Calcification
• Dystrophic calcification of the necrotic core → rigid, brittle plaque. May cause 'eggshell' calcification visible on X-ray. Paradoxically associated with stable lesions but complicates percutaneous interventions.
4. Aneurysm formation
• Atherosclerotic plaques in the aortic wall destroy the media → weakened wall → aneurysmal dilation. The mechanism: inflammation, proteases (MMPs) from macrophages degrade elastin and collagen. Most commonly: abdominal aortic aneurysm (AAA).
5. Atheroembolism
• Plaque rupture → release of cholesterol crystals / thrombotic debris → emboli to distal vessels → 'blue toe syndrome', renal infarcts, mesenteric ischaemia.
6. Progressive stenosis → chronic ischaemia
• Coronary: stable angina → chronic heart failure
• Renal: renovascular hypertension, ischaemic nephropathy
• Mesenteric: intestinal ischaemia / 'abdominal angina'
• Peripheral: intermittent claudication → rest pain → gangrene
SELF-CHECK
A 55-year-old man develops an acute MI. Coronary angiography performed 24 hours earlier showed only 45% stenosis at the culprit site. What pathological finding at the plaque BEST explains this acute event?
A. Heavy calcification of the fibrous cap causing embolisation
B. Rupture of a thin fibrous cap exposing the lipid core with thrombosis
C. Plaque with a thick fibrous cap and dense SMC content
D. Intraplaque haemorrhage from well-formed vasa vasorum
Reveal Answer
Answer: B. Rupture of a thin fibrous cap exposing the lipid core with thrombosis
Thin-cap fibroatheroma (TCFA) — the vulnerable plaque — typically causes <50% stenosis because most of its volume is occupied by a large lipid core with eccentric remodelling rather than lumen-encroachment. Rupture of the thin cap exposes the highly thrombogenic lipid core (collagen, tissue factor) to blood, triggering rapid platelet aggregation and thrombus formation that abruptly occludes the vessel. Option D (intraplaque haemorrhage) can also precipitate ACS but is the less common mechanism; option A and C describe stable lesions.
Aneurysms: Definition and Classification
Aneurysms: Definition and Classification
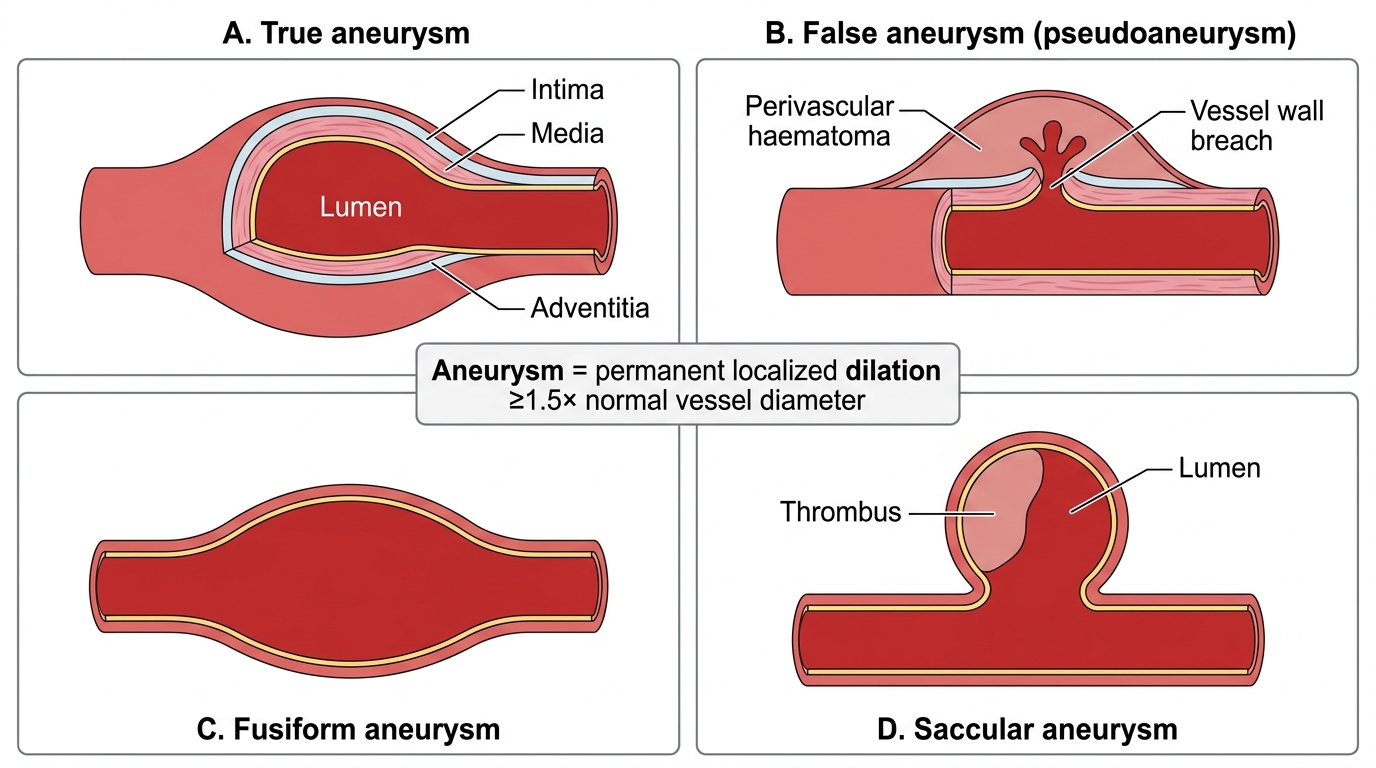
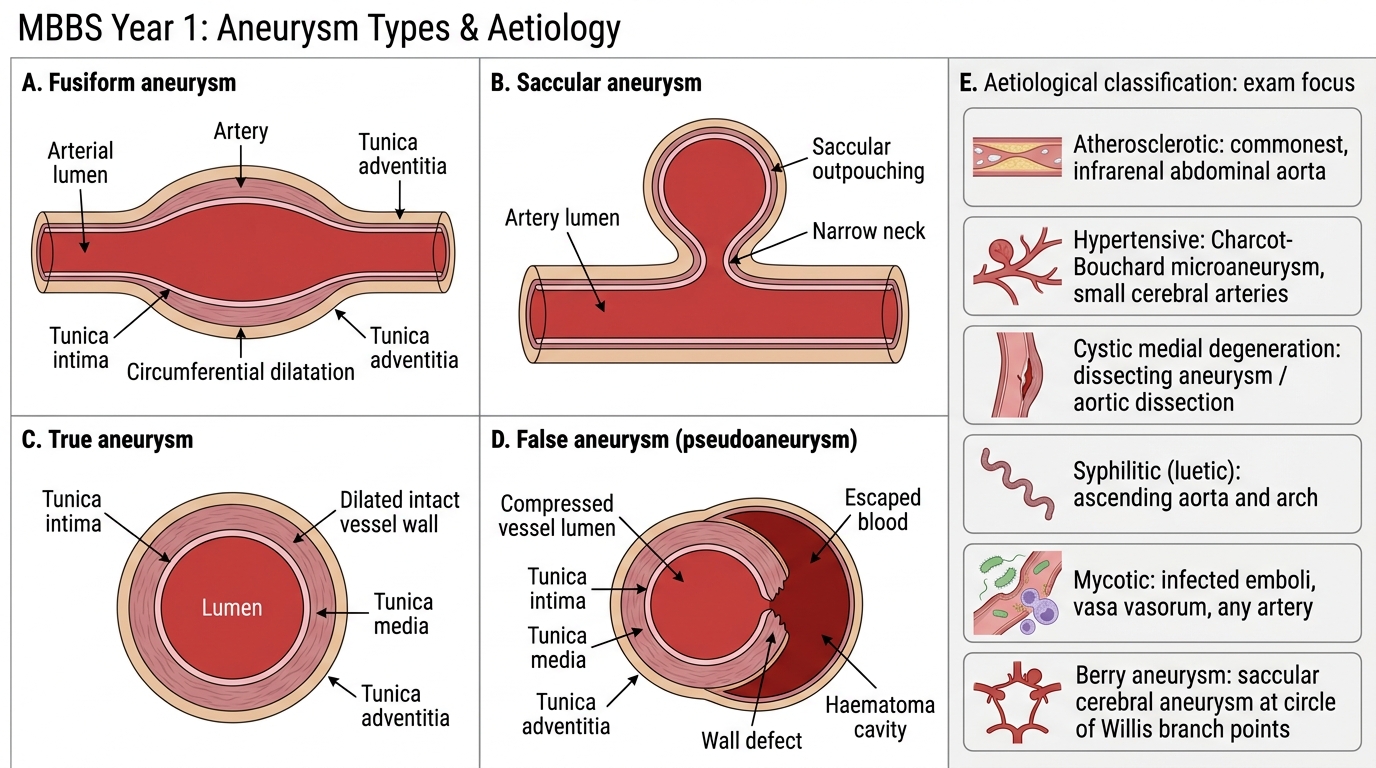
An aneurysm is a localised, abnormal, permanent dilation of a blood vessel (or cardiac chamber) to at least 1.5× its normal diameter.
True vs False aneurysm:
| Type | Wall | Example |
|---|---|---|
| True aneurysm | All three layers of the vessel wall (intima, media, adventitia) | Atherosclerotic AAA, syphilitic, berry |
| False aneurysm (pseudoaneurysm) | Haematoma contained by only adventitia and/or perivascular tissue — NOT a complete vessel wall | Post-catheterisation femoral artery, traumatic, anastomotic leak |
Morphological classification:
• Fusiform aneurysm — circumferential, symmetric dilation involving the full circumference of the vessel wall; spindle-shaped. Typical of atherosclerotic AAA.
• Saccular aneurysm — one-sided, spherical outpouching involving only part of the circumference. Typical of berry aneurysms at the circle of Willis and syphilitic aortitis.
Aneurysm Morphology and Anatomy
Aetiological classification (MOST IMPORTANT for exam):
1. Atherosclerotic — commonest overall; abdominal aorta below renal arteries (AAA)
2. Hypertensive — small cerebral arteries (Charcot-Bouchard microaneurysms) → intracerebral haemorrhage
3. Cystic medial degeneration → dissecting aneurysm / aortic dissection (Marfan syndrome, HTN)
4. Syphilitic (luetic) — tertiary syphilis; thoracic aorta (ascending + arch)
5. Mycotic — infected emboli lodge in vasa vasorum → septic weakening; any artery
6. Berry (saccular cerebral) — congenital defect in media at circle of Willis branch points