Page 20 of 34
PA26.{4,9} | Congenital Heart Disease & Cardiomyopathies — SDL Guide
Learning Objectives
- Classify congenital heart defects as left-to-right shunts, right-to-left shunts, or obstructive lesions and explain the haemodynamic consequences of each
- Describe the pathology, pathophysiology, and complications of VSD, ASD, PDA, and Tetralogy of Fallot
- Explain Eisenmenger syndrome — its mechanism, significance, and clinical consequences
- Classify cardiomyopathies (dilated, hypertrophic, restrictive) and describe the gross morphology, microscopy, and distinguishing features of each
- Identify the causes, pathophysiology, and major complications of hypertrophic obstructive cardiomyopathy (HOCM)
- Recognise the Indian-relevant pattern of restrictive cardiomyopathy (endomyocardial fibrosis)
INSTRUCTIONS
Cardiovascular malformations and cardiomyopathies together account for a significant proportion of cardiac morbidity and mortality across all age groups — from the cyanosed neonate to the young athlete who collapses on the field. Understanding the haemodynamic logic of congenital shunts and the pathological basis of muscle-disease cardiomyopathies builds the foundation for clinical cardiology and surgical decision-making. This module integrates morphology, physiology, and clinical consequences to give you a working framework.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 12 (Heart) (textbook)
- Harsh Mohan Textbook of Pathology, 7th ed., Ch 15 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 6-year-old boy is brought to the OPD because he squats down after running a few steps in the playground. His lips and fingernails turn blue during these episodes. His mother says he was 'always a bit blue' since birth and was told there is 'something wrong with the heart'. On examination: clubbing of fingers, loud systolic murmur, and a boot-shaped heart on chest X-ray. What is going on — and why does squatting help? By the end of this module you will answer this precisely.
WHY THIS MATTERS
Congenital heart defects occur in approximately 8 per 1,000 live births — they are the commonest group of serious congenital malformations. VSD alone accounts for nearly 30% of all congenital heart disease. Cardiomyopathies are the leading indication for cardiac transplantation worldwide. As a clinician you will encounter these conditions in paediatric wards, adult medicine, obstetric clinics (peripartum cardiomyopathy), and forensic post-mortems (sudden death in HOCM). NMC competency PA26.4 + PA26.9 ensure you can recognise, classify, and explain the pathological basis of each.
RECALL
Before proceeding, recall these Year-1 concepts:
- Pulmonary vascular resistance (PVR) is high at birth and falls over the first weeks of life — this is why some shunts are not immediately apparent.
- Blood flows from high pressure to low pressure. The systemic circulation is normally higher pressure than the pulmonary circulation.
- The fetal circulation has two right-to-left shunts: the foramen ovale (atrial level) and the ductus arteriosus (great vessel level) — both normally close after birth.
- Volume overload leads to dilatation; pressure overload leads to hypertrophy.
- Cyanosis (central blue discolouration) appears when deoxygenated haemoglobin exceeds 5 g/dL in arterial blood.
Aetiology of Congenital Heart Disease
Aetiology of Congenital Heart Disease
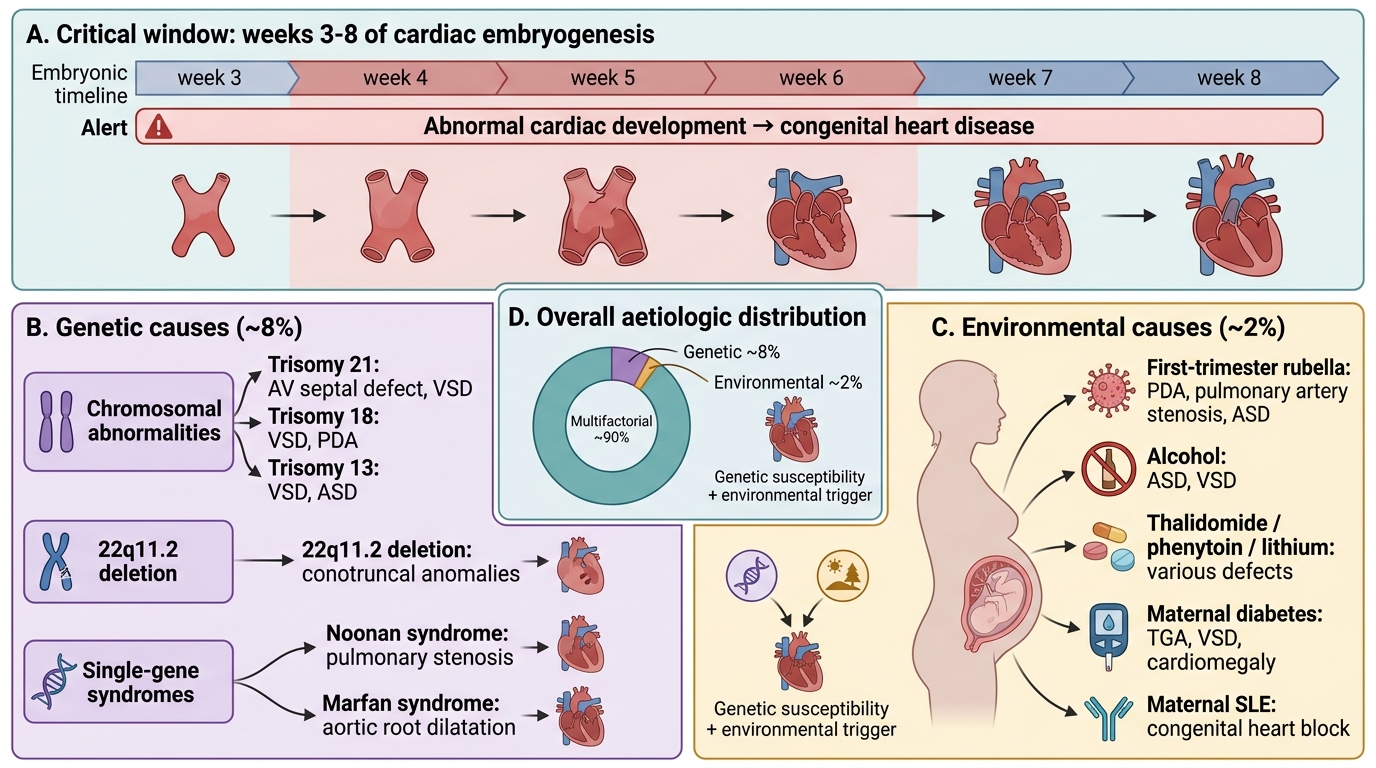
Congenital heart disease (CHD) results from abnormal cardiac development during weeks 3–8 of embryogenesis. Aetiology is predominantly multifactorial (genetic susceptibility + environmental trigger).
Genetic causes (~8%):
• Chromosomal — Trisomy 21 (Down syndrome): AV septal defect, VSD; Trisomy 18 (Edwards): VSD, PDA; Trisomy 13 (Patau): VSD, ASD
• 22q11.2 deletion (DiGeorge/velocardiofacial syndrome): conotruncal anomalies — truncus arteriosus, tetralogy of Fallot, interrupted aortic arch
• Single-gene mutations: Noonan syndrome (pulmonary stenosis), Marfan syndrome (aortic root dilatation)
Environmental causes (~2%):
• Rubella in first trimester — PDA, pulmonary artery stenosis, ASD (classic triad)
• Alcohol — fetal alcohol syndrome: ASD, VSD
• Thalidomide, phenytoin, lithium — various defects
• Maternal diabetes — transposition of great arteries, VSD, cardiomegaly
• Maternal systemic lupus erythematosus — congenital heart block
The remaining ~90% are multifactorial — a genetic substrate interacting with unidentified environmental factors.
Classification of Congenital Heart Disease
Haemodynamic Classification of Congenital Heart Disease
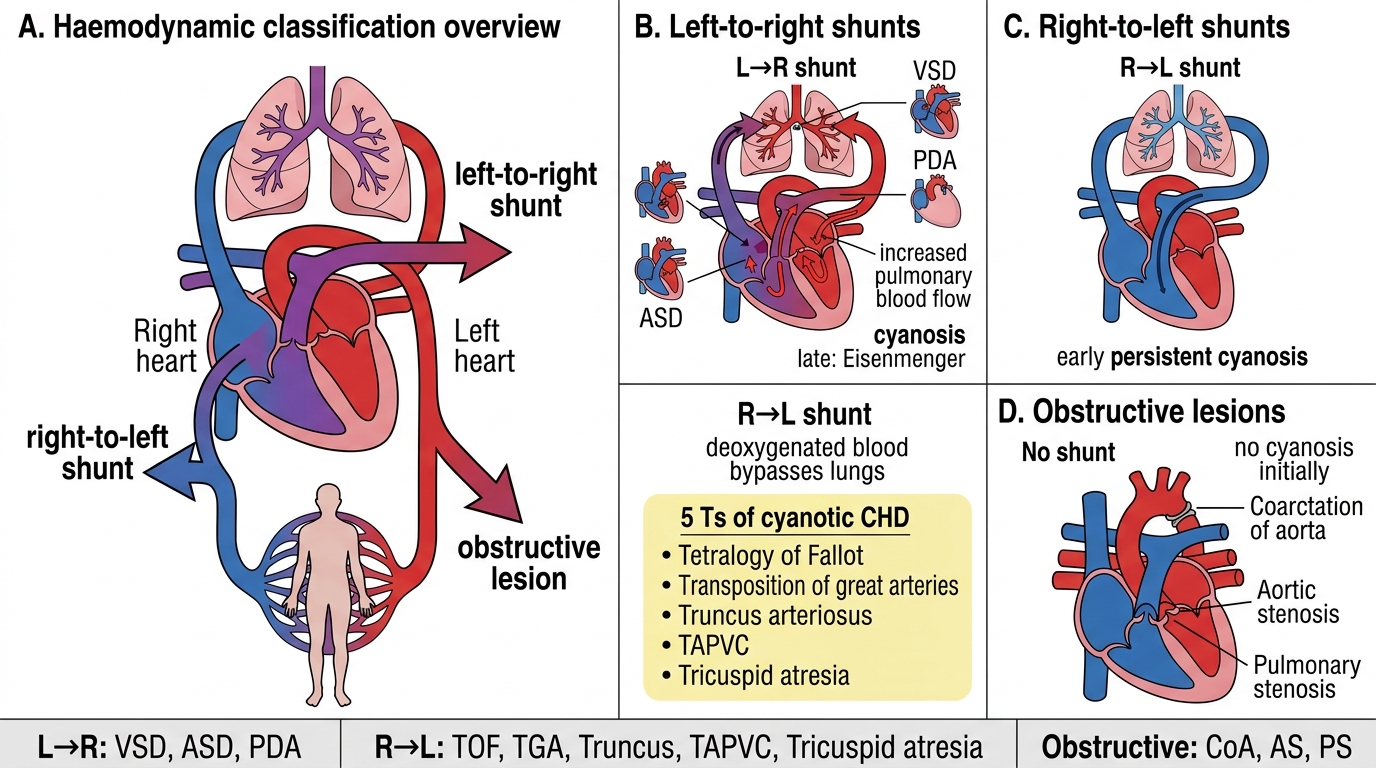
CHD is classified haemodynamically into three groups:
| Category | Direction | Cyanosis | Examples |
|---|---|---|---|
| Left-to-right shunts | L→R initially | Late (Eisenmenger) | VSD, ASD, PDA |
| Right-to-left shunts | R→L | Early, persistent | Tetralogy of Fallot, TGA, Truncus, TAPVC, Tricuspid atresia |
| Obstructive lesions | No shunt | None initially | Coarctation of aorta, aortic stenosis, pulmonary stenosis |
The 5 Ts of cyanotic CHD: Tetralogy of Fallot, Transposition of great arteries, Truncus arteriosus, Total anomalous pulmonary venous connection (TAPVC), Tricuspid atresia.
Key logic: in L→R shunts, oxygenated blood recirculates through the lungs → increased pulmonary blood flow → initially no cyanosis. In R→L shunts, deoxygenated blood bypasses the lungs → systemic cyanosis from birth.
Left-to-Right versus Right-to-Left Cardiac Shunts
Left-to-Right Shunts — VSD, ASD, PDA
Left-to-Right Shunts: VSD, ASD, and PDA
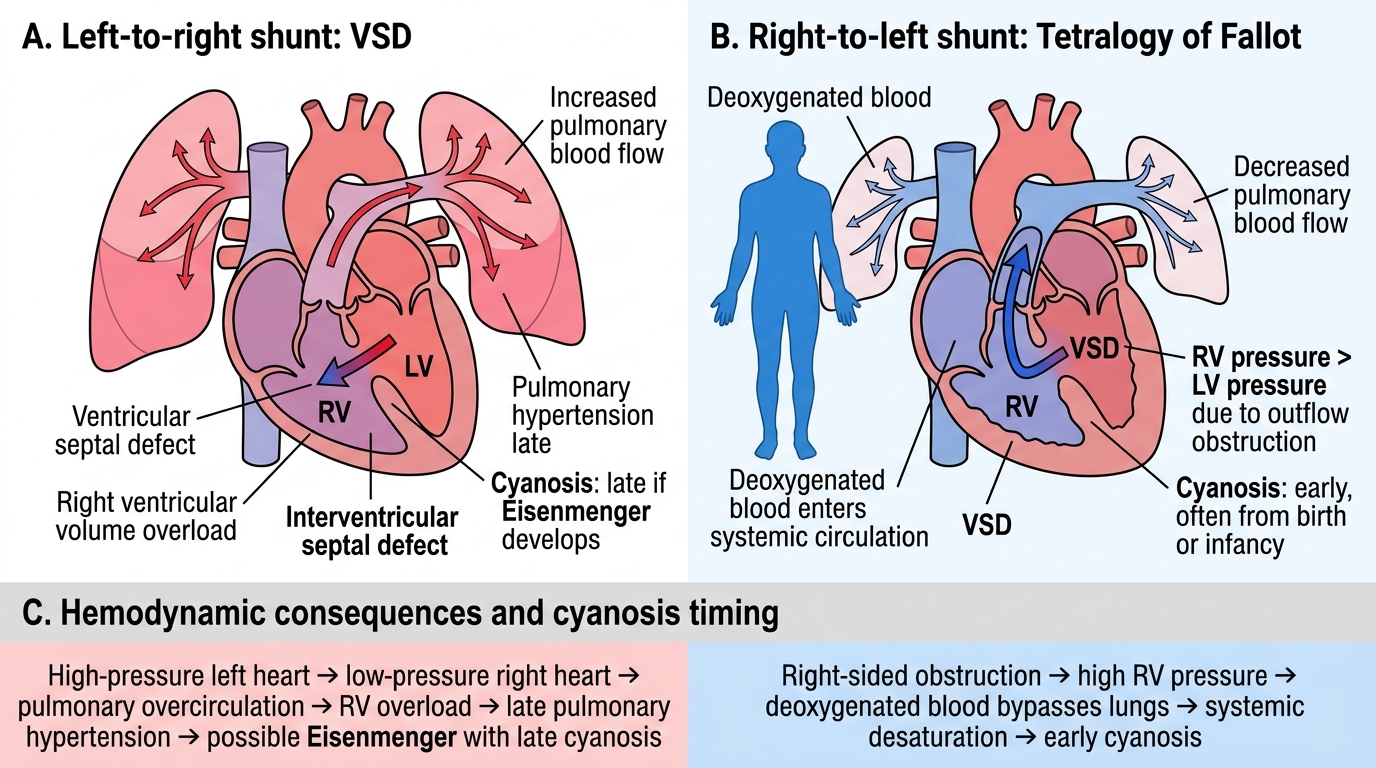
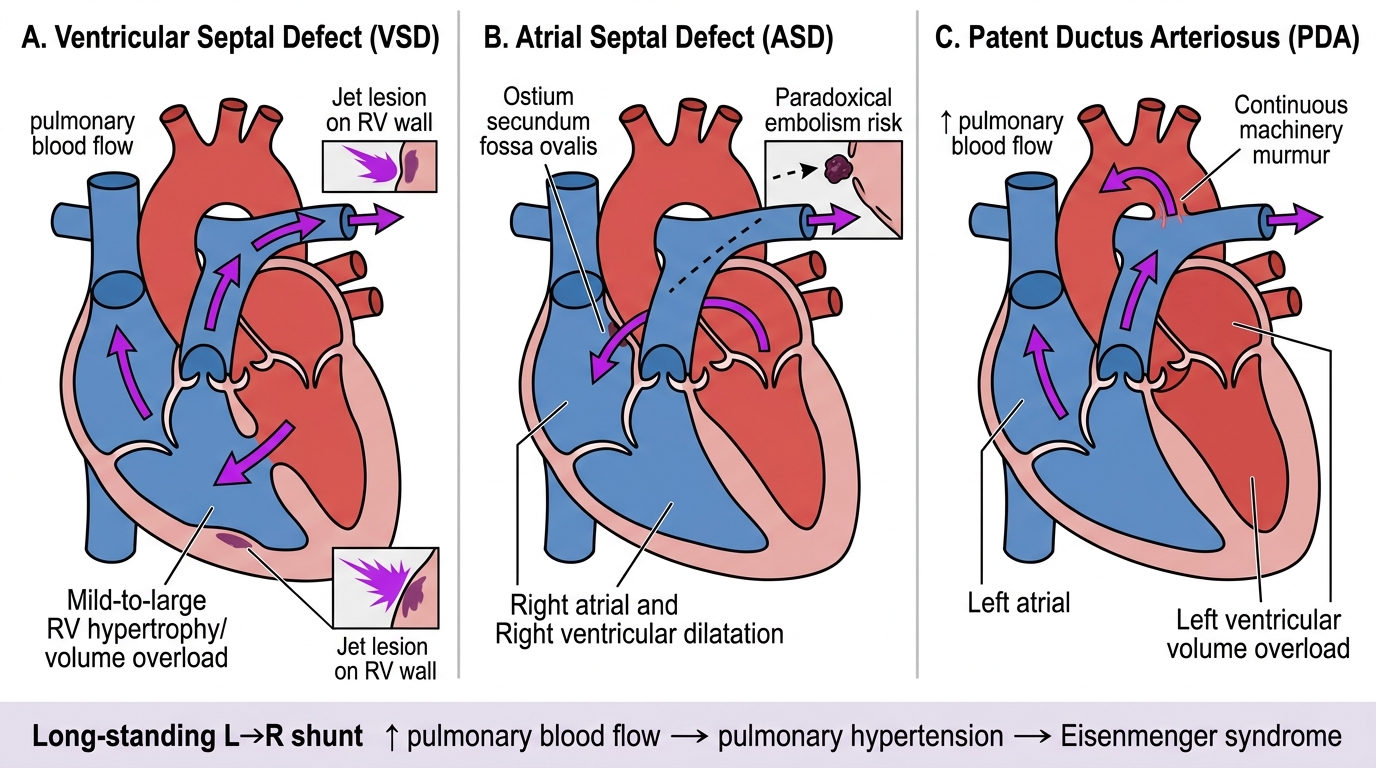
Ventricular septal defect (VSD) is the commonest congenital heart defect (~30% of all CHD). Most occur in the membranous septum (perimembranous VSD).
Pathophysiology: LV pressure > RV pressure → L→R shunt → increased pulmonary blood flow → right ventricular volume overload → pulmonary hypertension over years.
Gross: Defect in the interventricular septum; size determines haemodynamic significance. Small VSDs (Roger's disease) may close spontaneously. Large VSDs lead to RVH and eventually Eisenmenger.
Complications: Pulmonary hypertension, RV failure, infective endocarditis (jet lesion on RV wall), Eisenmenger syndrome.
Atrial septal defect (ASD) — commonest type is ostium secundum (fossa ovalis region). Ostium primum ASD is associated with Down syndrome.
Pathophysiology: LA pressure slightly > RA → L→R shunt → right heart volume overload → right atrial + ventricular dilatation, increased pulmonary flow.
Complications: Pulmonary hypertension (late), atrial arrhythmias, paradoxical embolism (venous thrombus crosses to systemic circulation → stroke).
Patent ductus arteriosus (PDA) — failure of the ductus arteriosus to close after birth. Common in premature infants and after first-trimester rubella.
Pathophysiology: Aortic pressure > pulmonary artery → L→R shunt → increased pulmonary flow → left heart volume overload.
Gross/clinical: Continuous ('machinery') murmur. Prostaglandin E1 keeps PDA open (used therapeutically in duct-dependent lesions); indomethacin (prostaglandin inhibitor) closes it medically in premature infants.
SELF-CHECK
A 35-year-old woman with a known large VSD since childhood is now found to have an oxygen saturation of 82% at rest. Her fingernails are clubbed and her lips are blue. Which mechanism best explains her current cyanosis?
A. Increased left-to-right shunting causing pulmonary oedema
B. Paradoxical embolism causing pulmonary infarction
C. Reversal of the shunt to right-to-left due to pulmonary hypertension
D. Infective endocarditis causing valve destruction
Reveal Answer
Answer: C. Reversal of the shunt to right-to-left due to pulmonary hypertension
This is Eisenmenger syndrome. The longstanding large L→R shunt caused progressive pulmonary hypertension, raising RV and pulmonary artery pressures until they equalled then exceeded systemic pressure. The shunt then reversed to R→L, sending deoxygenated blood directly into the systemic circulation. This is the pathological endpoint of any large uncorrected L→R shunt and is a contraindication to surgical closure.