Page 21 of 34
PA26.{4,9} | Congenital Heart Disease & Cardiomyopathies — SDL Guide (Part 2)
Eisenmenger Syndrome — Shunt Reversal
Eisenmenger Syndrome: Shunt Reversal
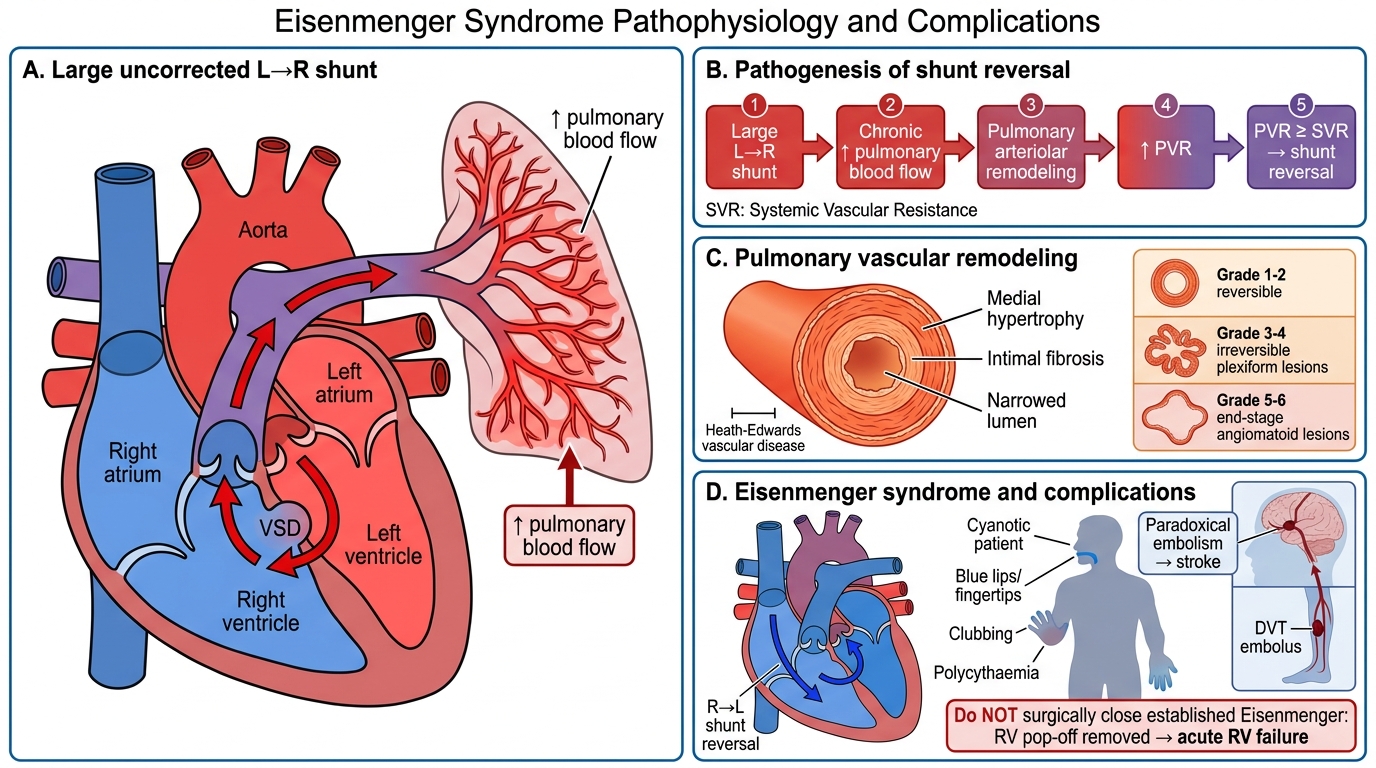
Eisenmenger syndrome is the final common pathway of large, uncorrected left-to-right shunts.
Mechanism:
1. Large L→R shunt → chronic increase in pulmonary blood flow
2. Pulmonary arterioles undergo medial hypertrophy and intimal fibrosis (Heath-Edwards grading of pulmonary vascular disease)
3. Pulmonary vascular resistance (PVR) rises progressively
4. When PVR ≥ systemic vascular resistance (SVR), shunt reverses → R→L
5. Deoxygenated blood enters systemic circulation → central cyanosis, clubbing, polycythaemia
Heath-Edwards changes (irreversible at Grade 4+):
• Grade 1-2: Medial hypertrophy, intimal proliferation — reversible with repair
• Grade 3-4: Plexiform lesions, fibrinoid necrosis — irreversible
• Grade 5-6: Angiomatoid lesions — end-stage
Clinical significance: Once Eisenmenger is established, surgical closure of the defect is contraindicated — it removes the 'pop-off valve' for the RV, causing acute RV failure. Only heart-lung transplantation offers cure.
CLINICAL PEARL
Paradoxical embolism is a life-threatening complication of any cardiac right-to-left communication. A deep vein thrombosis (DVT) travels to the right heart → crosses the defect → enters the systemic circulation → causes stroke or peripheral arterial occlusion. Even a small PFO (patent foramen ovale) — present in ~25% of adults — can transmit emboli during Valsalva manoeuvres that transiently raise right atrial pressure. Always think of paradoxical embolism in a young patient with cryptogenic stroke and no arterial risk factors.
Tetralogy of Fallot — The Archetypal Cyanotic CHD
Tetralogy of Fallot: Anatomy, Shunt, and Clinical Correlates
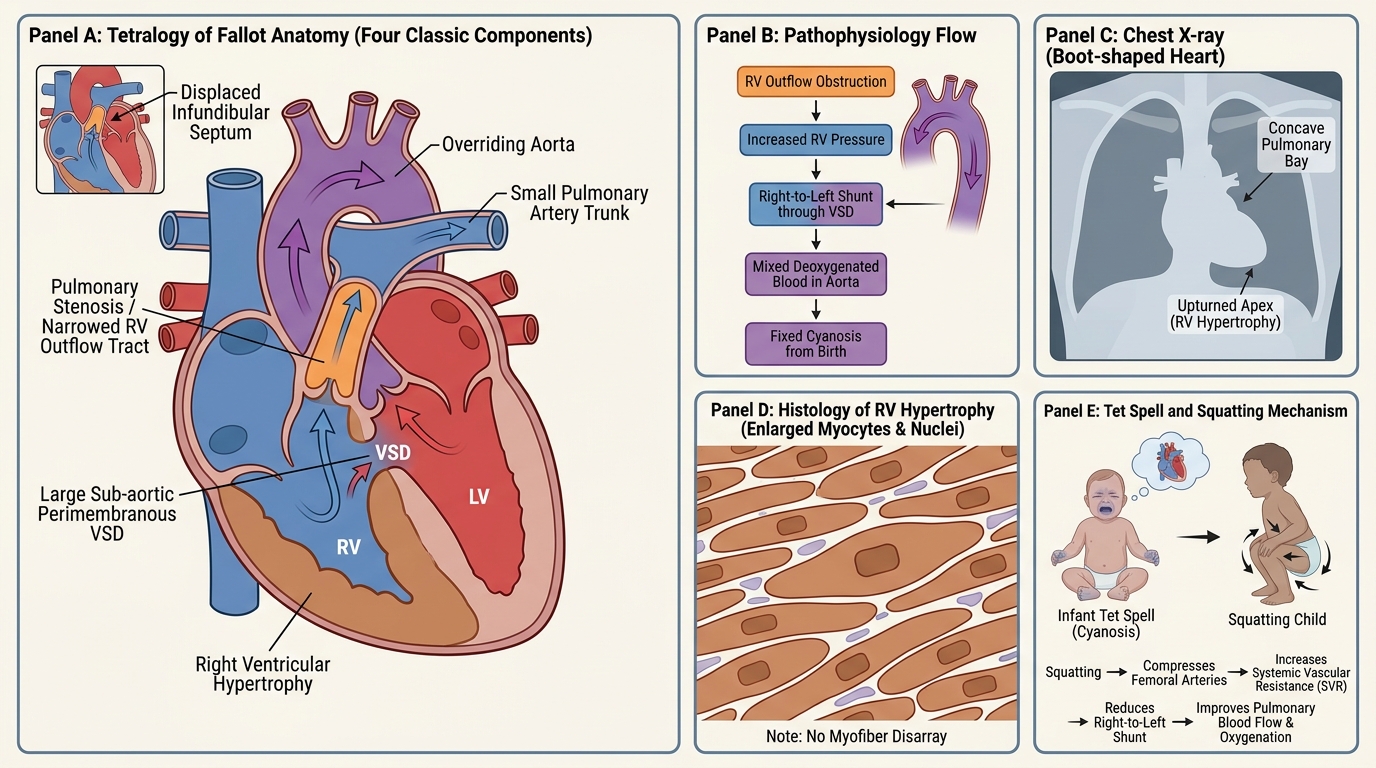
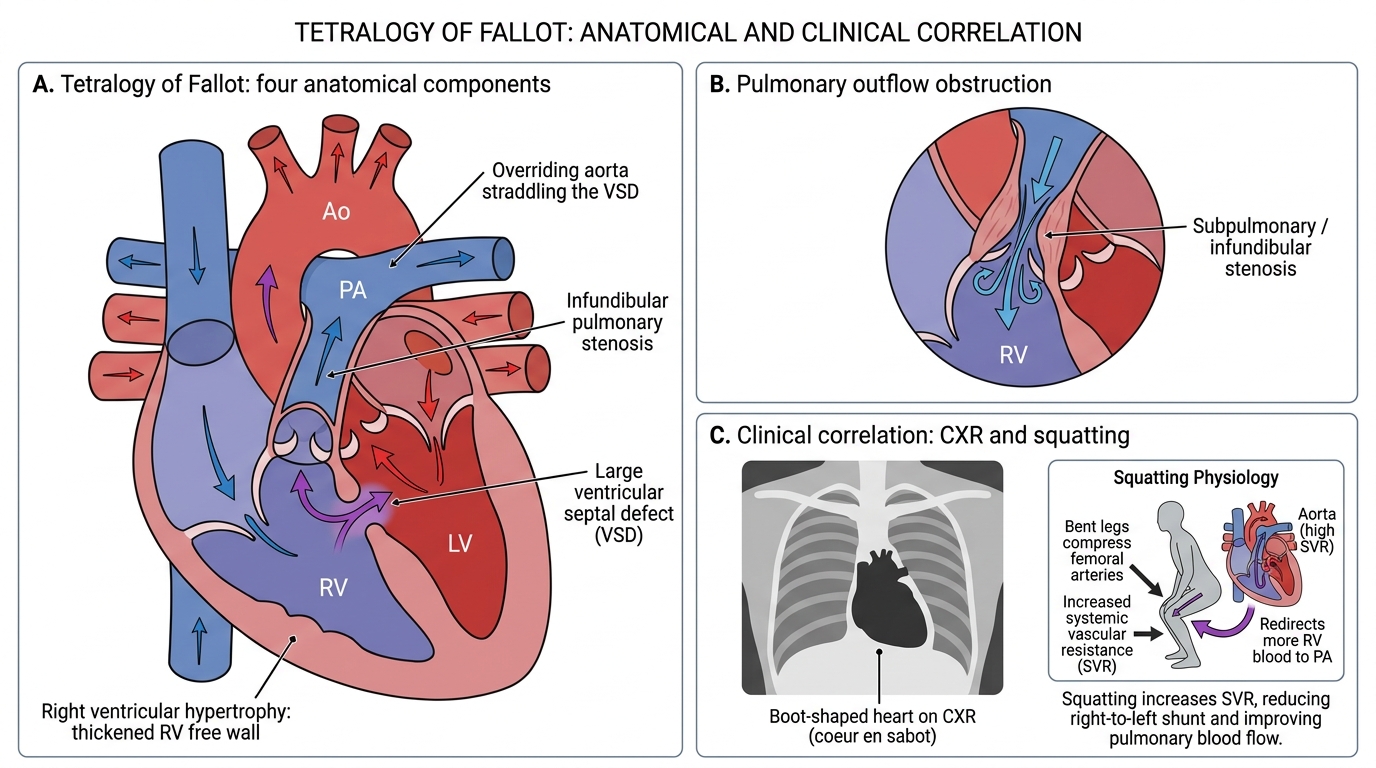
Tetralogy of Fallot (ToF) is the commonest cyanotic congenital heart defect, accounting for ~10% of all CHD. It arises from anterior-superior displacement of the infundibular (outlet) septum during development.
The 4 components (all follow from one developmental error):
1. Ventricular septal defect (large, sub-aortic, perimembranous)
2. Overriding aorta (aorta straddles the VSD, receiving blood from both ventricles)
3. Pulmonary stenosis (infundibular ± valvular; the obstruction that drives R→L shunting)
4. Right ventricular hypertrophy (consequence of obstruction, not a primary defect)
Pathophysiology: RV outflow obstruction → RV pressure rises ≥ LV pressure → blood preferentially exits via VSD → aorta receives deoxygenated blood → early, fixed cyanosis from birth.
Gross: Boot-shaped heart (coeur en sabot) on CXR — small pulmonary artery trunk, upturned apex from RVH, concave pulmonary bay.
Micro: RVH — increased myocyte diameter, enlarged nuclei, no disarray (unlike HOCM).
Tet spells (hypercyanotic episodes):
Sudden decrease in pulmonary blood flow → acute worsening cyanosis, loss of consciousness. Precipitated by crying, feeding, fever (↓SVR). Squatting raises SVR (compresses femoral arteries) → increases resistance to L→R flow → forces more blood through the pulmonary valve → temporarily improves oxygenation.
Complications: Polycythaemia (compensatory), paradoxical embolism, brain abscess (bypasses pulmonary filter), infective endocarditis, growth retardation.
Tetralogy of Fallot: Four Components and Clinical Correlation
SELF-CHECK
In Tetralogy of Fallot, why does squatting temporarily relieve the cyanotic spell?
A. Squatting increases venous return and dilates the pulmonary outflow tract
B. Squatting compresses femoral arteries, raising systemic vascular resistance and forcing more blood through the pulmonary valve
C. Squatting reduces heart rate and decreases myocardial oxygen demand
D. Squatting closes the overriding aorta by mechanical compression
Reveal Answer
Answer: B. Squatting compresses femoral arteries, raising systemic vascular resistance and forcing more blood through the pulmonary valve
Squatting kinks and compresses the large femoral arteries in the inguinal crease, acutely raising systemic vascular resistance (SVR). With SVR now higher than pulmonary resistance, the haemodynamic gradient favours pushing more RV blood through the narrow pulmonary valve into the lungs rather than across the VSD into the aorta. This transiently improves pulmonary blood flow and oxygenation.
Other Right-to-Left Shunts (The 5 Ts — Brief Overview)
Other Right-to-Left Shunts: The 5 Ts Beyond TOF
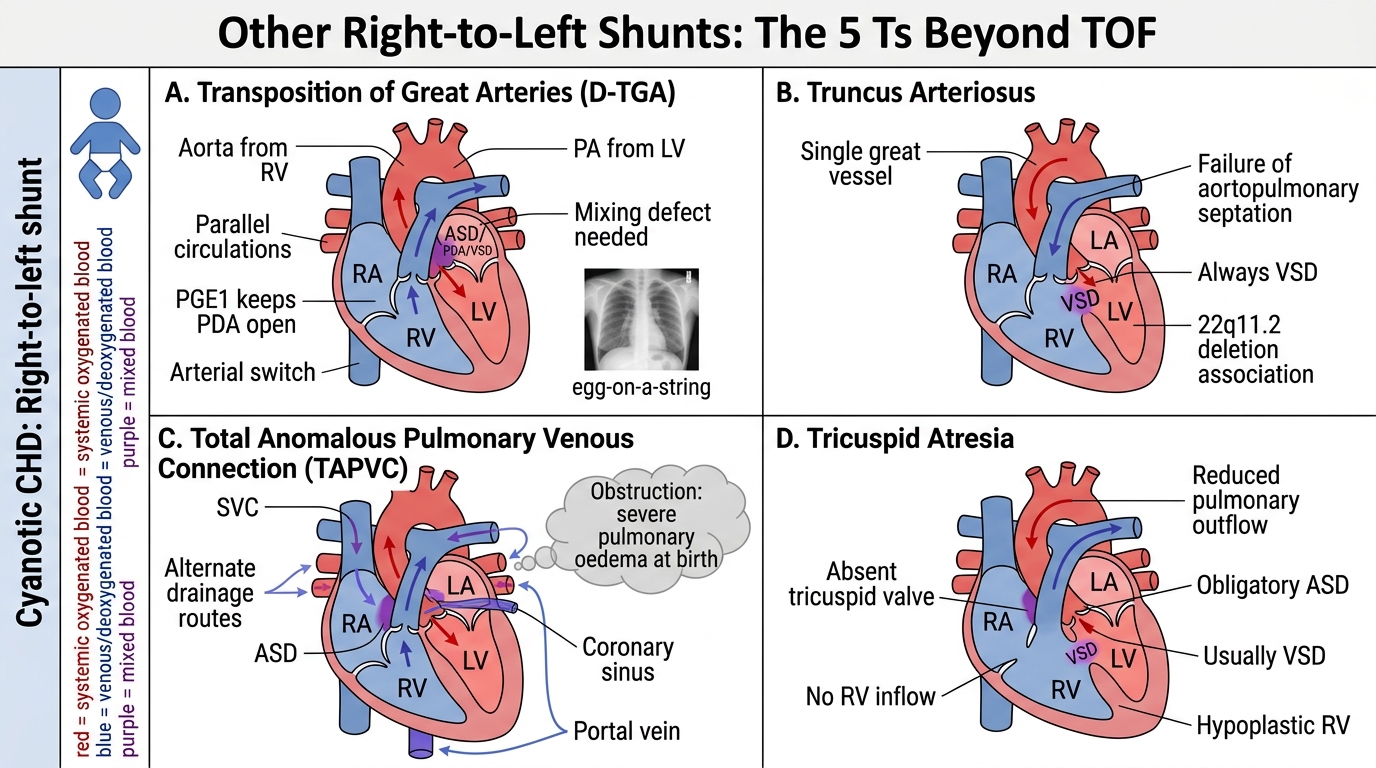
Beyond Tetralogy of Fallot, four other cyanotic defects complete the '5 Ts':
Transposition of great arteries (TGA): Aorta arises from RV; pulmonary artery from LV. Two parallel circulations incompatible with life unless a mixing defect (ASD, VSD, or PDA) coexists. D-TGA is the commonest cyanotic lesion presenting in the neonatal period (first hours of life). Egg-on-a-string CXR appearance. Emergency: maintain PDA with prostaglandin E1; definitive: arterial switch operation.
Truncus arteriosus: Single great vessel arises from both ventricles (failure of aortopulmonary septation). Always associated with VSD. Associated with 22q11.2 deletion.
Total anomalous pulmonary venous connection (TAPVC): All four pulmonary veins drain into the right side (portal vein, SVC, coronary sinus) instead of the LA. Requires mixing defect (ASD) to survive. May be obstructed → severe pulmonary oedema at birth.
Tricuspid atresia: Complete absence of tricuspid valve → no RV inflow → obligatory ASD + usually VSD for survival. Hypoplastic RV.