Page 22 of 34
PA26.{4,9} | Congenital Heart Disease & Cardiomyopathies — SDL Guide (Part 3)
Obstructive Lesions — Coarctation of Aorta
Coarctation of Aorta
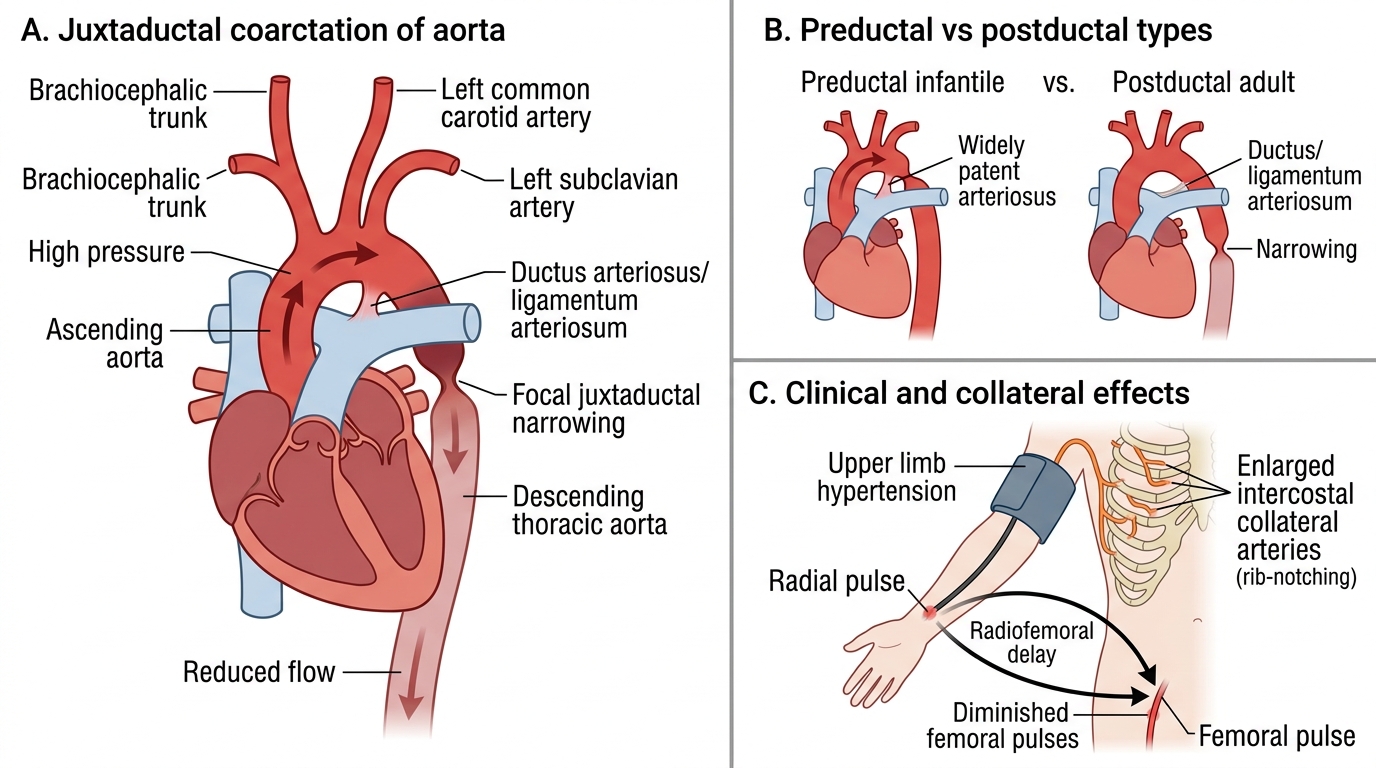
Coarctation of aorta is a discrete narrowing of the aortic lumen, classically near the ductus arteriosus (juxtaductal). Two types based on position relative to the ductus:
| Feature | Preductal (Infantile) | Postductal (Adult) |
|---|---|---|
| Position | Proximal to ductus | Distal to ductus |
| Ductus | Widely patent (required for lower body perfusion) | Closed/ligamentum |
| Presentation | Neonatal heart failure | Hypertension in young adult |
| Lower limb pulses | Diminished/absent | Diminished; radiofemoral delay |
| Collaterals | Not developed | Well-developed intercostal collaterals |
Associations: Turner syndrome (45,X) — bicuspid aortic valve + coarctation is the classic pairing.
Gross: Ridge/shelf of intimal and medial tissue narrowing the lumen. Dilated proximal aorta. Collateral channels — internal mammary, intercostal arteries enlarge → rib notching on CXR (3–9th ribs bilaterally).
Complications: Hypertension (upper body), LV hypertrophy, aortic dissection/rupture, IE, intracranial haemorrhage (Circle of Willis aneurysms from hypertension).
Haemodynamic 'E' sign / '3' sign on CXR: indentation of the aorta between the proximal dilation and post-stenotic dilation.
SELF-CHECK
A 19-year-old woman with Turner syndrome (45,X) is found to have blood pressure 160/90 mmHg in both arms but weak and delayed femoral pulses bilaterally. Chest X-ray shows rib notching (ribs 3–9). What is the most likely cardiac finding?
A. Postductal coarctation of aorta with intercostal collateral vessels
B. Preductal coarctation of aorta with patent ductus arteriosus
C. Bicuspid aortic valve with aortic regurgitation
D. Atrial septal defect with pulmonary hypertension
Reveal Answer
Answer: A. Postductal coarctation of aorta with intercostal collateral vessels
The combination of hypertension in the upper extremities with radiofemoral delay, rib notching (due to enlarged intercostal collateral arteries), and Turner syndrome (45,X) is the classic presentation of postductal (adult-type) coarctation of the aorta. The ductus is closed (ligamentum arteriosum), so intercostal collaterals have had years to develop, eroding the inferior rib margins. Turner syndrome also commonly includes a bicuspid aortic valve.
Cardiomyopathies — Classification and Overview
Cardiomyopathies: Classification and Functional Overview
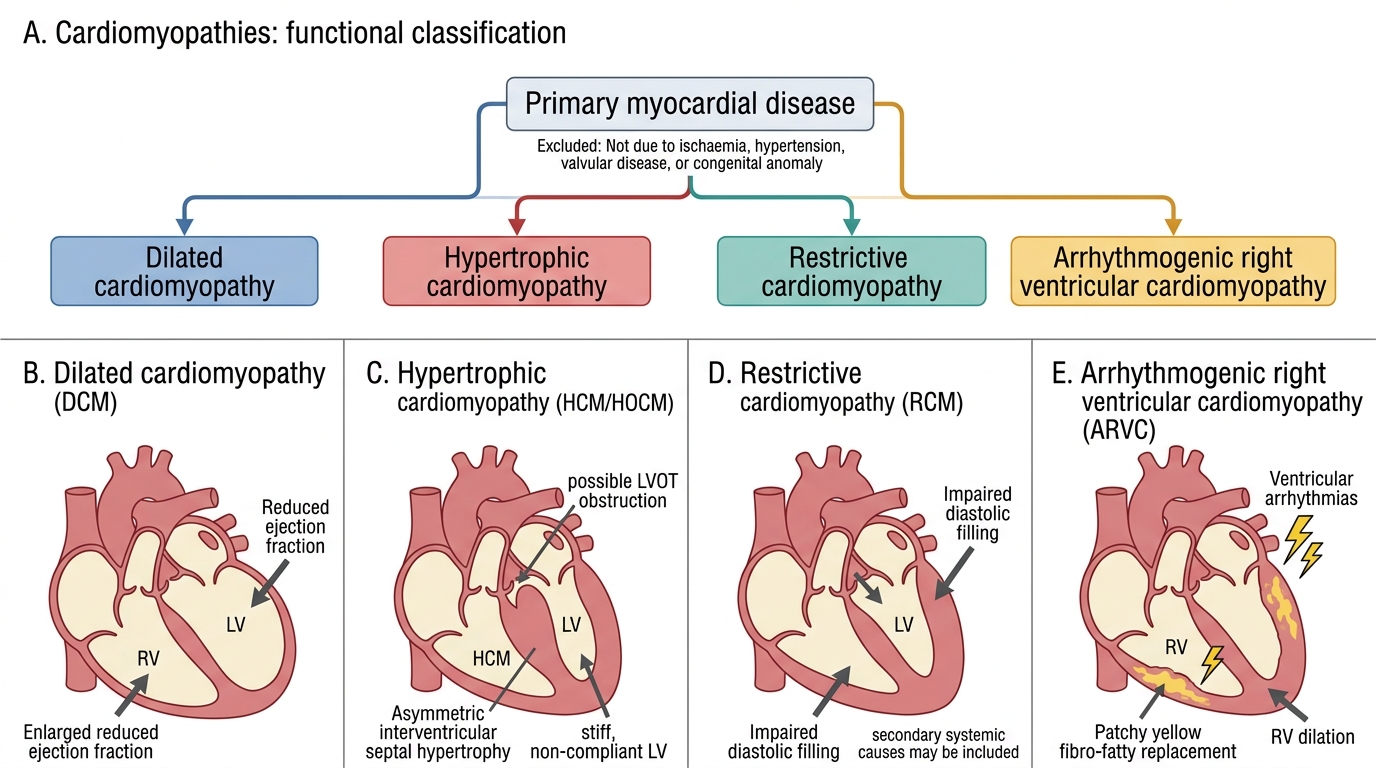
Cardiomyopathies are primary diseases of the myocardium not caused by ischaemia, hypertension, valvular disease, or congenital anomalies (though secondary cardiomyopathies from systemic disease are included in the restrictive group).
The WHO/ESC classification recognises three main functional types:
| Type | Dominant Defect | Chamber Change | Function |
|---|---|---|---|
| Dilated (DCM) | Systolic failure | 4-chamber dilatation + ↑ wall stress | EF markedly reduced |
| Hypertrophic (HCM/HOCM) | Diastolic failure ± LVOT obstruction | Asymmetric septal hypertrophy | EF normal or ↑; stiff, non-compliant LV |
| Restrictive (RCM) | Diastolic failure | Normal/↓ cavity; stiff walls | EF normal; impaired filling |
A fourth category, arrhythmogenic right ventricular cardiomyopathy (ARVC), involves fibrofatty replacement of the RV myocardium.
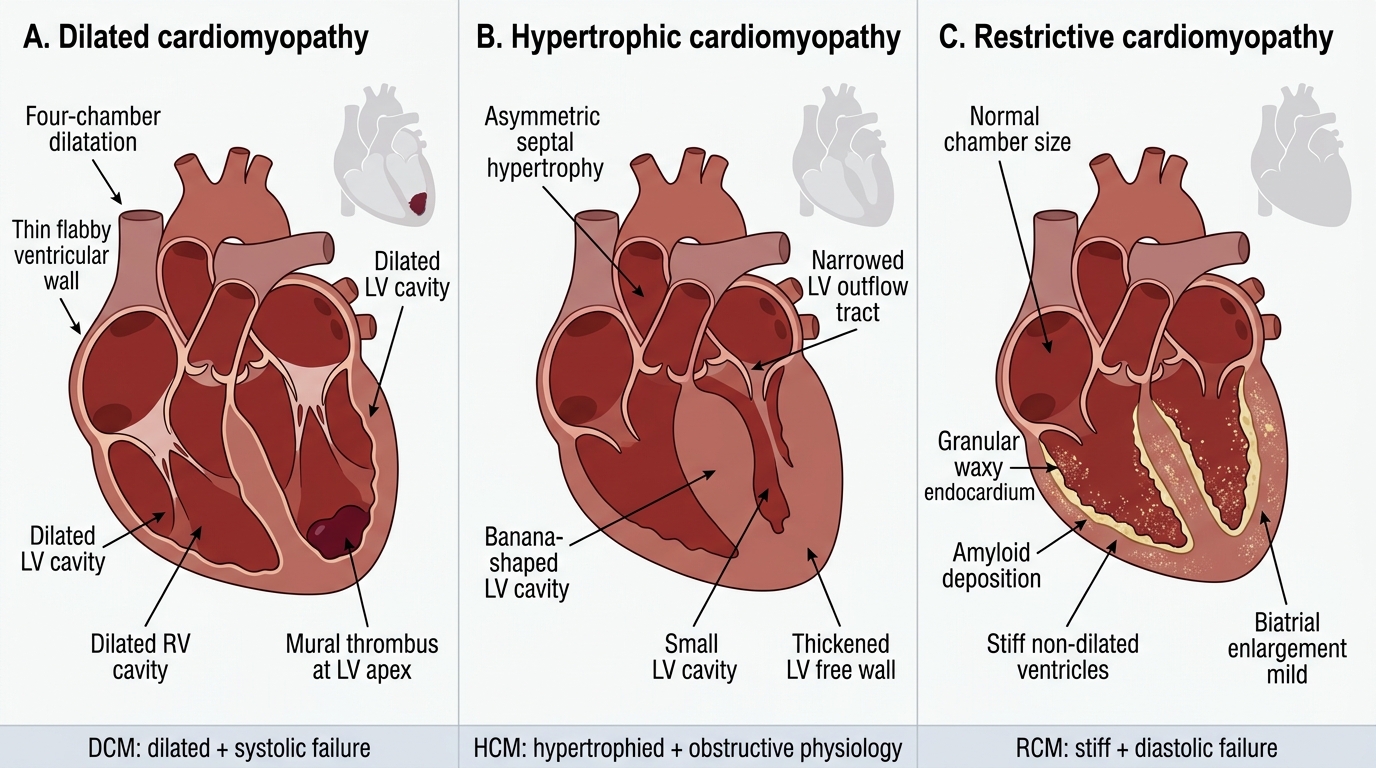
Gross Comparison of Cardiomyopathy Types
Dilated Cardiomyopathy — Pathology and Causes
Dilated Cardiomyopathy: Pathology and Causes
Dilated cardiomyopathy (DCM) is the commonest cardiomyopathy and the leading cause of cardiac transplantation.
Causes:
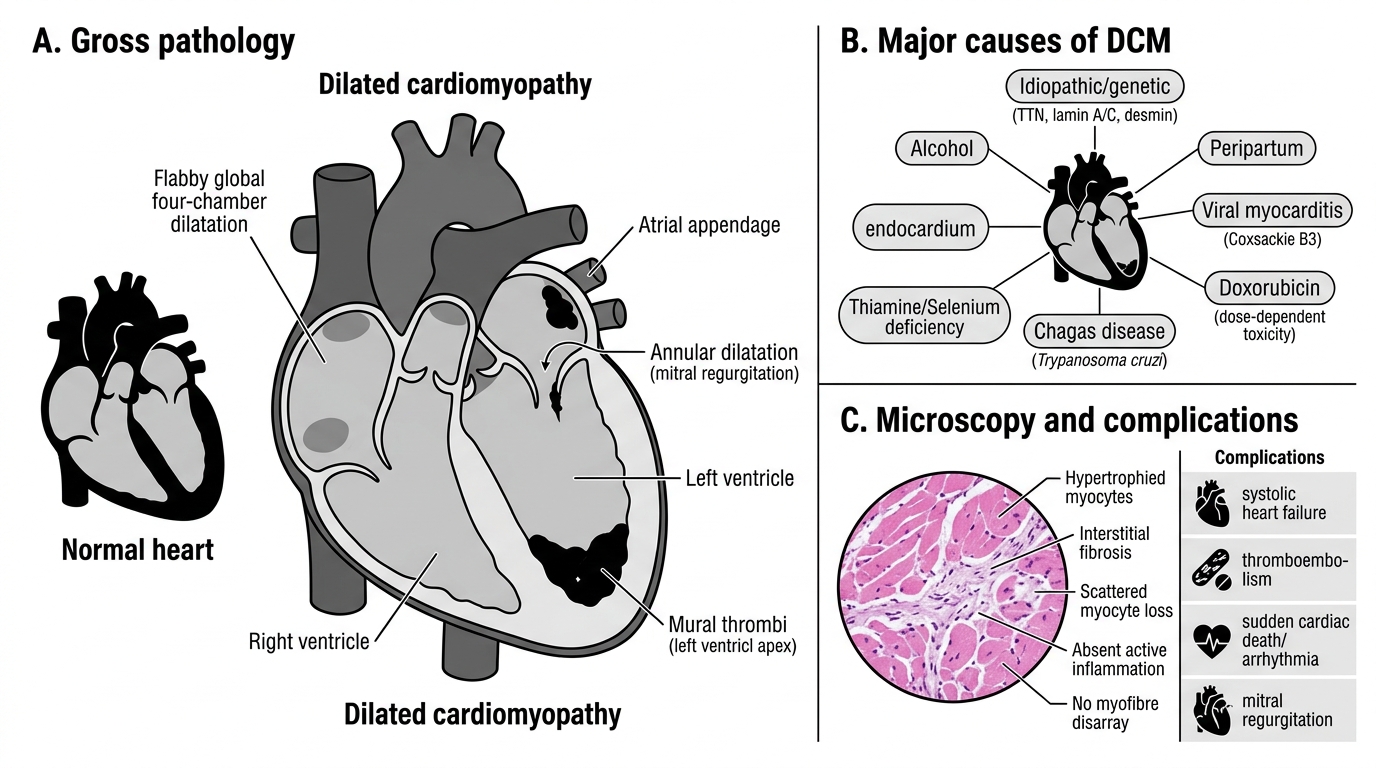
• Idiopathic (~50%) — many have underlying genetic mutations (titin, lamin A/C, desmin — cytoskeletal proteins)
• Genetic (~25%) — familial DCM; autosomal dominant; titin (TTN) mutations most common
• Alcohol — toxic myopathy; reversible in early stages
• Peripartum cardiomyopathy — onset last month of pregnancy or first 5 months postpartum; immune/prolactin-mediated
• Viral myocarditis → post-inflammatory DCM (Coxsackievirus B3, parvovirus B19, CMV)
• Doxorubicin (Adriamycin) — cumulative dose-dependent free-radical toxicity to mitochondria; irreversible above 550 mg/m²
• Chagas disease — Trypanosoma cruzi; important in South America
• Nutritional — thiamine deficiency (beriberi), selenium deficiency (Keshan disease)
Gross: Flabby, dilated all four chambers (biventricular > right-dominant). Endocardium pallid, thin. Mural thrombi common in LV apex and atrial appendages.
Micro: Myocyte hypertrophy (compensatory), interstitial fibrosis, scattered myocyte loss. Inflammation absent (distinguishes from active myocarditis). No myofibre disarray.
Complications: Heart failure (systolic), thromboembolism, sudden cardiac death (arrhythmia), mitral regurgitation (annular dilatation).