Page 23 of 34
PA26.{4,9} | Congenital Heart Disease & Cardiomyopathies — SDL Guide (Part 4)
Hypertrophic Cardiomyopathy (HOCM) — Pathology and Genetics
Hypertrophic Obstructive Cardiomyopathy: Pathology and Genetics
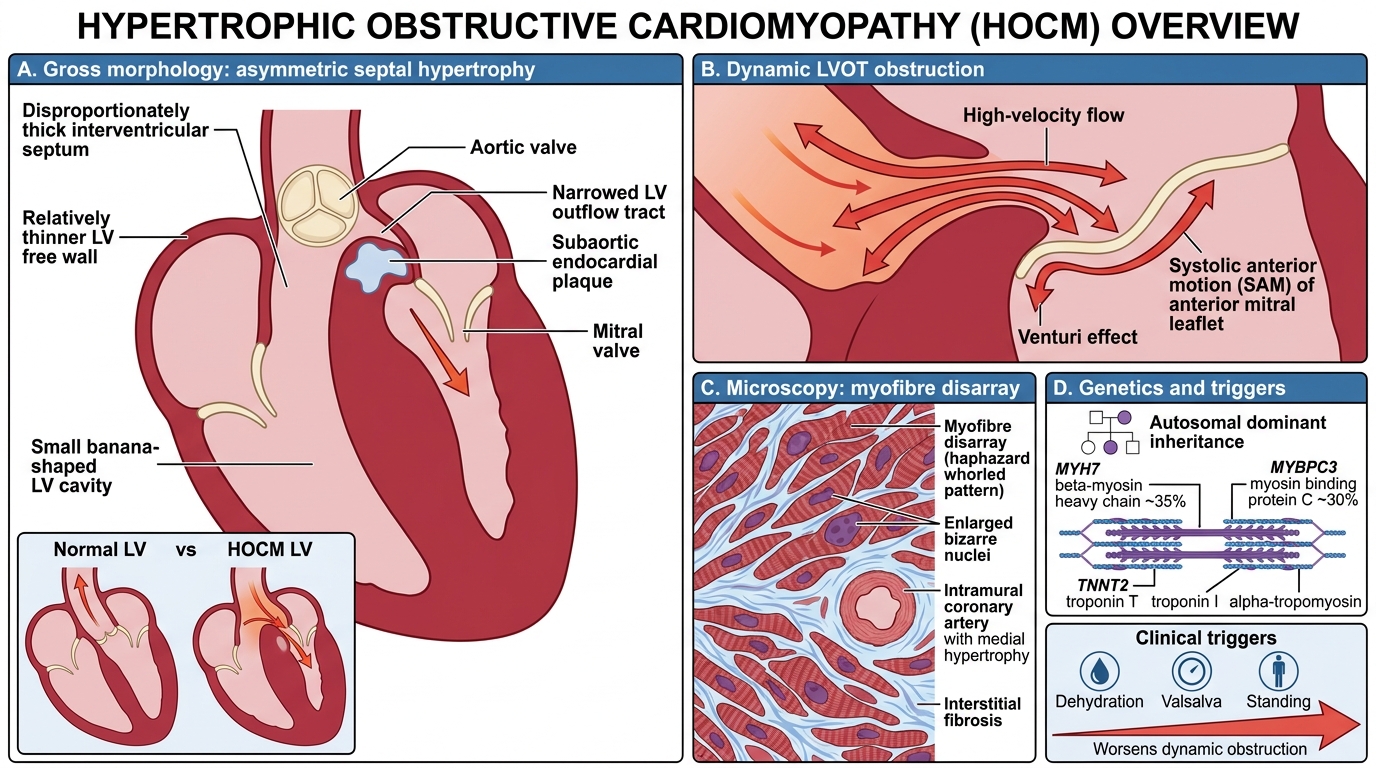
Hypertrophic cardiomyopathy (HCM) is characterised by left ventricular hypertrophy in the absence of an obvious cause (no hypertension, no aortic stenosis). When the hypertrophy obstructs the left ventricular outflow tract (LVOT), it is termed hypertrophic obstructive cardiomyopathy (HOCM).
Genetics: Autosomal dominant; mutations in sarcomere protein genes.
• Beta-myosin heavy chain (MYH7) — most common (~35%)
• Myosin binding protein C (MYBPC3) — ~30%
• Also: troponin T (TNNT2), troponin I, alpha-tropomyosin
Penetrance is variable; 60% have an identifiable mutation.
Gross: Asymmetric septal hypertrophy (ASH) — interventricular septum disproportionately thickened (septum:free wall ratio >1.3:1). LV cavity is small, banana-shaped. Subaortic endocardial plaque (friction from SAM).
Micro (pathognomonic): Myofibre disarray — myocytes in haphazard, whorled ('fish-scale') pattern instead of parallel arrays. Myocyte hypertrophy with bizarre, enlarged nuclei. Interstitial and replacement fibrosis. Small vessel disease (intramural coronary arteries with medial hypertrophy → ischaemia).
LVOT obstruction mechanism:
1. Asymmetric septal hypertrophy narrows the LVOT
2. High-velocity flow through narrowed LVOT creates Venturi effect
3. Systolic anterior motion (SAM) of the mitral valve — anterior mitral leaflet is sucked towards septum, further obstructing LVOT
4. Dynamic obstruction — worse with dehydration, Valsalva, standing (↓preload); better with squatting, passive leg raise (↑preload)
Complications: Sudden cardiac death (SCD) — especially in young athletes (commonest cause of SCD in <35 years in USA); ventricular arrhythmias on exertion. Heart failure (diastolic). Mitral regurgitation (SAM). Infective endocarditis.
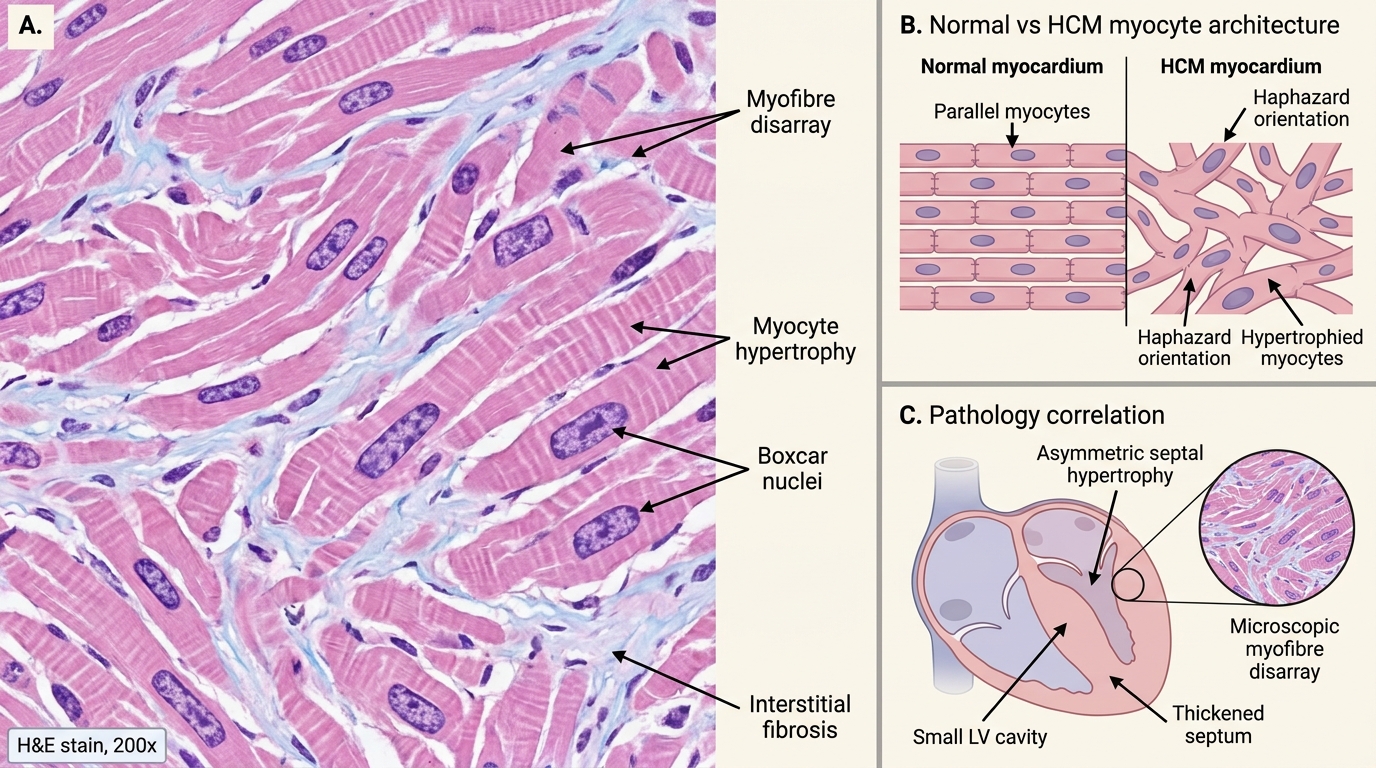
Hypertrophic Cardiomyopathy: Myofibre Disarray
CLINICAL PEARL
HOCM and the young athlete who collapses: HOCM is the commonest identifiable cause of sudden cardiac death in athletes under 35 in Western countries (in contrast, anomalous coronary artery origin is second). The typical scenario: an apparently healthy young person collapses and dies during or just after vigorous exercise. Exertion → ↑ heart rate, ↓ filling time, ↓ preload → worsening LVOT obstruction → VF → sudden death. Pre-participation ECG screening picks up ST/T changes and LVH in ~50% of HOCM cases — this is the rationale for mandatory cardiac screening in competitive athletes.
SELF-CHECK
On microscopy, a 28-year-old male athlete who died suddenly shows markedly hypertrophied myocytes arranged in haphazard whorled patterns with interstitial fibrosis. Which protein mutation is most commonly responsible for this condition?
A. Titin (TTN) — cytoskeletal scaffolding protein
B. Desmoplakin (DSP) — desmosomal protein
C. Emerin (EMD) — nuclear envelope protein
D. Beta-myosin heavy chain (MYH7) — sarcomere thick filament protein
Reveal Answer
Answer: D. Beta-myosin heavy chain (MYH7) — sarcomere thick filament protein
The haphazard myofibre disarray is pathognomonic of hypertrophic cardiomyopathy (HCM). The most commonly mutated gene is MYH7 (beta-myosin heavy chain), accounting for ~35% of familial HCM. MYBPC3 (myosin binding protein C) is the second most common. Both are sarcomere proteins whose mutations cause abnormal contractile mechanics and compensatory hypertrophy with disarray. Titin mutations cause dilated cardiomyopathy; desmoplakin and emerin mutations cause ARVC and Emery-Dreifuss muscular dystrophy with cardiomyopathy, respectively.
Restrictive Cardiomyopathy — Types and Indian Relevance
Restrictive Cardiomyopathy: Types and Indian Relevance
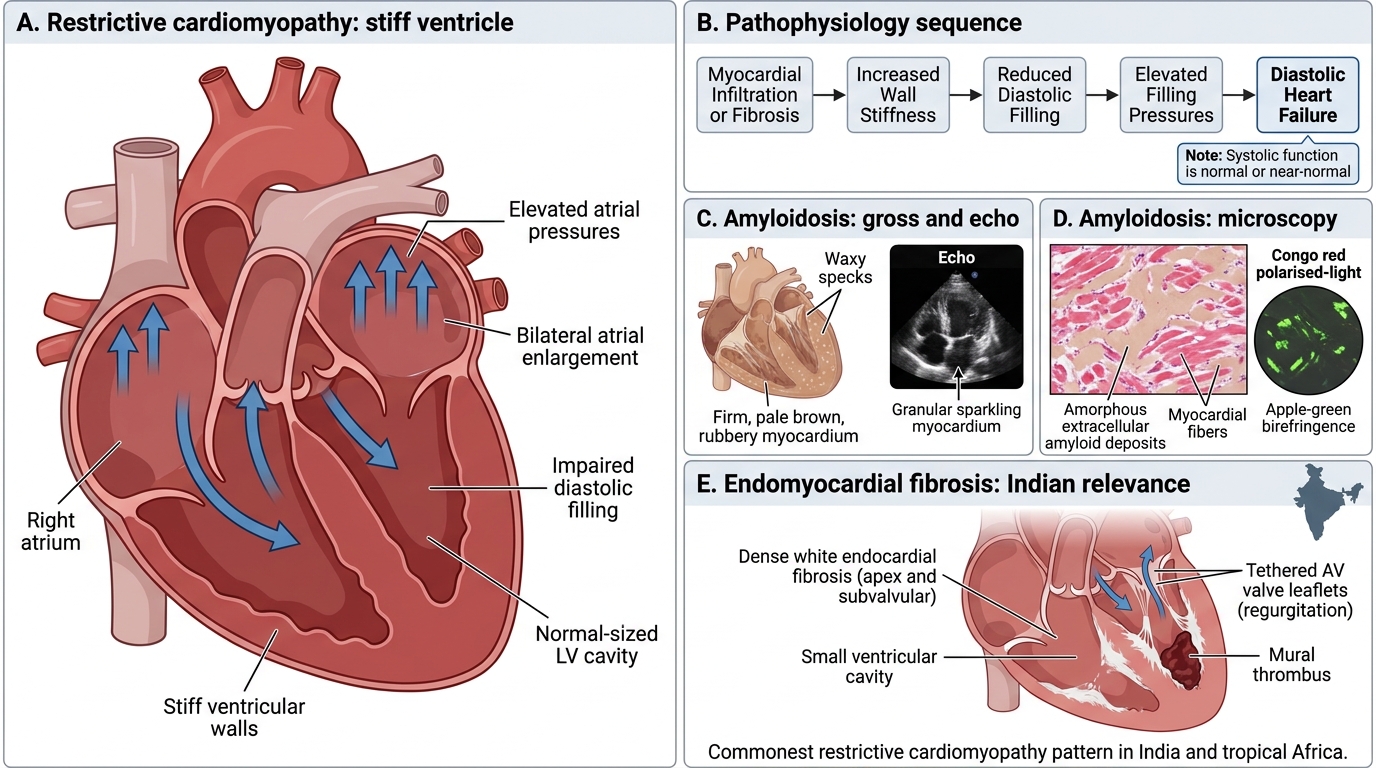
Restrictive cardiomyopathy (RCM) is characterised by decreased ventricular compliance (stiff ventricle) with normal or near-normal systolic function. The ventricle cannot relax and fill adequately → diastolic heart failure → ↑ atrial pressures → bilateral atrial enlargement.
Pathophysiology: Infiltration or fibrosis of the myocardium ↑ wall stiffness → ↓ diastolic filling → normal-sized LV cavity with markedly elevated filling pressures → mimics constrictive pericarditis clinically.
Causes of restrictive cardiomyopathy:
1. Amyloidosis — commonest cause in developed countries
• Amyloid fibrils (AL or transthyretin) deposit in interstitium → granular, 'sparkling' appearance on echo
• Gross: heart is firm, rubbery, pale brown; cut surface has waxy specks
• Micro: pink amorphous extracellular deposits — Congo red stain → apple-green birefringence under polarised light
2. Endomyocardial fibrosis (EMF) — commonest in India and tropical Africa; highly relevant for Indian medical students
• Fibrous obliteration of the ventricular apex(es), typically bilateral
• Aetiology: unclear — eosinophilic inflammation (Löffler endocarditis) → organisation → fibrosis; nutritional factors, autoimmunity
• Gross: dense white endocardial fibrosis, particularly at apex and subvalvular region; small cavity
• Complications: restrictive physiology, AV valve regurgitation (fibrosis tethers leaflets), mural thrombus
- Sarcoidosis — non-caseating granulomas replacing myocardium; predilection for conduction system → heart block + sudden death
- Haemochromatosis — iron deposits in myocytes → rusty brown discolouration on gross; Perls' Prussian blue stain positive
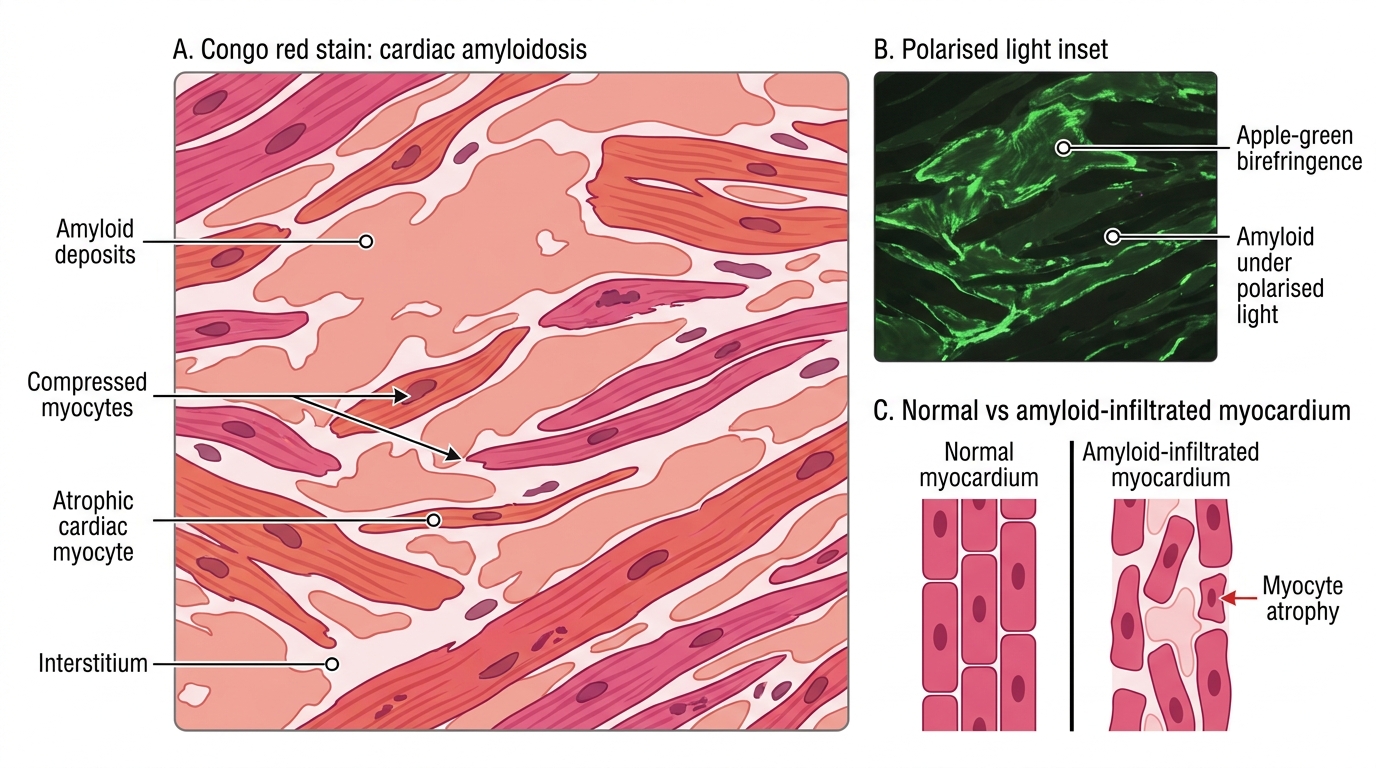
Cardiac Amyloidosis: Congo Red and Polarised Light
Myocarditis — Brief Overview
Myocarditis: Causes, Pathology, Diagnosis, and Outcomes
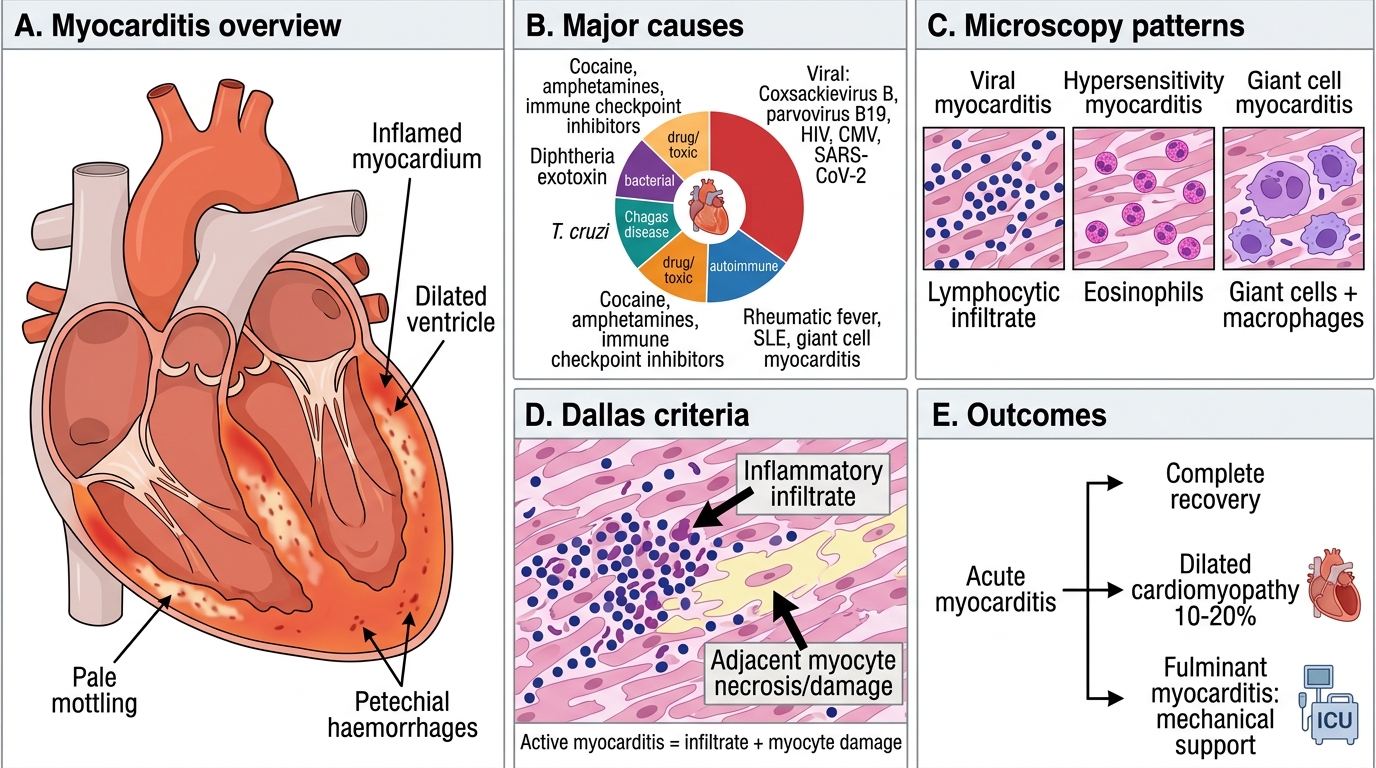
Myocarditis is inflammation of the myocardium, most commonly viral, and is an important precursor to dilated cardiomyopathy.
Causes:
• Viral (most common) — Coxsackievirus B (most important), parvovirus B19, HIV, CMV, SARS-CoV-2
• Bacterial — diphtheria (exotoxin-mediated — the clinically important one; toxin inhibits protein synthesis in myocardium + peripheral nerves)
• Chagas disease — T. cruzi; chronic form leads to DCM and conduction defects
• Autoimmune — rheumatic fever (pancarditis), SLE, giant cell myocarditis (rare but fulminant)
• Drug/toxic — cocaine, amphetamines, immune checkpoint inhibitors (cancer therapy)
Gross: Flabby, dilated, pale/mottled myocardium. Petechial haemorrhages in acute phase.
Micro: Diffuse interstitial inflammatory infiltrate (lymphocytes in viral; eosinophils in hypersensitivity; giant cells with macrophages in giant cell myocarditis). Myocyte necrosis in severe cases.
Dallas criteria (histological diagnosis): active myocarditis = inflammatory infiltrate + adjacent myocyte necrosis/damage.
Outcome: Complete recovery (most), progression to DCM (~10–20%), fulminant myocarditis requiring mechanical support.
SELF-CHECK
A 45-year-old woman in South India presents with progressive breathlessness, bilateral ankle oedema, and marked ascites. Echocardiography shows bilateral ventricular apex obliteration and restrictive filling pattern with normal ejection fraction. Which pathological process explains this picture?
A. Amyloid infiltration of the ventricular myocardium
B. Asymmetric septal hypertrophy causing diastolic dysfunction
C. Fibrous obliteration of the ventricular apices due to endomyocardial fibrosis
D. Viral myocarditis leading to post-inflammatory cardiomyopathy
Reveal Answer
Answer: C. Fibrous obliteration of the ventricular apices due to endomyocardial fibrosis
The combination of bilateral ventricular apex obliteration, restrictive filling pattern, preserved ejection fraction, and a South Indian patient is the classic presentation of endomyocardial fibrosis (EMF). EMF is the most common cause of restrictive cardiomyopathy in India and tropical Africa. The dense endocardial fibrosis obliterates the apices and tethers the AV valve leaflets. The markedly elevated venous pressures explain the ascites — RV involvement is common. Amyloid also causes restriction but shows interstitial infiltration, not apex obliteration.
Complications Summary — CHD and Cardiomyopathies
Complications of CHD and Cardiomyopathies
Understanding the complications logically (rather than memorising lists) requires tracing the haemodynamic consequences:
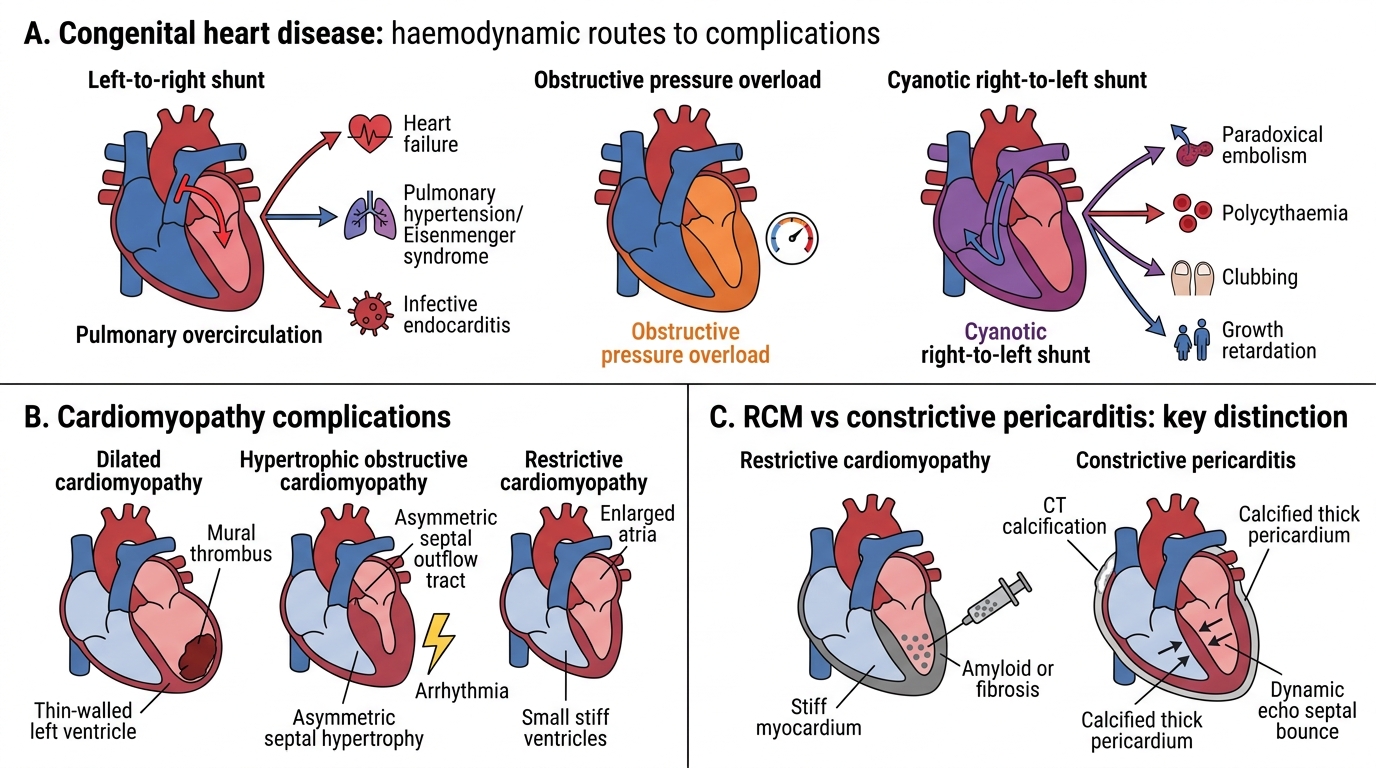
Congenital Heart Disease — shared complications:
• Heart failure — volume overload (L→R shunts), pressure overload (obstructive), or cyanotic defects (hypoxia → myocardial dysfunction)
• Pulmonary hypertension → Eisenmenger syndrome — any large L→R shunt
• Infective endocarditis (IE) — turbulent flow creates jet lesion on endocardium/valves → nidus for bacteria
• Paradoxical embolism — any right-to-left communication, including post-Eisenmenger reversal
• Polycythaemia — chronic hypoxia stimulates EPO → ↑ RBCs → hyperviscosity, thrombosis, gout
• Clubbing — chronic peripheral hypoxia → periosteal + soft tissue changes
• Growth retardation — chronic cyanosis and heart failure impair somatic growth
Cardiomyopathy complications:
• DCM: systolic heart failure, mural thrombus/embolism, AF, sudden death
• HCM/HOCM: sudden death (young athletes), diastolic failure, AF, IE
• RCM: diastolic failure, mimics constrictive pericarditis, AF, thrombus
Key distinction: RCM and constrictive pericarditis are haemodynamically similar (elevated filling pressures, small cavity, normal EF) but distinguishable by:
• Pericardial calcification on CT — favours constrictive
• Septal bounce (interventricular dependence) on echo — favours constrictive
• Endomyocardial biopsy — positive in RCM (amyloid, fibrosis)