Page 13 of 34
PA26.3 | Heart Failure — SDL Guide (Part 3)
Pathology of the Failing Heart
Pathology of the Failing Heart
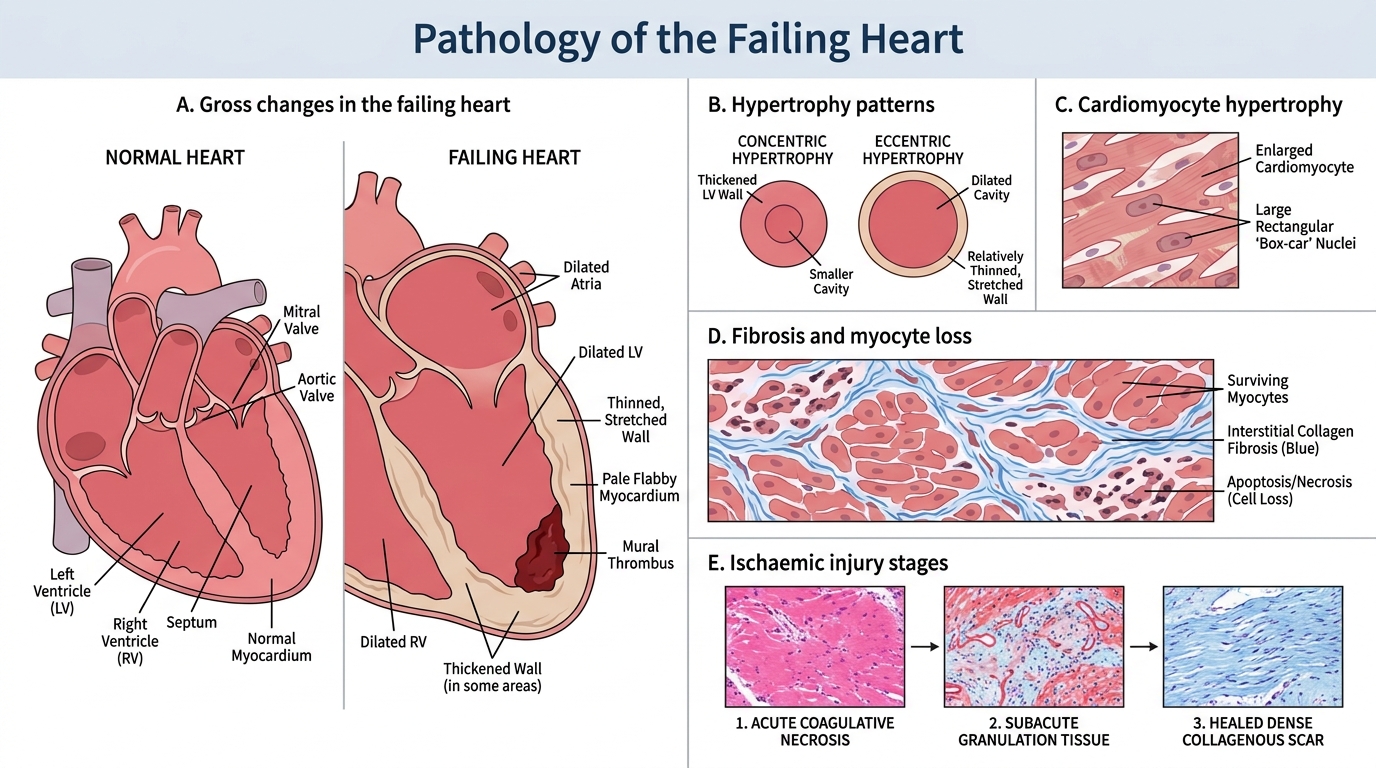
The heart itself undergoes predictable structural changes that vary by aetiology and duration.
Gross pathology:
- Dilatation: all types of heart failure that have progressed sufficiently show ventricular enlargement. The cavity appears widened; in severe cases the heart may weigh 2-3× normal (normal ~300-350 g in adults).
- Hypertrophy: wall thickness > 15 mm (LV) is hypertrophy. Concentric = pressure-loaded wall, eccentric = volume-loaded thinned wall.
- Pale, flabby myocardium: in dilated cardiomyopathy or end-stage ischaemic disease, the myocardium appears pale and soft (fatty change, atrophy, fibrosis).
- Mural thrombi: in dilated, poorly contractile ventricles, stasis predisposes to mural thrombus formation (see complications below).
Microscopic pathology:
- Cardiomyocyte hypertrophy: enlarged cells with large, "box-car" nuclei.
- Interstitial and replacement fibrosis (activated by angiotensin II, TGF-β, aldosterone).
- Myocyte loss by apoptosis and necrosis.
- In ischaemic heart disease: coagulative necrosis (acute), granulation tissue (subacute), dense collagenous scar (healed).
Complications of Heart Failure
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Complications of Heart Failure
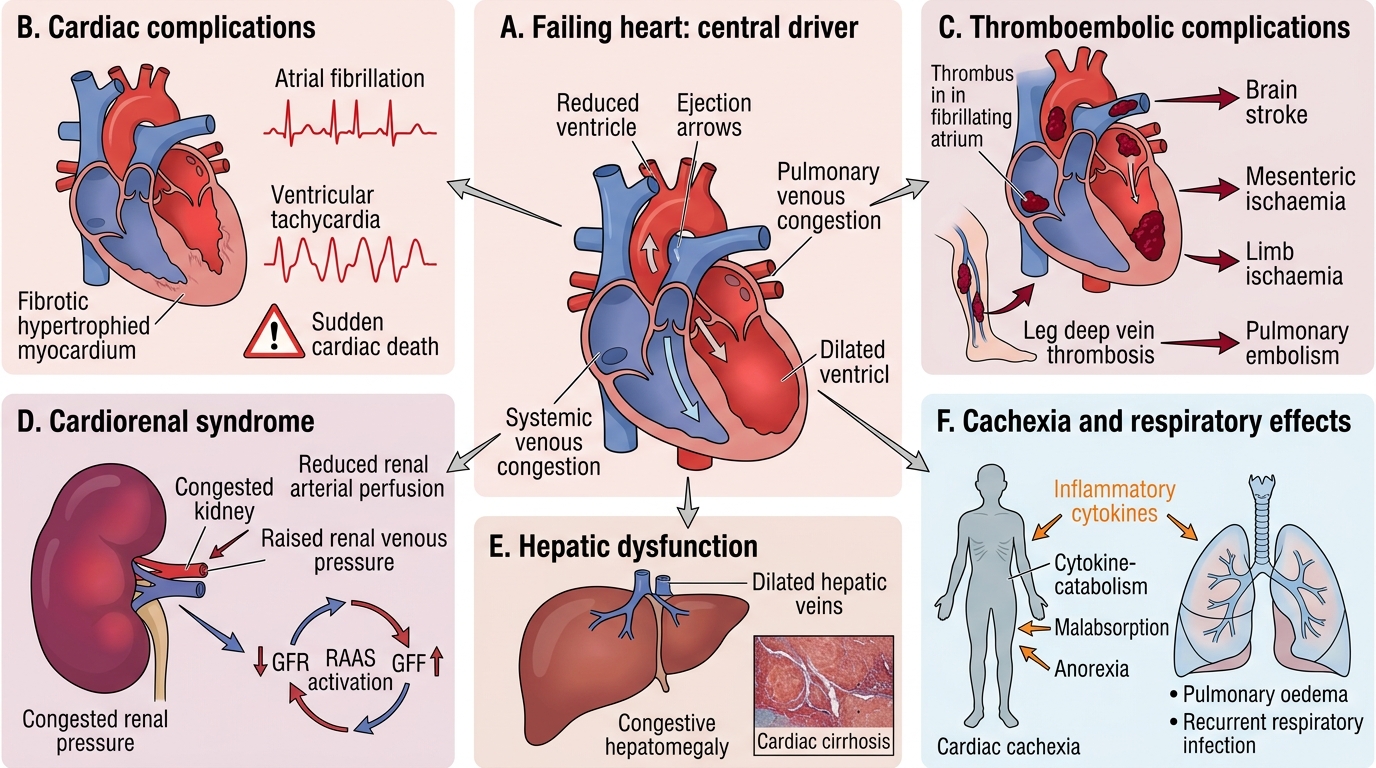
Heart failure is not a static endpoint — it spawns a cascade of complications across multiple organs.
Cardiac complications:
- Arrhythmias: the hypertrophied, fibrosed, neurohormone-bathed myocardium is an arrhythmogenic substrate. Atrial fibrillation is present in up to 50% of patients with advanced HF. Ventricular arrhythmias (VT/VF) cause sudden cardiac death — the commonest mode of death in HF (competing with progressive pump failure).
- Sudden cardiac death: accounts for ~50% of HF mortality, predominantly via ventricular arrhythmia.
Thromboembolic complications:
- Mural thrombus in dilated ventricles or fibrillating atria → systemic arterial emboli → stroke, mesenteric ischaemia, limb ischaemia.
- Venous stasis (low cardiac output + immobility) → deep vein thrombosis → pulmonary embolism.
Renal dysfunction (cardiorenal syndrome):
- Reduced renal perfusion (low cardiac output) + venous congestion (raised renal venous pressure) → ↓GFR → acute kidney injury or progressive chronic kidney disease. RAAS activation worsens this cycle.
Hepatic dysfunction:
- Congestive hepatomegaly, cardiac cirrhosis (as above). Synthetic failure in advanced cases.
Cardiac cachexia:
- Progressive weight loss (fat + lean mass) in chronic HF. Mechanisms: reduced mesenteric perfusion → malabsorption; elevated pro-inflammatory cytokines (TNF-α, IL-6) → catabolism; anorexia from hepatic distension.
Respiratory failure: in acute decompensated LHF — alveolar oedema → hypoxaemia → respiratory acidosis if severe.
Staging, Classification, and BNP as Biomarker
Heart Failure Classification and BNP Biomarker
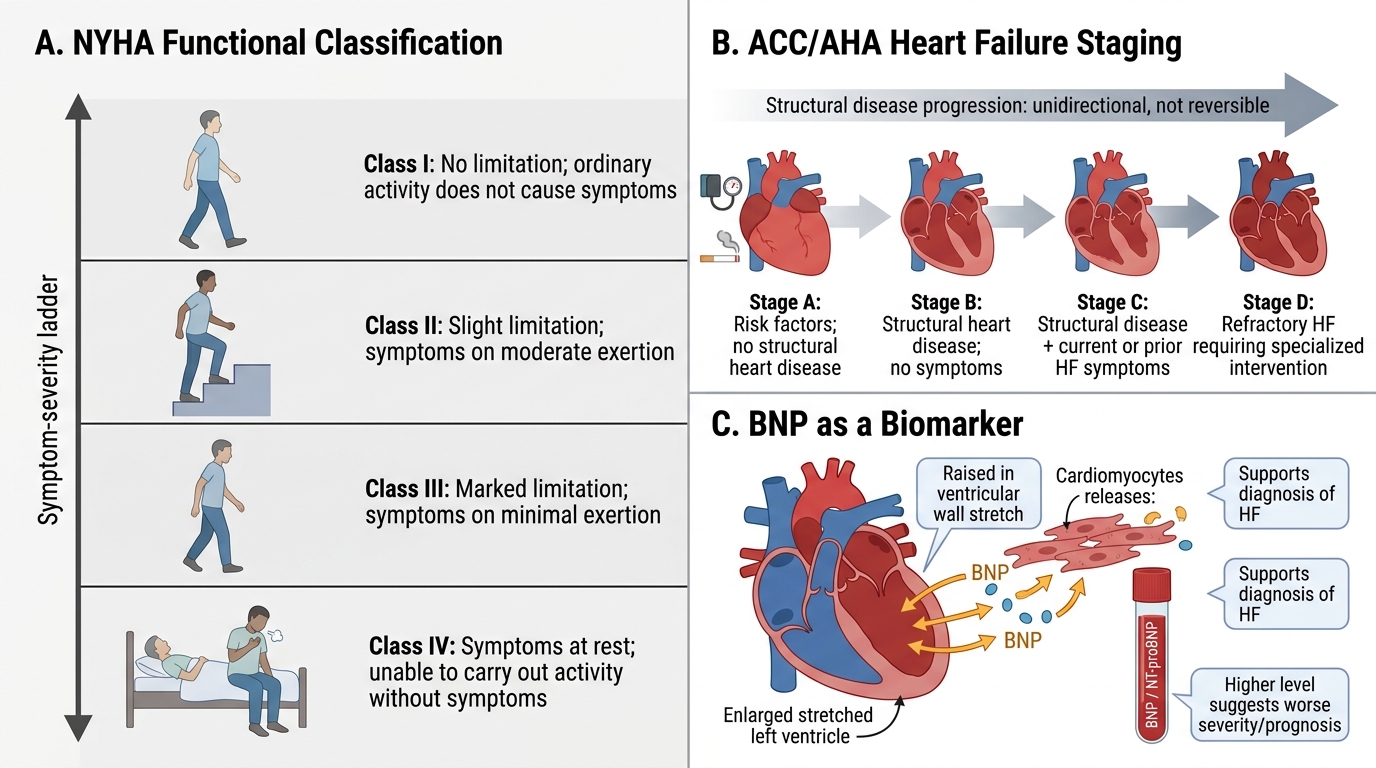
NYHA Functional Classification (symptoms-based):
| Class | Description |
|---|---|
| I | No limitation; ordinary activity does not cause symptoms |
| II | Slight limitation; comfortable at rest; symptoms on moderate exertion |
| III | Marked limitation; comfortable at rest; symptoms on minimal exertion |
| IV | Unable to carry out any activity without symptoms; symptoms at rest |
ACC/AHA Staging (structural disease progression — unidirectional, not reversible):
| Stage | Description |
|---|---|
| A | Risk factors present; no structural heart disease |
| B | Structural heart disease; no symptoms |
| C | Structural disease + current or prior HF symptoms |
| D | Refractory HF requiring advanced intervention (LVAD, transplant) |
Note: A patient can remain at Stage C while fluctuating between NYHA Class II and IV. Stages A/B represent the preventable window.
Brain Natriuretic Peptide (BNP):
BNP (and its cleavage product, NT-proBNP) is synthesised and secreted by ventricular cardiomyocytes in response to wall stretch and increased filling pressure. It acts as an endogenous counter-regulator: promotes natriuresis, vasodilation, and inhibits RAAS — but is insufficient at advanced stages.
Clinical utility:
- BNP < 100 pg/mL: HF very unlikely in a patient presenting with dyspnoea (high negative predictive value).
- BNP > 400 pg/mL: HF highly likely.
- Serial BNP guides treatment intensity — falling BNP with treatment correlates with improved prognosis.
- Elevated in: any cause of ventricular wall stress (PE, severe hypertension, CKD — the latter reduces clearance).
SELF-CHECK
A 65-year-old man with ischaemic cardiomyopathy has NYHA Class III symptoms. He is admitted with decompensation and a new stroke due to systemic embolism. Which mechanism BEST explains the embolic stroke?
A. Paradoxical embolism through a patent foramen ovale
B. Mural thrombus in a poorly contractile, dilated left ventricle
C. Right ventricular thrombus dislodging into the pulmonary circulation
D. Atherosclerotic plaque rupture in the carotid artery
Reveal Answer
Answer: B. Mural thrombus in a poorly contractile, dilated left ventricle
In dilated, hypokinetic left ventricles — characteristic of ischaemic cardiomyopathy — stasis of blood promotes mural thrombus formation on the endocardial surface, particularly at the apex. Fragments can embolise systemically causing stroke, mesenteric ischaemia, or limb ischaemia. This is a direct complication of impaired LV systolic function. RV thrombus would embolise to the pulmonary circulation (not systemic), and carotid atherosclerosis is a separate pathology.
Integrated Summary: Left vs Right Heart Failure at a Glance
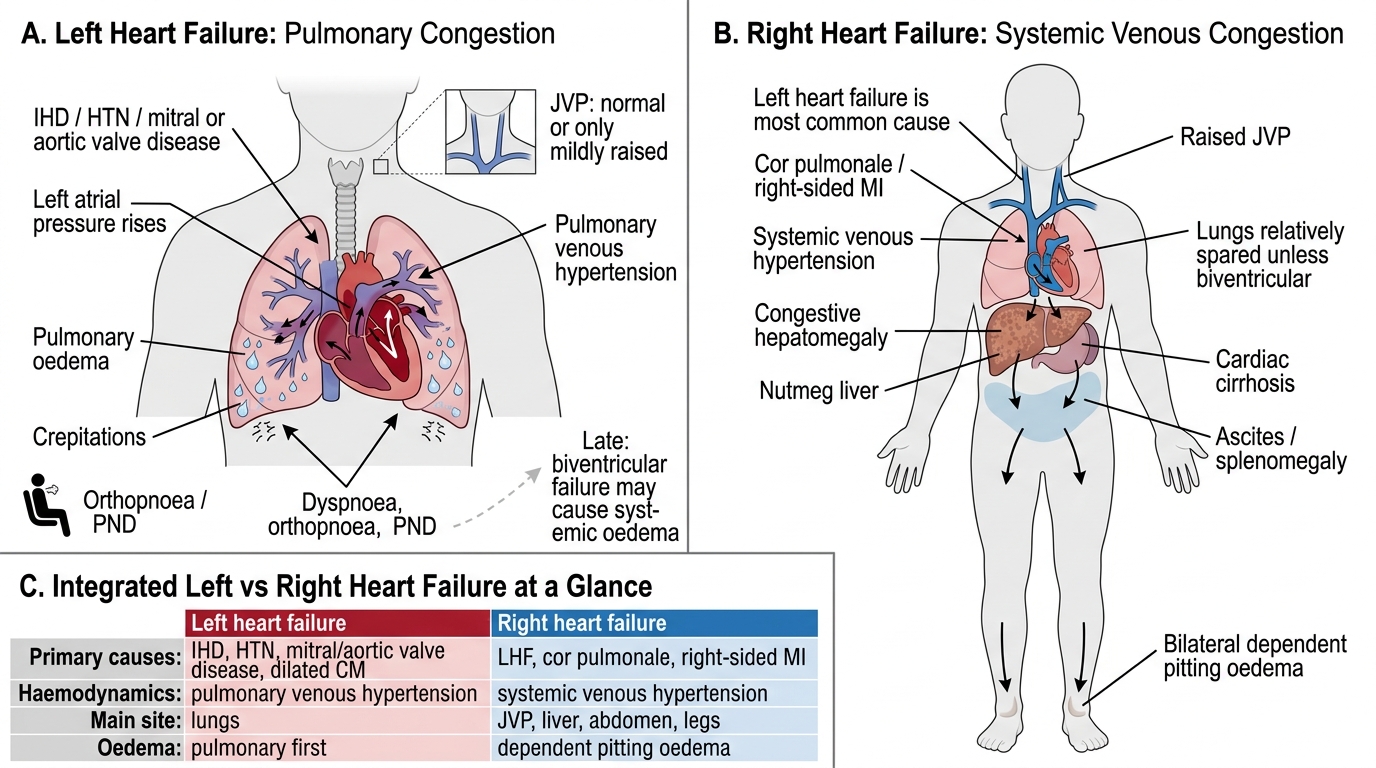
Left vs Right Heart Failure at a Glance
| Feature | Left Heart Failure | Right Heart Failure |
|---|---|---|
| Primary cause | IHD, HTN, mitral/aortic valve disease, dilated CM | LHF (most common), cor pulmonale, right-sided MI |
| Haemodynamic effect | Pulmonary venous hypertension | Systemic venous hypertension |
| Lungs | Pulmonary oedema (orthopnoea, PND, crepitations) | Relatively spared (unless also left-sided) |
| Liver | Normal or mildly congested | Congestive hepatomegaly, nutmeg liver, cardiac cirrhosis |
| JVP | Normal or mildly raised | Markedly raised |
| Oedema | Pulmonary (+ later systemic if biventricular) | Bilateral dependent pitting oedema |
| Ascites/splenomegaly | Absent unless biventricular | Present in significant RHF |
| Characteristic cell | Heart failure cells (alveolar siderophages) | Centrilobular hepatocyte necrosis |
| BNP | Elevated | Elevated (both ventricles can release BNP) |
When both ventricles fail — congestive heart failure (CHF) — all of the above features coexist. In clinical practice, biventricular failure is far more common than pure left- or right-sided failure in late disease.