Page 12 of 34
PA26.3 | Heart Failure — SDL Guide (Part 2)
Left Heart Failure — Causes and Pulmonary Consequences
Left Heart Failure: Pulmonary Consequences
Left heart failure (LHF) results from failure of the left ventricle to eject blood adequately forward into the systemic circulation or from failure of the left atrium (e.g. mitral stenosis) to empty into the LV.
Common causes: ischaemic heart disease (IHD — infarction or ischaemic cardiomyopathy), systemic hypertension, aortic and mitral valve disease, dilated cardiomyopathy, myocarditis.
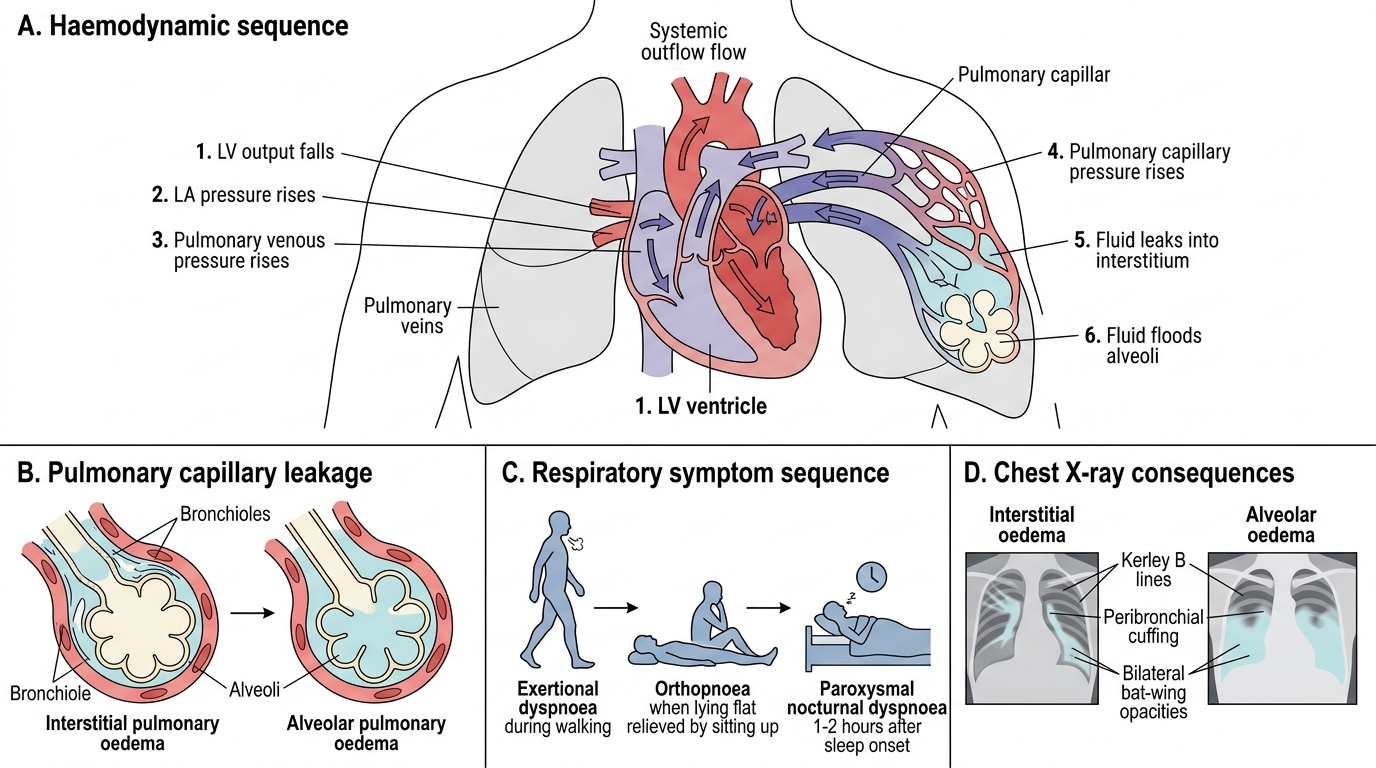
Haemodynamic sequence:
1. LV output falls → LA pressure rises → pulmonary venous pressure rises → pulmonary capillary pressure rises.
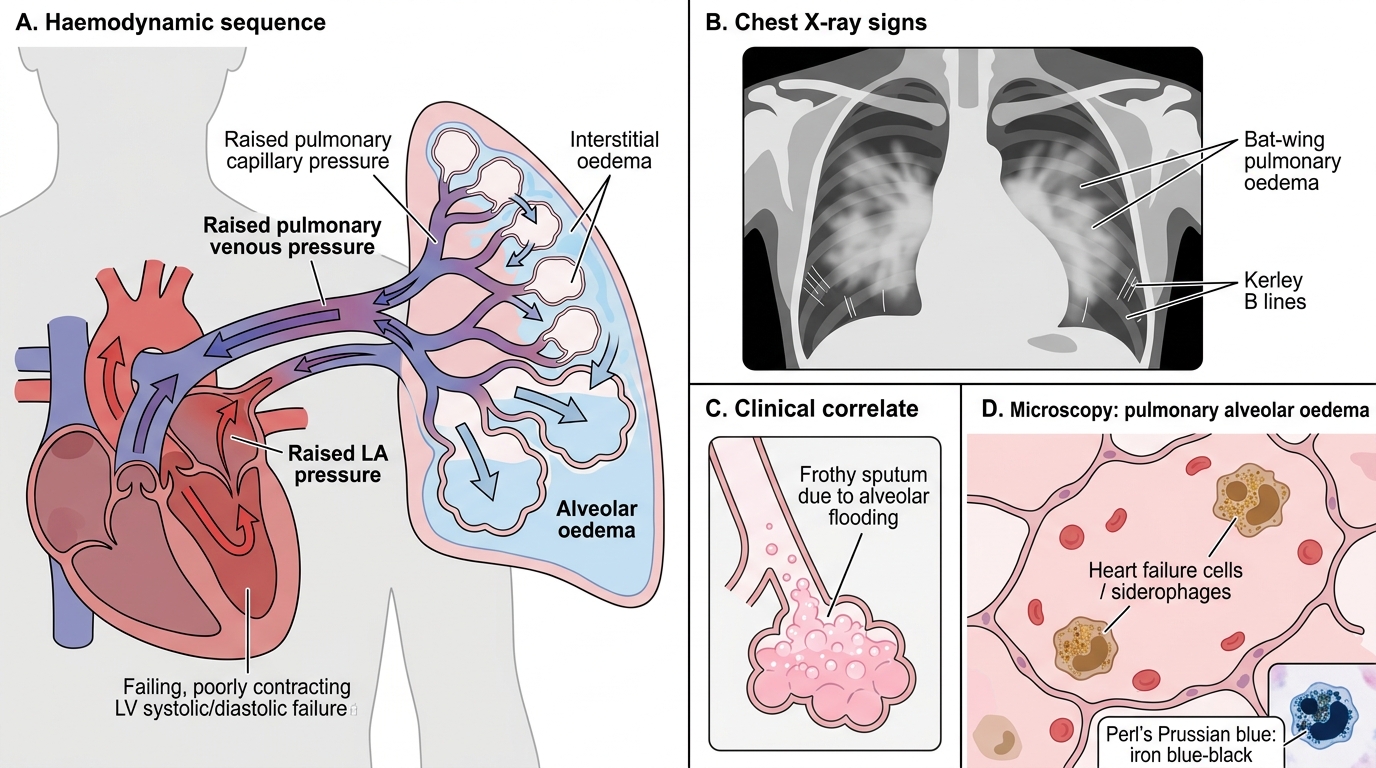
2. When pulmonary capillary pressure exceeds plasma oncotic pressure (~25 mmHg), fluid transudates into interstitial spaces → interstitial pulmonary oedema (peribronchial cuffing, Kerley B lines on CXR).
3. Further rise → alveolar flooding → alveolar pulmonary oedema (frothy pink sputum, fine crepitations, bat-wing opacification on CXR).
Respiratory symptoms follow this sequence: exertional dyspnoea → orthopnoea (dyspnoea on lying flat, relieved by sitting up — because supine posture redistributes fluid from legs to pulmonary circulation) → paroxysmal nocturnal dyspnoea (PND) (sudden nocturnal breathlessness, 1-2 hours after sleep onset, as fluid shifts centrally).
Left Heart Failure: Haemodynamic Sequence to Pulmonary Oedema
"Heart failure cells" (siderophages): chronic pulmonary congestion leads to repeated small alveolar haemorrhages. Alveolar macrophages phagocytose the extravasated red cells and accumulate haemosiderin (iron pigment from Hb breakdown). These haemosiderin-laden macrophages are pathognomonic of chronic passive pulmonary congestion. They are demonstrated by Perl's Prussian blue stain, which colours the iron blue-black.
Reduced forward output → hypoperfusion of kidneys (pre-renal oliguria), brain (confusion in acute decompensation), and skeletal muscle (fatigue, weakness).
CLINICAL PEARL
Orthopnoea vs PND — why the difference?
Both result from fluid redistribution when the patient lies down, but the timing differs. Orthopnoea occurs immediately on lying down because gravity instantly redistributes interstitial oedema. PND occurs 1-2 hours after sleep onset because fluid redistribution from the legs is gradual — it takes time for the dependent oedema of the legs (accumulated over the day) to mobilise into the pulmonary circulation. Clinically, you elicit orthopnoea by asking "how many pillows do you sleep on?" — each extra pillow is a clinical step of worsening LHF.
SELF-CHECK
Sputum examination of a patient with chronic left heart failure reveals macrophages laden with brown-yellow granular pigment that stains blue with Perl's Prussian blue stain. These cells are called:
A. Foam cells (lipid-laden macrophages)
B. Heart failure cells (siderophages)
C. Dust cells (carbon-laden macrophages)
D. Erythrophages
Reveal Answer
Answer: B. Heart failure cells (siderophages)
Heart failure cells (siderophages) are alveolar macrophages that have ingested haemosiderin derived from the breakdown of extravasated red blood cells in chronically congested alveoli. Perl's Prussian blue stain confirms the iron content (blue colour). They are pathognomonic of chronic passive pulmonary congestion. Foam cells contain lipid (Oil Red O positive); dust cells contain carbon (black pigment); erythrophages contain intact RBCs.
Right Heart Failure — Causes and Systemic Venous Consequences
Right Heart Failure: Causes and Systemic Venous Congestion
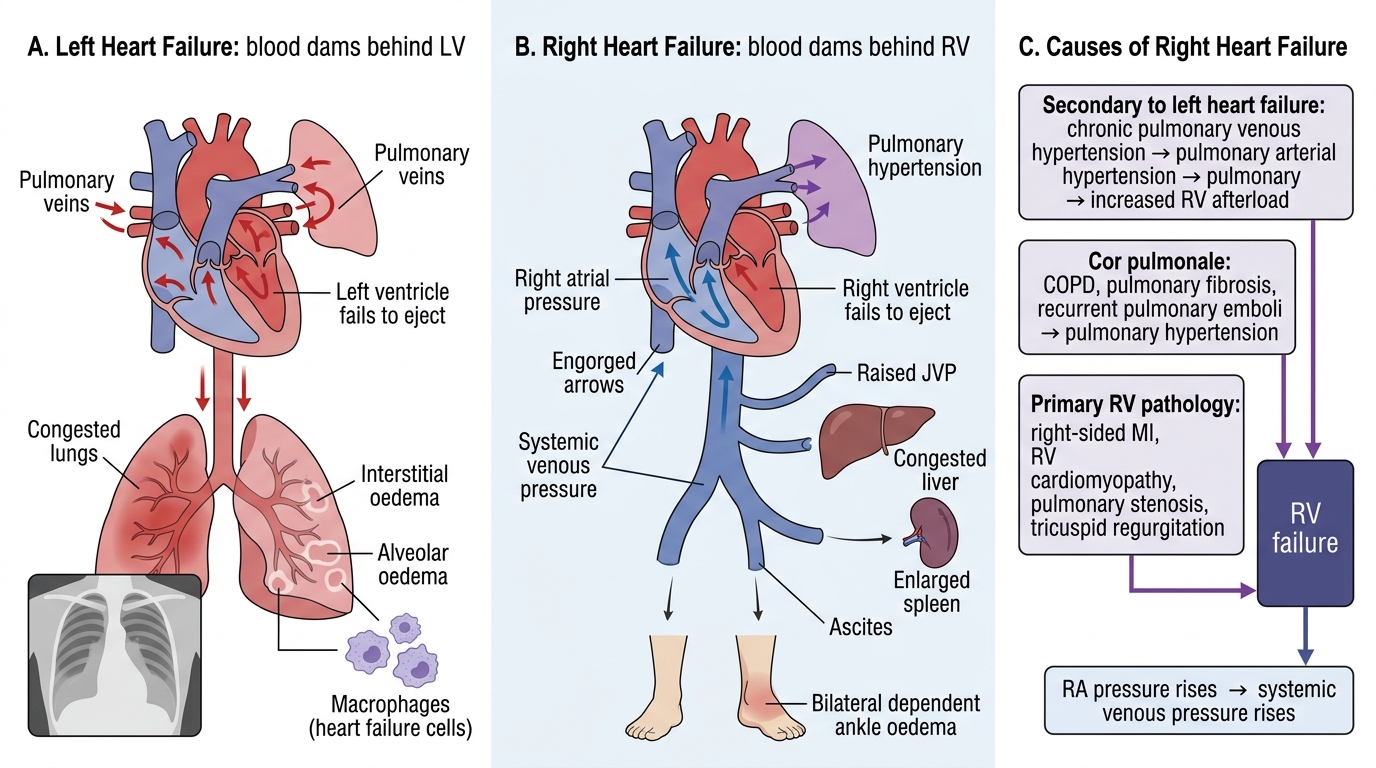
Right heart failure (RHF) results from failure of the right ventricle to eject blood into the pulmonary circulation.
Causes:
- Most commonly: secondary to left heart failure — chronic pulmonary venous hypertension raises pulmonary arterial pressure, increasing RV afterload until the RV fails.
- Cor pulmonale: RHF due to pulmonary hypertension from primary lung disease (COPD, pulmonary fibrosis, recurrent pulmonary emboli) — without LHF as the driver.
- Primary RV pathology: right-sided MI, RV cardiomyopathy, pulmonary stenosis, tricuspid regurgitation.
Haemodynamic consequence: RV fails → RA pressure rises → systemic venous pressure rises → engorgement of all systemic veins and viscera.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Left Versus Right Heart Failure: Congestion Patterns
Clinical and pathological findings:
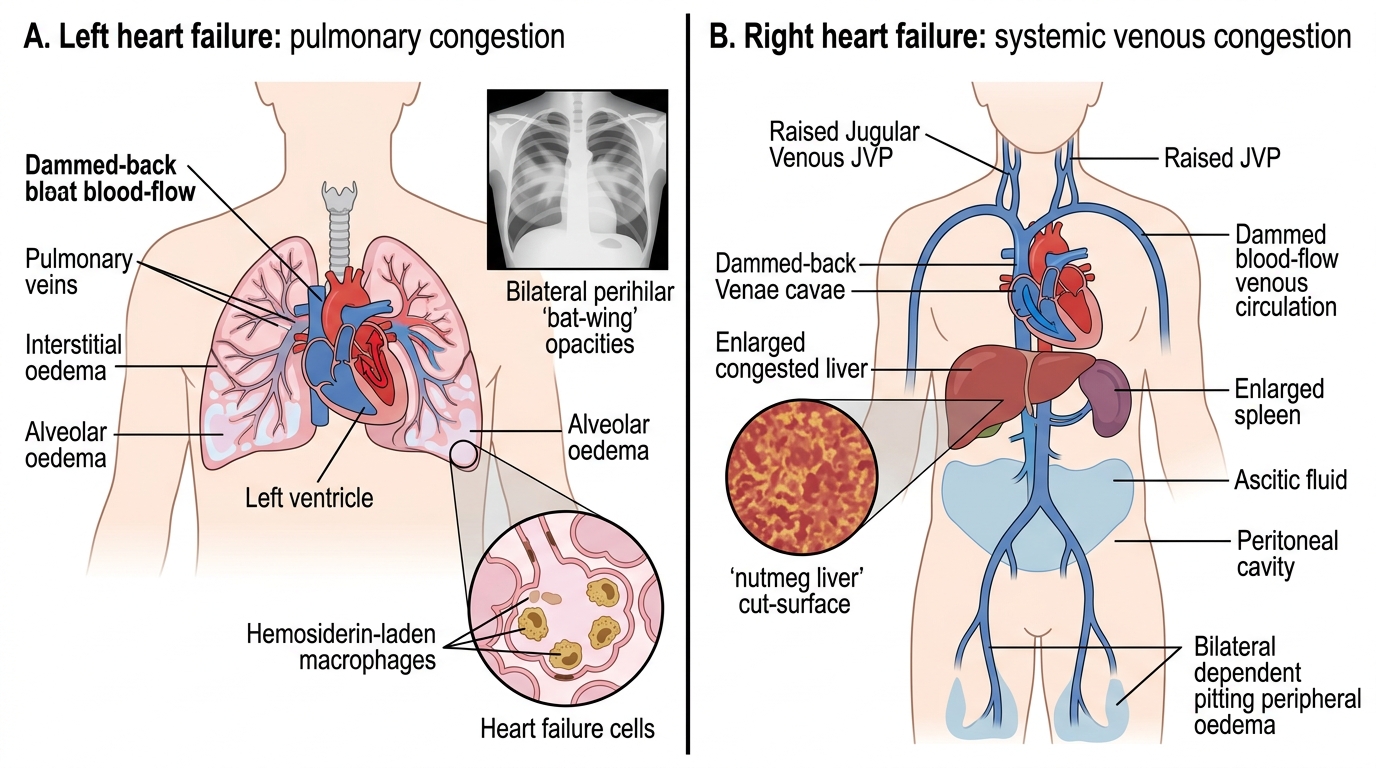
- Raised jugular venous pressure (JVP): the internal jugular vein acts as a manometer of right atrial pressure. JVP > 4 cm above sternal angle is abnormal.
- Dependent pitting oedema: gravity-dependent accumulation of transudated fluid in subcutaneous tissues. Bilateral ankle and leg oedema in ambulant patients; sacral oedema in bed-bound patients. Non-pitting oedema suggests lymphoedema — a different diagnosis.
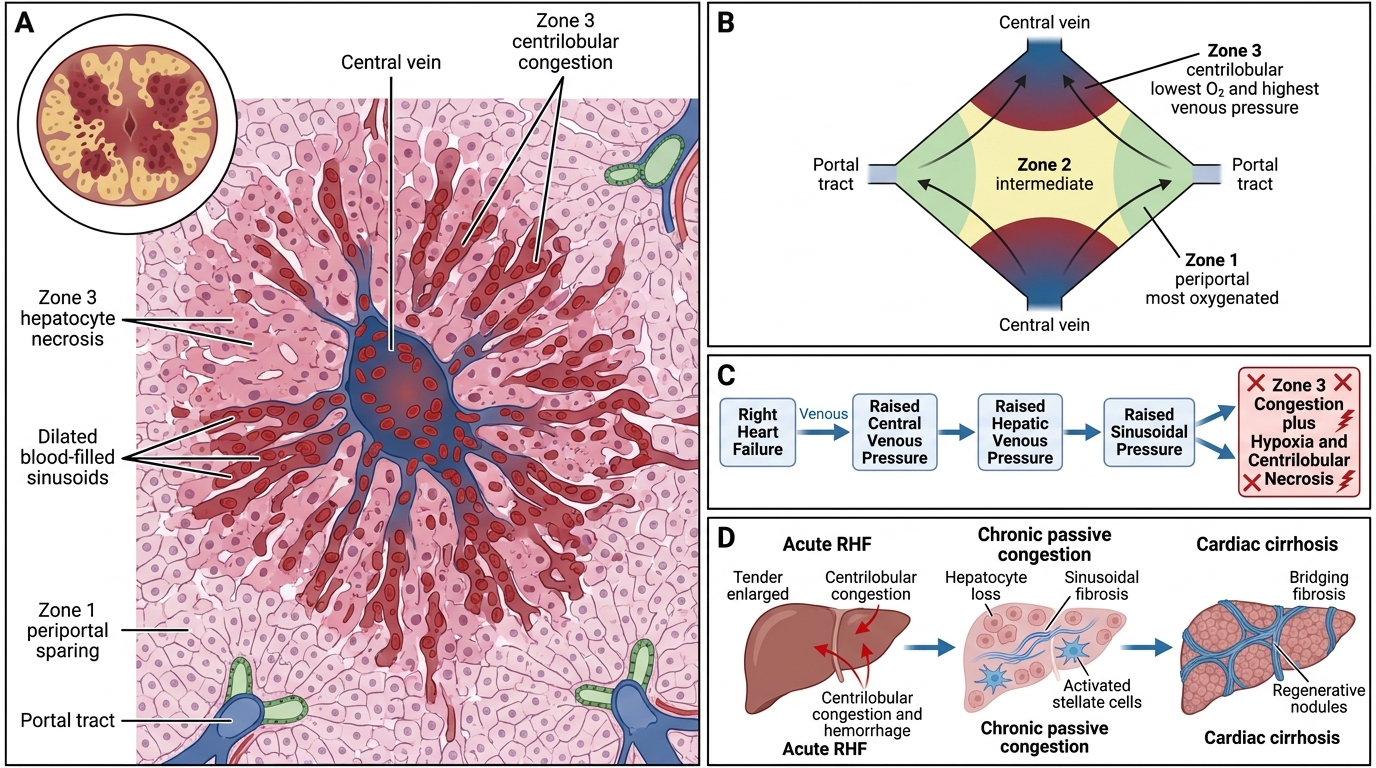
- Congestive hepatomegaly ("nutmeg liver"): hepatic venous outflow is obstructed by raised central venous pressure → sinusoidal distension in the centrilobular (perivenular) zone → centrilobular congestion and haemorrhage → centrilobular hepatocyte necrosis (congestion necrosis). Macroscopically, the cut surface shows a mottled red-and-yellow pattern resembling a nutmeg — hence "nutmeg liver." Microscopically: dilated, congested centrilobular sinusoids surrounded by necrotic hepatocytes, with preserved or fatty periportal hepatocytes. Chronic severe congestion → cardiac cirrhosis (centrilobular fibrosis).
- Ascites: transudation into the peritoneal cavity from elevated portal venous and hepatic sinusoidal pressure. SAAG ≥ 1.1 g/dL confirms portal hypertension aetiology.
- Splenomegaly: passive congestion of splenic sinusoids → firm, enlarged spleen ("congestive splenomegaly").
- Peripheral cyanosis: reduced cardiac output → increased O₂ extraction → more deoxyhaemoglobin in peripheral blood.
Nutmeg Liver and Cardiac Cirrhosis — Pathological Detail
Nutmeg Liver and Cardiac Cirrhosis
The liver deserves particular attention as it uniquely shows the progression of passive venous congestion to structural damage.
Zones of the hepatic acinus (Rappaport):
- Zone 1 (periportal) = closest to hepatic artery, most oxygenated, most resistant to ischaemia.
- Zone 3 (centrilobular / perivenular) = farthest from hepatic artery, most dependent on venous drainage, first to suffer from venous outflow obstruction.
In right heart failure, raised central venous pressure directly raises hepatic venous and then sinusoidal pressure. Zone 3 (centrilobular) hepatocytes are simultaneously congested and hypoxic (lowest O₂ tension, highest venous pressure). This dual insult explains the selectivity of centrilobular necrosis.
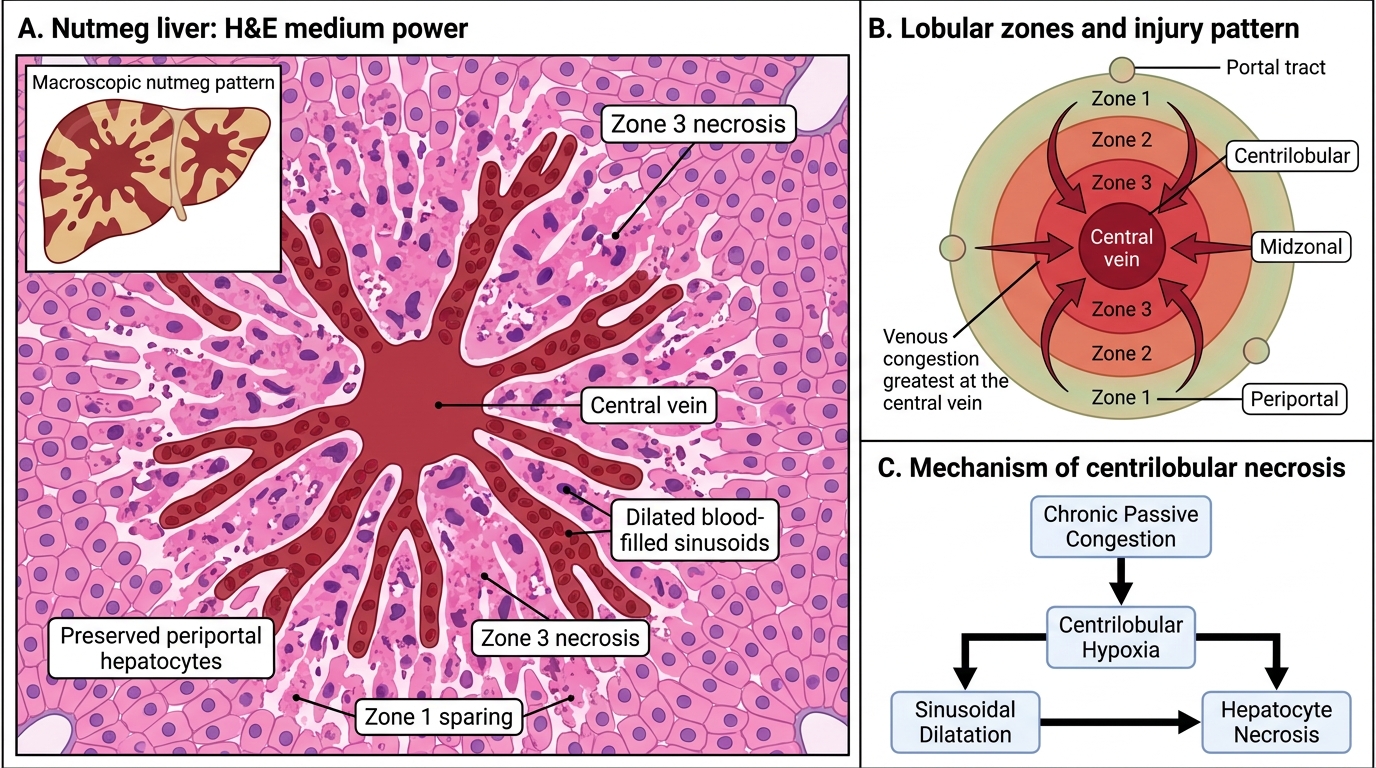
Nutmeg Liver: Centrilobular Congestion and Necrosis
Progression:
- Acute RHF: centrilobular congestion and haemorrhage → acute liver distension and tenderness ("hepatic angina").
- Subacute/chronic: centrilobular hepatocyte loss, sinusoidal fibrosis, stellate cell activation.
- Cardiac cirrhosis: bridging fibrosis from centrilobular zone to central vein in adjacent lobules — produces the classic "reverse lobulation" pattern unique to cardiac cirrhosis (periportal parenchyma is preserved as "islands").
Clinical marker: ALT/AST transiently elevated in acute decompensated HF ("shock liver" or cardiogenic hepatopathy). Chronic CHF → mildly raised bilirubin, prolonged PT, reduced synthetic function.
SELF-CHECK
In the "nutmeg liver" of chronic right heart failure, which zone of the hepatic acinus shows the most prominent necrosis and congestion, and why?
A. Zone 1 (periportal) — because it receives all portal blood first
B. Zone 2 (midzonal) — because it is equidistant from both oxygen sources
C. Zone 3 (centrilobular) — because it has the lowest oxygen tension and drains directly into the hepatic vein
D. Zone 3 (centrilobular) — because it receives the most hepatic arterial blood
Reveal Answer
Answer: C. Zone 3 (centrilobular) — because it has the lowest oxygen tension and drains directly into the hepatic vein
Zone 3 (centrilobular / perivenular zone) has the lowest oxygen tension (being farthest from the hepatic artery) and its sinusoids drain directly into the central (hepatic) vein. In right heart failure, raised hepatic venous pressure obstructs outflow here first, causing combined congestion and ischaemia — dual insult → centrilobular necrosis. Zone 1 is most oxygenated and most resistant. Option D is wrong — the hepatic artery preferentially perfuses zone 1.