Page 6 of 34
PA26.6 | Ischaemic Heart Disease & Acute Coronary Syndromes — SDL Guide
Learning Objectives
- Define IHD and describe the epidemiology and risk factors underlying coronary atherosclerosis
- Explain the pathophysiology of stable angina versus acute plaque change leading to the ACS spectrum
- Distinguish STEMI, NSTEMI, and unstable angina by mechanism, coronary occlusion pattern, and biomarker profile
- Describe the gross and microscopic evolution of myocardial infarction across its full timeline from 0 hours to 8 weeks
- Interpret cardiac biomarker kinetics (troponin I/T, CK-MB, myoglobin) in the clinical context of ACS
- List the major complications of myocardial infarction and their clinicopathological basis
- Identify key ECG changes and describe reperfusion injury including contraction band necrosis
INSTRUCTIONS
Cardiovascular disease kills more people worldwide than any other cause — and IHD is its dominant driver. For a Year-2 student, this module bridges the vascular pathology you studied in Cluster CV-1 (atherosclerosis) with the clinical emergency you will encounter in every hospital posting. Understanding the evolution of a myocardial infarct — hour by hour, cell by cell — is foundational for interpreting ECGs, interpreting troponin trends, and understanding why MI complications occur when they do. Work through each section sequentially; the micro_quiz blocks are placed immediately after high-yield concepts to reinforce retention.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 12 (Heart) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 16 (Cardiovascular System) (textbook)
- 2023 ESC Guidelines for the management of ACS (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old male construction worker collapses at a worksite. His colleagues describe crushing chest pain radiating to the left arm for 40 minutes before he lost consciousness. In the emergency room his troponin I is 18 ng/mL (reference < 0.04), ECG shows ST elevation in leads II, III, and aVF, and his BP is 80/50. The cardiologist calls a 'Code STEMI'.
Every minute of delay costs 1.9 million myocardial cells. By the time you finish this module, you will understand exactly what is happening at the molecular, cellular, and tissue level inside this patient's heart — and why each minute matters.
WHY THIS MATTERS
Ischaemic heart disease (IHD) is the single leading cause of death in India and globally, accounting for approximately 17% of all deaths. It is the pathological culmination of coronary atherosclerosis — a process that begins in the second decade of life and accelerates through adult risk factor exposure.
For your clinical postings, IHD is unavoidable: every ICU, every casualty, and every general medicine ward will present you with ACS, MI complications, and troponin trends. The NMC CBUC competency PA26.6 specifically requires you to interpret cardiac function tests in ACS — an examined competency in both theory papers and OSCE.
RECALL
Before proceeding, recall from Cluster CV-1:
- What is the sequence of events in atherosclerotic plaque formation (endothelial injury → foam cells → fibrous cap)?
- What are the major modifiable risk factors for atherosclerosis?
- What is the difference between stable and unstable plaque morphology?
- Recall the coronary arterial supply: which artery supplies the anterior wall? The inferior wall?
If any of these are uncertain, spend 5 minutes reviewing your CV-1 SDL before proceeding — this module builds directly on that foundation.
Definition and Epidemiology of IHD
Definition, Epidemiology, and Risk Factors of IHD
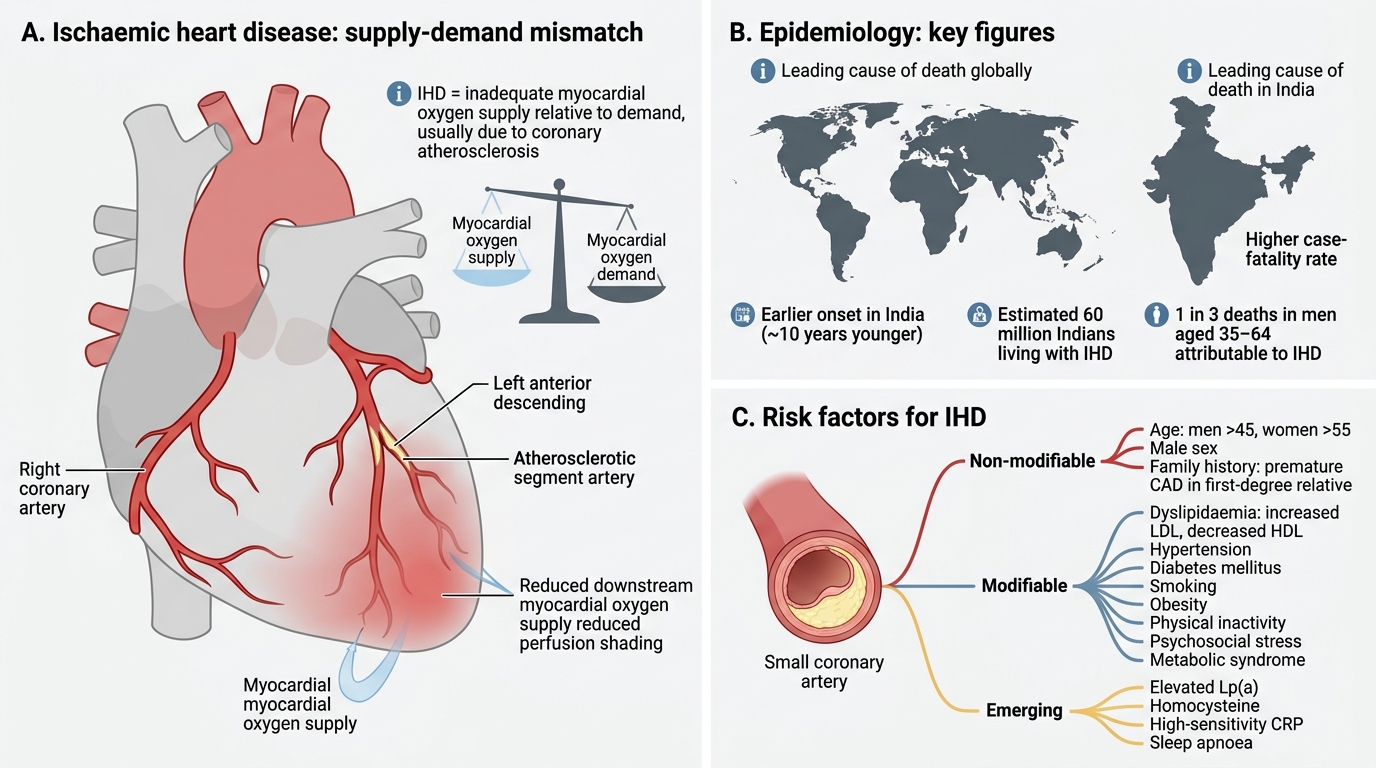
Ischaemic heart disease is a broad term for conditions in which the myocardial oxygen supply is inadequate relative to demand, almost always due to coronary artery disease (CAD) from atherosclerosis.
Epidemiology — key figures to remember:
• Leading cause of death globally (WHO 2023) and in India (GBD 2022)
• 1 in 3 deaths in men aged 35–64 are attributable to IHD
• India bears a disproportionate burden — earlier age of onset (~10 years younger than Western populations) and higher case-fatality rate
• Estimated 60 million Indians currently living with IHD
Risk factors (identical to atherosclerosis risk — this is not coincidental; IHD is atherosclerosis applied to coronaries):
Non-modifiable: age (men >45, women >55), male sex, family history (first-degree relative with premature CAD)
Modifiable: dyslipidaemia (↑LDL, ↓HDL), hypertension, diabetes mellitus, smoking, obesity, physical inactivity, psychosocial stress, metabolic syndrome
Emerging risk factors: elevated Lp(a), homocysteine, high-sensitivity CRP, sleep apnoea.
Pathophysiology: From Stable Plaque to ACS
From Stable Plaque to Acute Coronary Syndrome
Understanding IHD pathophysiology requires distinguishing two fundamentally different mechanisms:
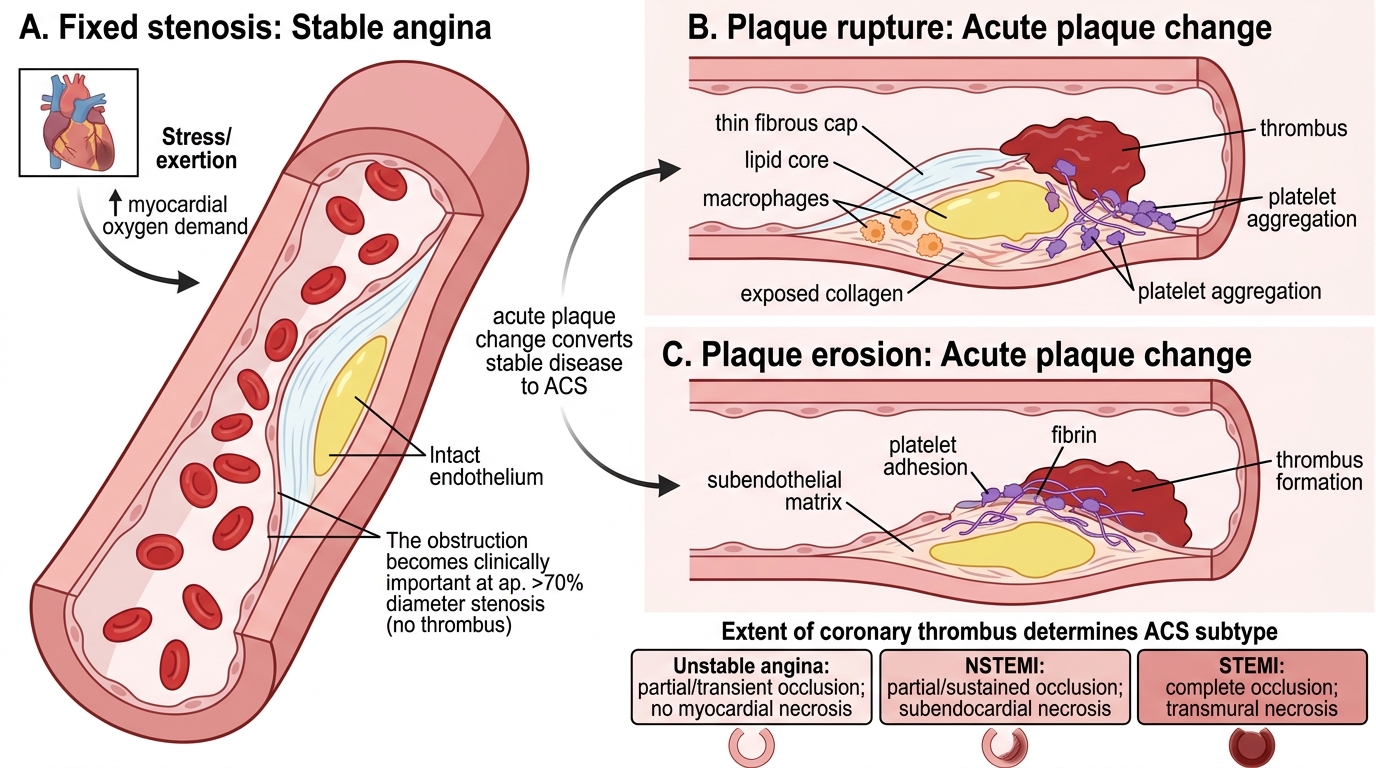
1. Fixed stenosis → Demand ischaemia (Stable Angina)
A stable atherosclerotic plaque with a thick fibrous cap progressively narrows the coronary lumen. When stenosis exceeds ~70% diameter, the fixed obstruction limits blood flow during exertion or stress. The result is stable angina — predictable, effort-induced chest pain that resolves with rest or nitrates. There is no thrombosis; the plaque is structurally intact.
2. Acute plaque change → Supply ischaemia (ACS)
Acute plaque change is the pivotal event that converts chronic stable disease into a life-threatening emergency. It has two main forms:
- Plaque rupture: A vulnerable plaque (thin fibrous cap, large lipid core, abundant macrophages) ruptures, exposing the thrombogenic subendothelial collagen and lipid core to flowing blood
- Plaque erosion: Endothelial cells overlying a plaque are lost without frank rupture; subendothelial matrix is exposed
Both mechanisms trigger the coagulation cascade and platelet aggregation → coronary thrombus.
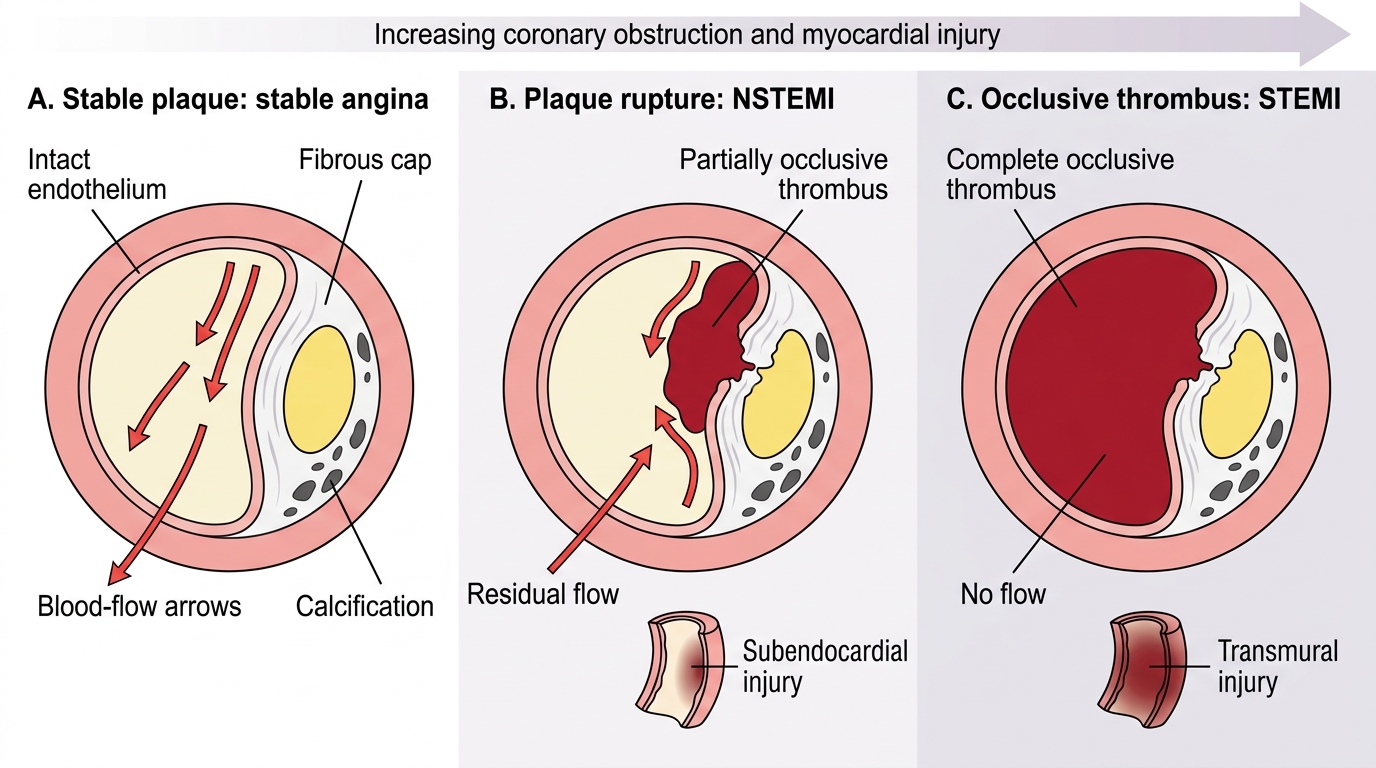
The extent of thrombus determines the ACS subtype:
| ACS Type | Occlusion | Myocardial Injury |
|---|---|---|
| Unstable Angina | Partial, transient | None (no necrosis) |
| NSTEMI | Partial, sustained | Subendocardial necrosis |
| STEMI | Complete, sustained | Transmural necrosis |
Vasospasm (Prinzmetal/variant angina) is a separate mechanism — transient severe spasm of a coronary artery, often at the site of a plaque, causing complete but reversible occlusion.
ACS Spectrum: Stable Plaque to STEMI
SELF-CHECK
A 62-year-old woman develops chest pain on climbing stairs that resolves within 5 minutes of rest. Coronary angiography shows 75% stenosis of the LAD with a smooth, calcified plaque and intact endothelium. No biomarker elevation. Which mechanism best explains her symptoms?
A. Plaque rupture with partial coronary thrombosis
B. Fixed stenosis causing demand ischaemia during exertion
C. Coronary vasospasm at the site of the plaque
D. Complete coronary occlusion with collateral supply
Reveal Answer
Answer: B. Fixed stenosis causing demand ischaemia during exertion
This is classic stable angina: a fixed high-grade stenosis limits flow only when myocardial oxygen demand increases (exertion), and symptoms resolve with rest when demand falls. Plaque rupture would produce ACS with biomarker elevation. Vasospasm is typically nocturnal and unpredictable. Complete occlusion without collaterals would cause infarction.
Coronary Territory Map and MI Localisation
Coronary Territories and MI Localisation
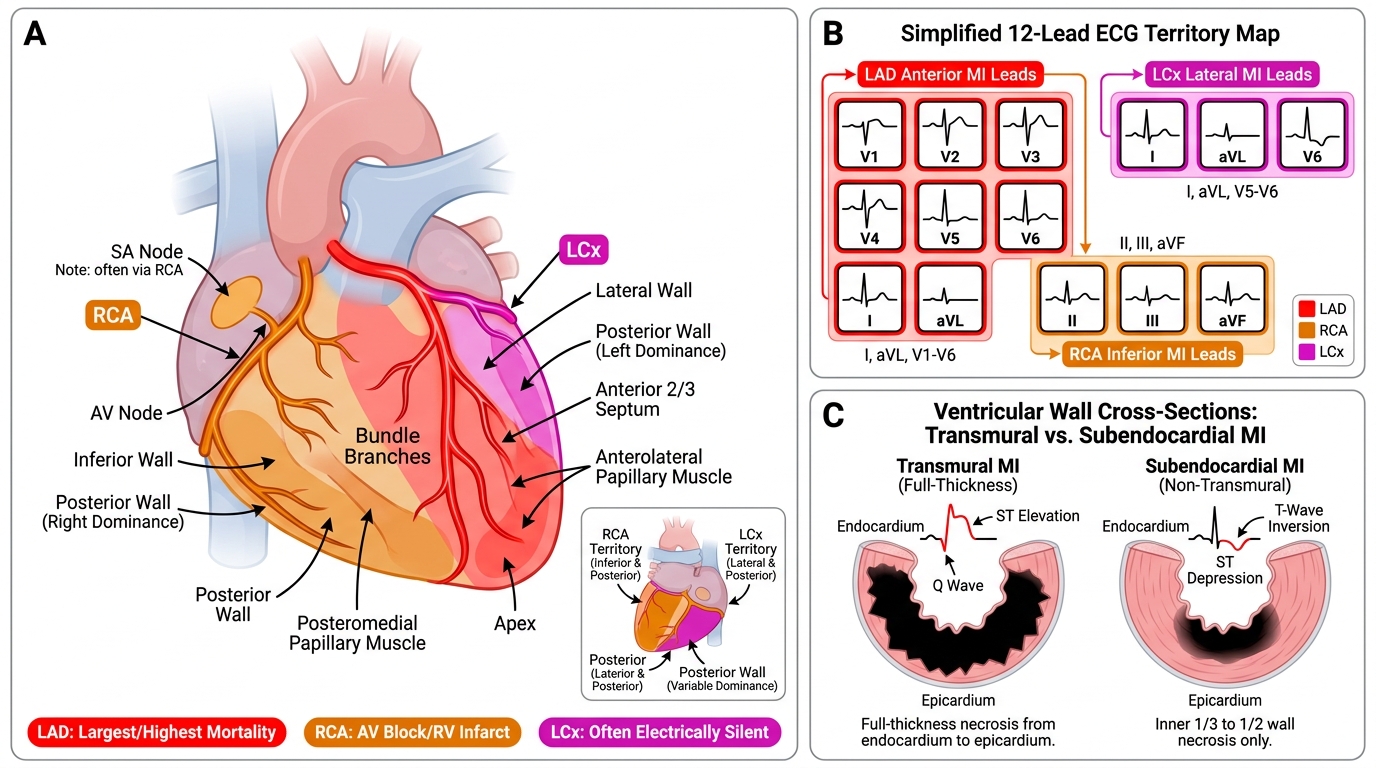
Knowing which coronary artery supplies which territory is essential for localising infarcts clinically:
Left Anterior Descending (LAD): Supplies the anterior wall and apex of the left ventricle, anterior two-thirds of the interventricular septum, anterolateral papillary muscle, and bundle branches. LAD occlusion produces anterior MI (ST elevation in leads I, aVL, V1–V6). LAD infarcts are typically the largest and carry the highest mortality.
Right Coronary Artery (RCA): Supplies the inferior wall and posterior wall (dominant in 80% of people), the posterior one-third of the septum, AV node (SA node in 60%), and the posteromedial papillary muscle. RCA occlusion produces inferior MI (ST elevation in II, III, aVF). RCA infarcts may present with AV conduction blocks and right ventricular infarction.
Left Circumflex (LCx): Supplies the lateral wall and, when dominant, the posterior wall. LCx occlusion produces lateral MI (ST elevation in I, aVL, V5–V6). LCx infarcts are often 'electrically silent' on standard ECG as leads for the lateral wall have lower sensitivity.
Transmural vs. Subendocardial MI:
- Transmural MI: Full-thickness necrosis across the ventricular wall; typically from complete coronary occlusion (STEMI). Associated with ST elevation and Q wave formation on ECG.
- Subendocardial MI: Necrosis confined to the inner one-third to one-half of the wall (the subendocardium is most vulnerable as it is furthest from epicardial coronaries and bears the highest wall tension). Associated with NSTEMI; no Q waves.
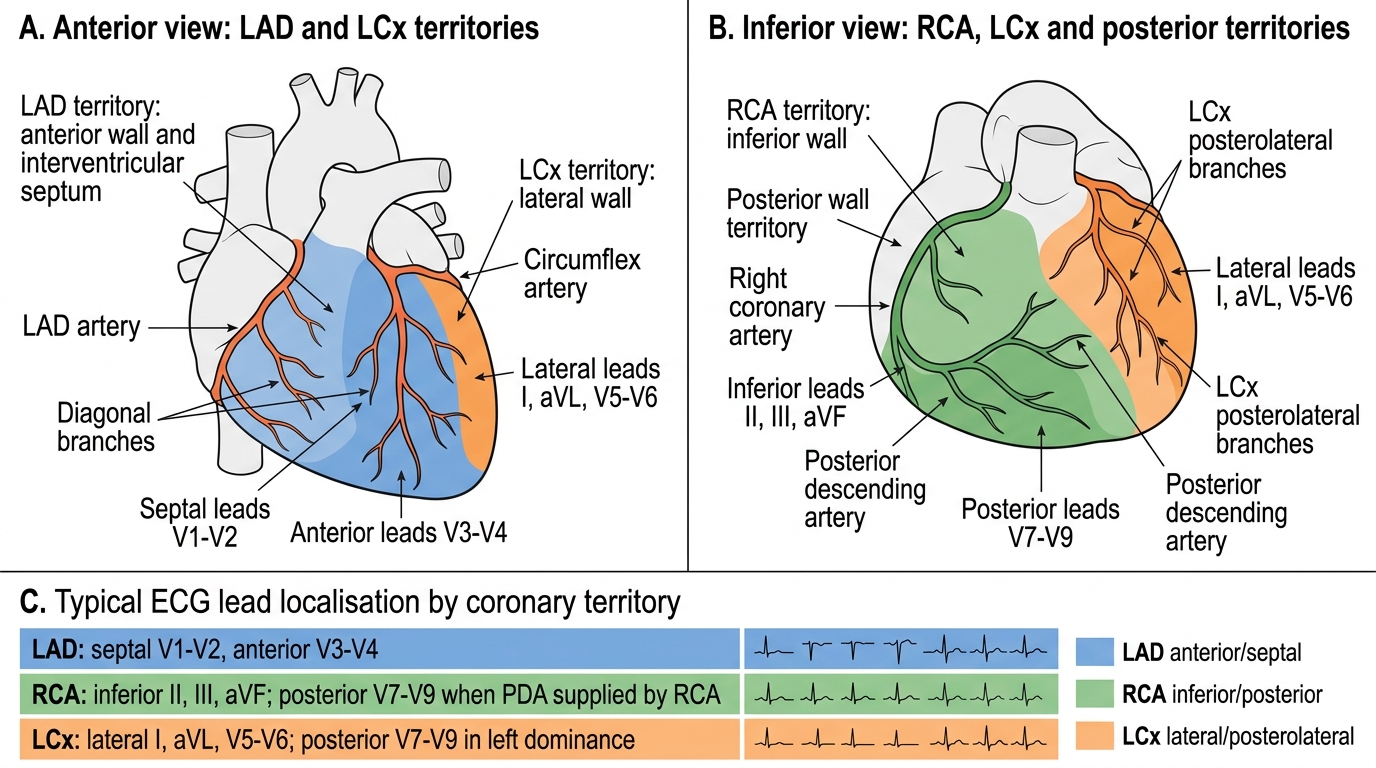
Coronary Artery Territories and ECG Lead Localisation