Page 9 of 34
PA26.6 | Ischaemic Heart Disease & Acute Coronary Syndromes — SDL Guide (Part 4)
Special Situations — Variant Angina and Sudden Cardiac Death
Variant Angina and Sudden Cardiac Death
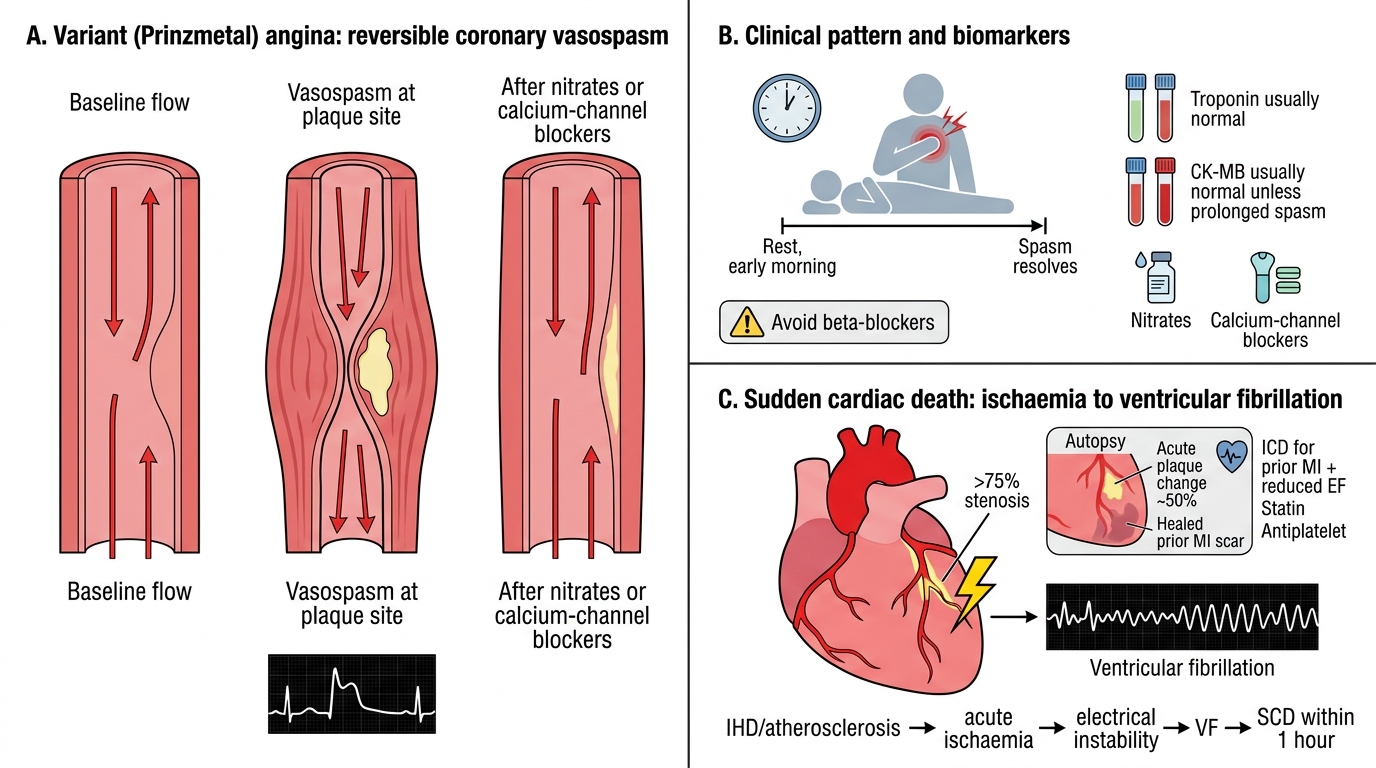
Variant (Prinzmetal) Angina:
Coronary vasospasm causes transient, severe reduction or complete cessation of coronary blood flow. Occurs at rest (often early morning), associated with transient ST elevation on ECG that resolves completely. Pathology: severe but reversible vasospasm, often at the site of an atheromatous plaque. Treated with calcium-channel blockers and nitrates; avoid beta-blockers. Troponin typically remains normal unless spasm is prolonged.
Sudden Cardiac Death (SCD):
- Defined as unexpected death within 1 hour of symptom onset, from a cardiac cause
- IHD (atherosclerosis ± acute plaque change) accounts for >80% in adults
- Mechanism: ventricular fibrillation triggered by ischaemia-induced electrical instability
- Pathological finding at autopsy: >75% stenosis in at least one major coronary artery; acute plaque change in ~50%; healed prior MI scars common
- Prevention: implantable cardioverter-defibrillators (ICDs) in patients with prior MI and reduced EF; statins/antiplatelets for secondary prevention
SELF-CHECK
A 48-year-old male smoker with no prior cardiac history is found to have the following test results 6 hours after onset of severe chest pain: Troponin I = 0.02 ng/mL (ref <0.04), CK-MB = 4 U/L (ref <25), ECG shows 1 mm ST depression in leads V4–V6. He is admitted and troponin is repeated at 3 hours: Troponin I = 0.18 ng/mL. What is the MOST LIKELY diagnosis?
A. Unstable angina — troponin is still below the diagnostic threshold
B. STEMI — ST changes confirm complete coronary occlusion
C. NSTEMI — rising troponin (delta) with ischaemic ECG changes but no ST elevation
D. Stable angina with demand ischaemia
Reveal Answer
Answer: C. NSTEMI — rising troponin (delta) with ischaemic ECG changes but no ST elevation
NSTEMI = ACS + rising troponin (the 'delta' — a rise from 0.02 to 0.18 ng/mL over 3h clearly crosses the diagnostic threshold) + ischaemic ECG changes (ST depression V4–V6) WITHOUT ST elevation. Unstable angina would show no troponin rise. STEMI requires ST elevation. Stable angina produces no biomarker change and symptoms only with exertion.
High-Yield Summary Table
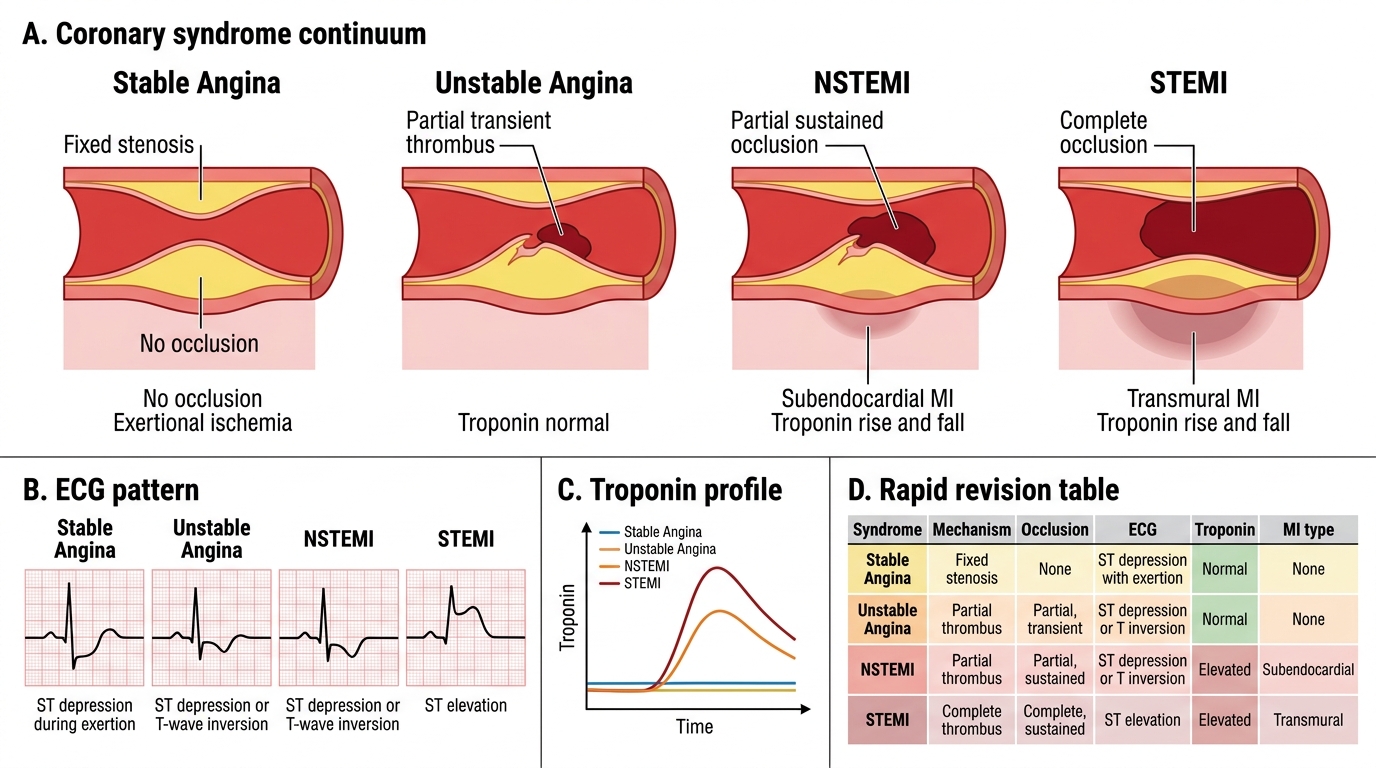
Acute Coronary Syndrome High-Yield Summary
Use this table for rapid revision:
| Syndrome | Mechanism | Occlusion | ECG | Troponin | MI type |
|---|---|---|---|---|---|
| Stable Angina | Fixed stenosis | None | ST↓ (exertion) | Normal | None |
| Unstable Angina | Partial thrombus | Partial, transient | ST↓/T↓ | Normal | None |
| NSTEMI | Partial, sustained | Partial, sustained | ST↓/T↓ | ↑↑ (rise+fall) | Subendocardial |
| STEMI | Complete occlusion | Complete | ST↑, Q waves | ↑↑↑ | Transmural |
| Variant Angina | Vasospasm | Transient complete | Transient ST↑ | Usually normal | None (unless prolonged) |
MI evolution timeline (must memorise):
• 0–12h: normal light microscopy / wavy fibres
• 12–24h: coagulative necrosis + contraction bands
• 1–3d: neutrophils (PMN peak)
• 3–7d: macrophages + phagocytosis
• 1–2wk: granulation tissue
• >2wk–2mo: dense collagen scar
Biomarker rule-of-thumb: Myoglobin rises first (1–3h), CK-MB peaks and returns fastest (48–72h, useful for reinfarction), Troponin is most sensitive/specific and stays longest (TnT up to 14d).