Page 8 of 34
PA26.6 | Ischaemic Heart Disease & Acute Coronary Syndromes — SDL Guide (Part 3)
Clinical Syndromes of IHD
Clinical Syndromes of Ischaemic Heart Disease
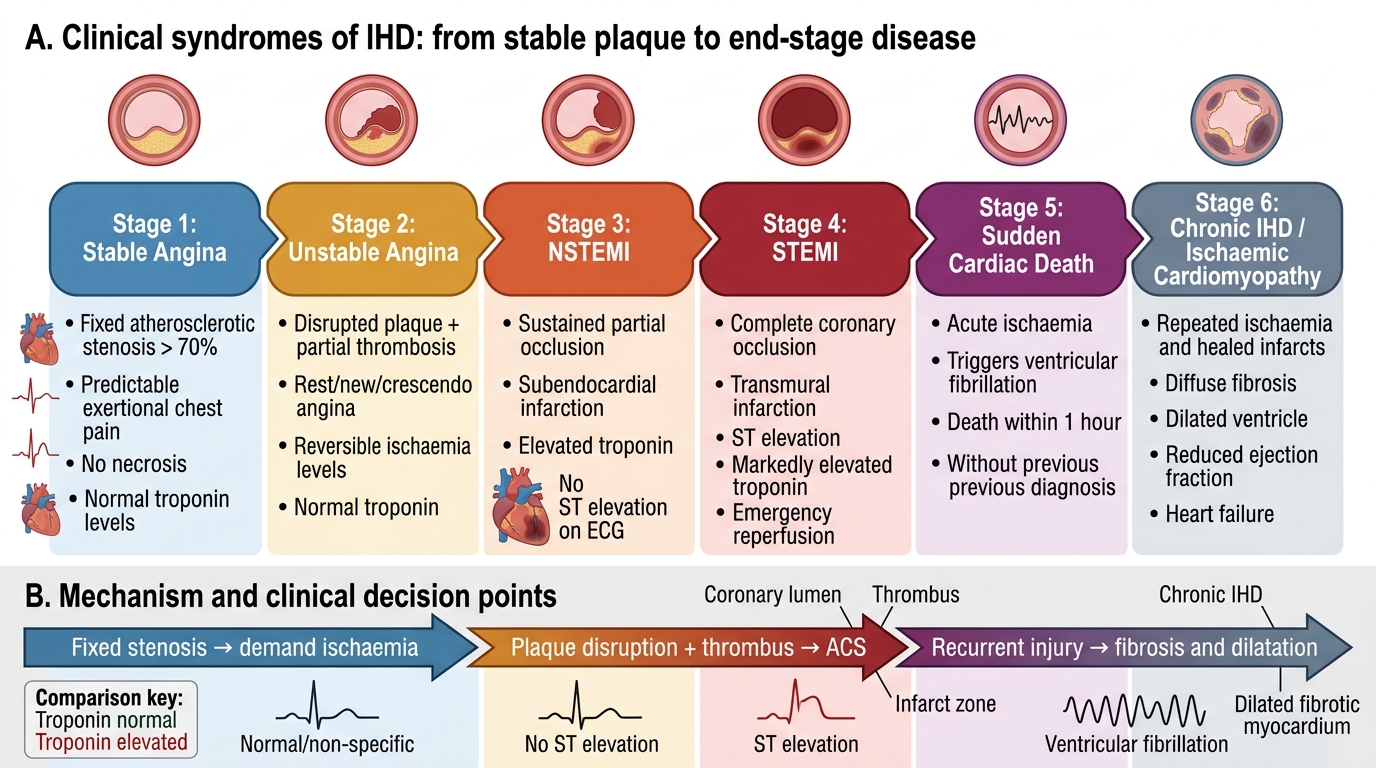
IHD presents across a spectrum of clinical syndromes:
1. Stable Angina
Predictable exertional chest pain; fixed stenosis >70%; no myocardial necrosis; troponin normal.
2. Unstable Angina (UA)
ACS without myocardial necrosis — rest pain, new-onset angina, or crescendo (worsening) angina. Biomarkers NORMAL. Mechanism: partial thrombosis on disrupted plaque causing transient or severe but reversible ischaemia.
3. NSTEMI
ACS with myocardial necrosis (elevated troponin) but NO ST elevation on ECG. Mechanism: sustained partial occlusion → subendocardial infarction. UA and NSTEMI share the same acute management pathway (anticoagulation + antiplatelet ± early PCI).
4. STEMI
ACS with complete coronary occlusion → transmural MI. ST elevation on ECG; troponin markedly elevated. Emergency reperfusion (primary PCI preferred, thrombolysis if PCI unavailable) is the standard of care.
5. Sudden Cardiac Death (SCD)
Death within 1 hour of symptoms. Mechanism: fatal arrhythmia (ventricular fibrillation) triggered by acute ischaemia, often in a patient with no prior diagnosis. IHD is the underlying cause in >80% of SCDs in adults >35 years.
6. Chronic IHD / Ischaemic Cardiomyopathy
Recurrent ischaemia, multiple healed infarcts, or chronically hibernating myocardium → diffuse myocardial fibrosis → dilated ischaemic cardiomyopathy with reduced ejection fraction and heart failure. This is the end-stage of IHD and a leading indication for cardiac transplantation.
Complications of Myocardial Infarction
Complications of Myocardial Infarction
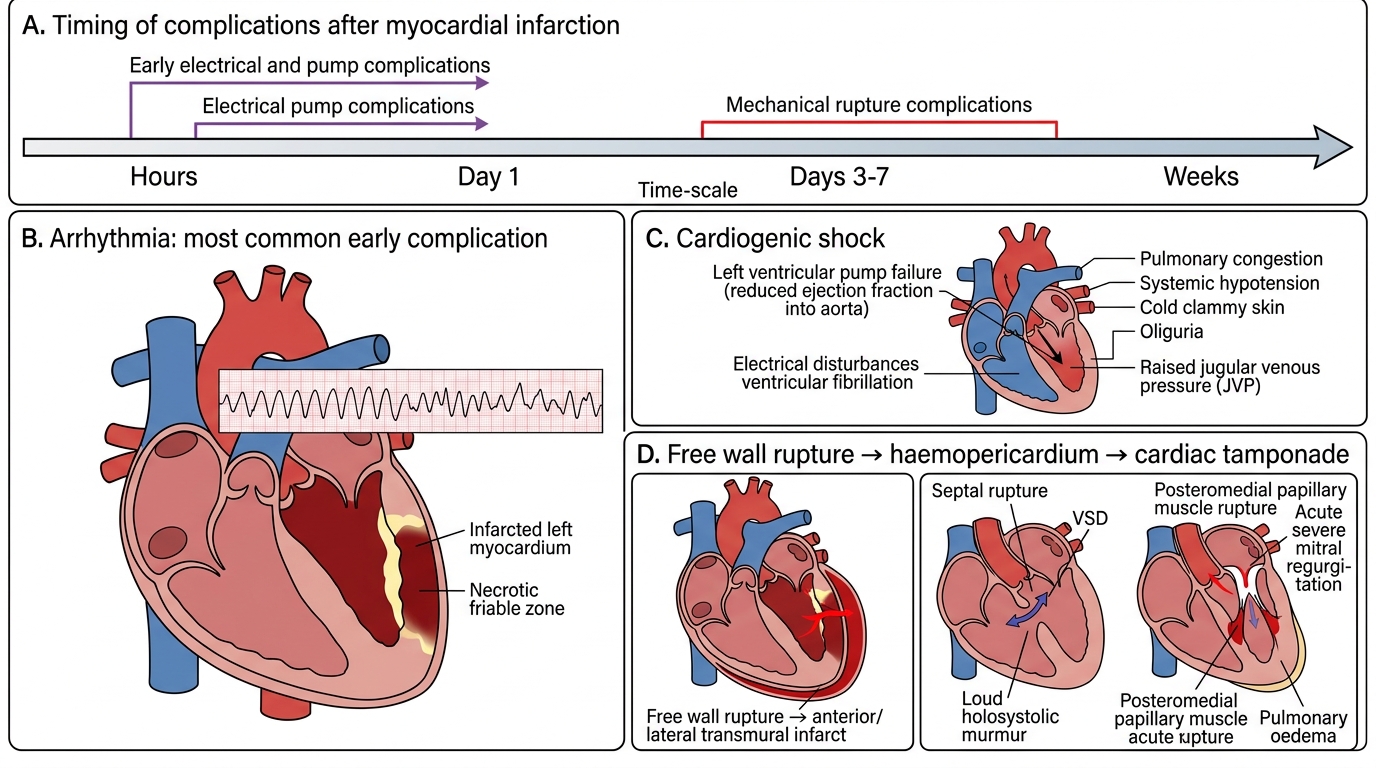
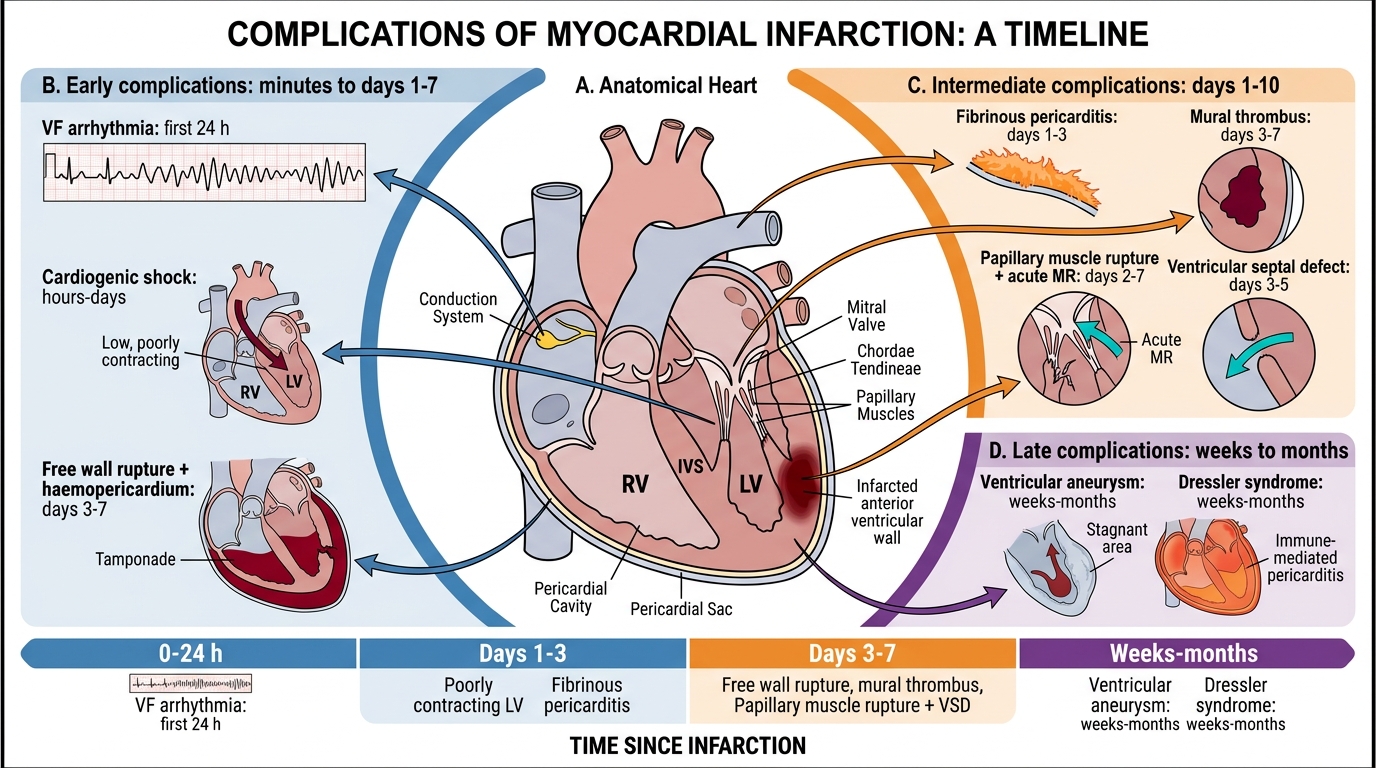
MI complications are grouped by the time at which they typically occur — this timing is directly explained by the pathological evolution of the infarct.
Early Complications (hours to days):
- Arrhythmia — the most common complication and the leading cause of death in the first few hours. Ischaemic myocytes have altered membrane potentials → re-entry circuits → ventricular tachycardia / ventricular fibrillation (VF). Also: sinus bradycardia and AV blocks (especially with inferior MI from RCA → AV node ischaemia).
- Cardiogenic shock — occurs when ≥40% of left ventricular myocardium is necrotic → pump failure → inadequate cardiac output. Clinical: hypotension, cold clammy skin, oliguria, elevated JVP. Mortality ~40–60%.
- Free wall rupture — occurs days 3–7, when the infarcted wall is maximally soft and friable (peak neutrophilic digestion). Rupture → haemopericardium → cardiac tamponade → sudden death. Most common in elderly first-MI patients with anterior or lateral transmural infarction.
- Ventricular septal defect (VSD) — septal rupture, also days 3–7. Presents as a new loud holosystolic murmur and acute heart failure. Requires urgent surgical repair.
- Papillary muscle rupture/dysfunction — posteromedial papillary muscle is most vulnerable (supplied solely by RCA; anterolateral has dual supply). Rupture → acute severe mitral regurgitation → acute pulmonary oedema. Present: new mitral regurgitation murmur + flash pulmonary oedema.
Intermediate Complications (days to weeks):
- Pericarditis — fibrinous pericarditis overlying the necrotic epicardium 2–4 days post-MI. Pleuritic chest pain, pericardial rub. Distinct from Dressler's syndrome.
- Mural thrombus — forms on the akinetic/dyskinetic endocardium overlying the infarct zone. Risk of systemic embolism → stroke, limb ischaemia. Particularly common with large anterior MI (apical akinesis). Detected by echocardiography; treated with anticoagulation.
Late Complications (weeks to months):
- Ventricular aneurysm — paradoxical outward bulging of the thinned fibrotic scar during systole. Complicates large transmural infarcts. Leads to progressive heart failure, refractory arrhythmia, and mural thrombus formation. (True aneurysm has all wall layers; pseudoaneurysm = contained rupture, surgical emergency.)
- Dressler's syndrome (post-MI syndrome) — autoimmune pericarditis weeks to months after MI. Fever, pericardial/pleural effusion, elevated ESR. Mechanism: antibodies against necrotic myocardial antigens. Responds to NSAIDs/steroids.
- Heart failure (chronic ischaemic cardiomyopathy) — progressive ventricular remodelling with dilation, fibrosis, and reduced EF following large or repeated MIs.
Timing of Major Myocardial Infarction Complications
SELF-CHECK
A 70-year-old woman is recovering in the coronary care unit on day 5 post-STEMI (anterior, large territory). She suddenly develops hypotension, elevated JVP, muffled heart sounds, and equalization of diastolic pressures on catheter measurement. ECG shows sinus tachycardia only. What is the most likely complication?
A. Papillary muscle rupture with acute mitral regurgitation
B. Ventricular septal rupture with acute shunt
C. Free wall rupture with cardiac tamponade
D. Ventricular tachycardia with haemodynamic compromise
Reveal Answer
Answer: C. Free wall rupture with cardiac tamponade
Beck's triad (hypotension, elevated JVP, muffled heart sounds) with equalisation of diastolic pressures = cardiac tamponade = free wall rupture. This is the classic presentation on days 3–7 when the necrotic wall is maximally friable due to neutrophilic infiltration. Large anterior MI in an elderly female (thin-walled, less pre-existing LV hypertrophy) is the typical risk profile. Papillary muscle rupture produces a loud mitral regurgitation murmur. VSR produces a VSD murmur. VT would show on ECG.
Interpreting Cardiac Function Tests in ACS — PA26.6
Interpreting Cardiac Function Tests in ACS
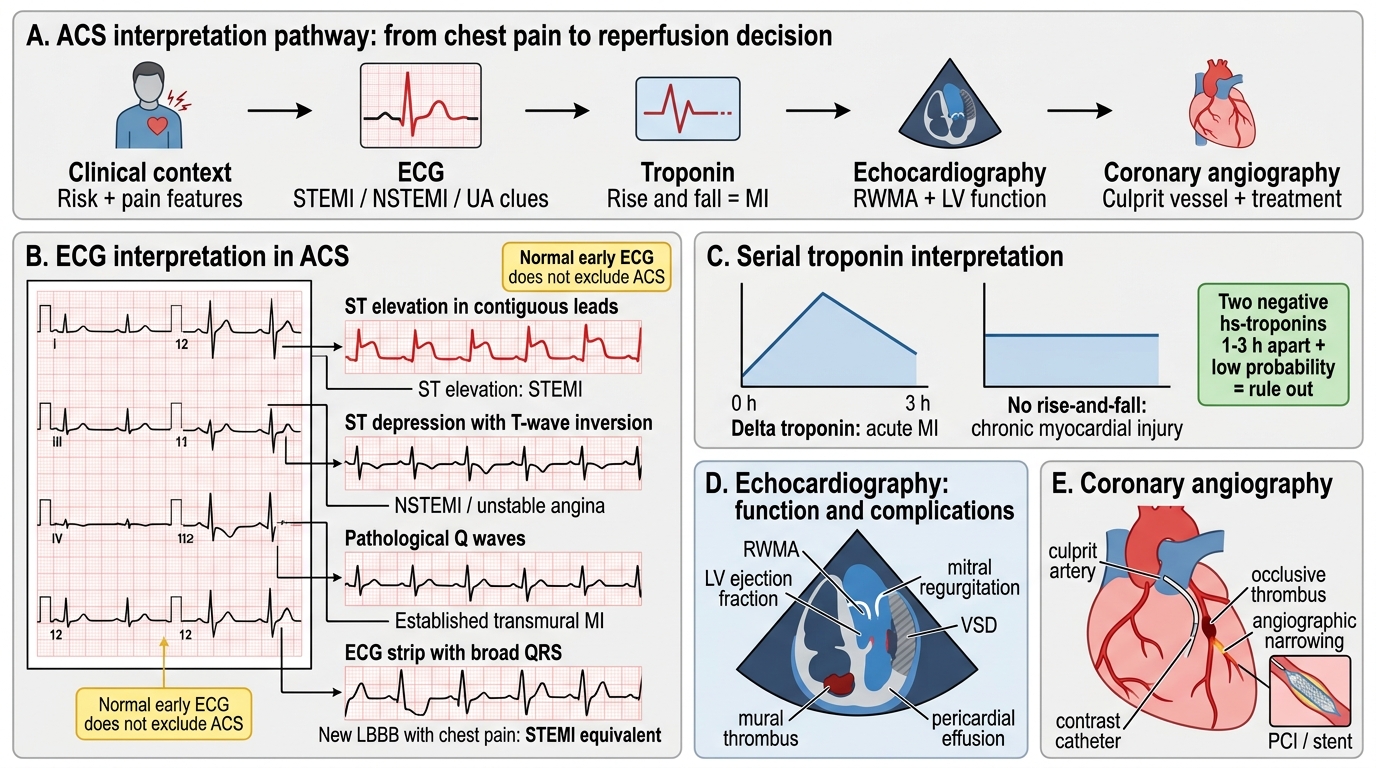
The NMC CBUC competency PA26.6 specifically requires that you can interpret cardiac function testing in ACS. Here is an integrated, examination-ready framework:
Step 1 — Clinical context:
Age, sex, risk factors, nature of pain (quality, radiation, onset, duration), relief with nitrates or rest.
Step 2 — ECG interpretation:
- Normal ECG → does NOT exclude ACS (NSTEMI, posterior MI, and early STEMI can all have normal early ECGs)
- ST elevation in ≥2 contiguous leads (>1 mm limb leads, >2 mm precordial) = STEMI → activate cath lab
- ST depression / T-wave inversion = NSTEMI or UA
- New pathological Q waves = established transmural MI
- New LBBB in chest pain = treat as STEMI equivalent
Step 3 — Troponin interpretation:
- Serial troponins at 0h and 3h (or 0h/1h for hs-troponin)
- A troponin RISE AND FALL (delta troponin) in the appropriate clinical context = MI
- Isolated elevated troponin without delta (no rise-and-fall) = chronic myocardial injury (e.g. renal failure, heart failure) rather than acute MI
- Rule-out pathway: two negative hs-troponins 1–3h apart + low clinical probability = safe discharge
Step 4 — Echocardiography:
- Regional wall motion abnormalities (RWMA) confirm ischaemic territory even before biomarker rise
- Assess LV function (ejection fraction) for risk stratification
- Detect complications: pericardial effusion, VSD, mitral regurgitation, mural thrombus
Step 5 — Coronary angiography:
- Diagnostic and therapeutic (PCI during same procedure)
- STEMI: emergency ('primary PCI')
- NSTEMI/UA: within 24–72 hours in high-risk patients
CLINICAL PEARL
The 'HEART score' integrates all five clinical domains: History (typical/atypical/non-cardiac), ECG, Age, Risk factors, and initial Troponin — each scored 0–2. A HEART score ≤3 in the ED identifies very low-risk patients safe for early discharge. High scores (≥7) predict MACE in ~50% within 6 weeks. This is a real-world application of exactly the pathophysiology you have studied — and is likely to appear in clinical-reasoning OSCEs.