Page 25 of 34
PA26.{8,10} | Pericardial Disease & Cardiac Tumours — SDL Guide
Learning Objectives
- Classify the etiology of pericarditis into infective, immune-mediated, and neoplastic categories
- Describe the gross and microscopic features of the six morphological types of pericarditis
- Explain the pathophysiology of cardiac tamponade and identify Beck's triad
- Distinguish constrictive pericarditis from cardiac tamponade in terms of mechanism and etiology
- Compare the features of pericardial effusion types — serous, serosanguineous, and chylous
- Describe the pathological features, clinical presentation, and complications of cardiac myxoma
- List the primary benign and malignant cardiac tumours, noting relative frequency
- Classify vascular tumours and identify distinguishing features of haemangioma, Kaposi sarcoma, angiosarcoma, and glomus tumour
INSTRUCTIONS
Diseases of the pericardium are tested disproportionately because they generate dramatic, exam-ready clinical pictures — the scratch of a friction rub, a heart silhouetted like a water bottle, a patient whose blood pressure falls with each breath. This module ties the morphology you will see on glass slides directly to those bedside signs, and then pivots to cardiac and vascular tumours, where pattern recognition (myxoma vs metastasis, Kaposi vs angiosarcoma) determines both diagnosis and management. Work through each block before moving ahead.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 12 (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 16 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old man presents two weeks after a 'flu-like illness' with sharp chest pain that worsens when he leans back and eases when he sits forward. Auscultation reveals a scratchy, to-and-fro sound at the left sternal border. ECG shows diffuse saddle-shaped ST elevation. Three days later the pain abates — but his neck veins are distended, his heart sounds are muffled, and his systolic blood pressure drops 15 mmHg on inspiration. What has changed morphologically, and why is he now in danger?
WHY THIS MATTERS
Pericardial disease bridges internal medicine, cardiothoracic surgery, and the autopsy table. TB remains the leading cause of constrictive pericarditis in India. Cardiac tamponade is a reversible cause of obstructive shock — missed only when the pathophysiology is not understood. Atrial myxoma mimics mitral stenosis clinically, yet is cured by surgery if caught. For the NMC CBUC examination PA26.8 and PA26.10 appear as long-answer questions requiring etiology + morphology + complications in a structured answer.
RECALL
Before you begin, revisit these concepts from Year 1:
- Pericardium — visceral (epicardium) + parietal layers; normal fluid 15–50 mL (ultrafiltrate)
- Inflammation sequence — exudate, organisation, fibrosis (from General Pathology)
- Granulomatous inflammation — Langhans giant cells, central caseation (TB) [PA Block 1]
- Heart anatomy — left atrial position relative to mitral valve [PY cardiovascular]
- Obstructive shock — mechanism differs from distributive/cardiogenic shock [PY]
If any of these feel shaky, spend five minutes reviewing before continuing.
Pericarditis — Etiology
Etiology of Pericarditis
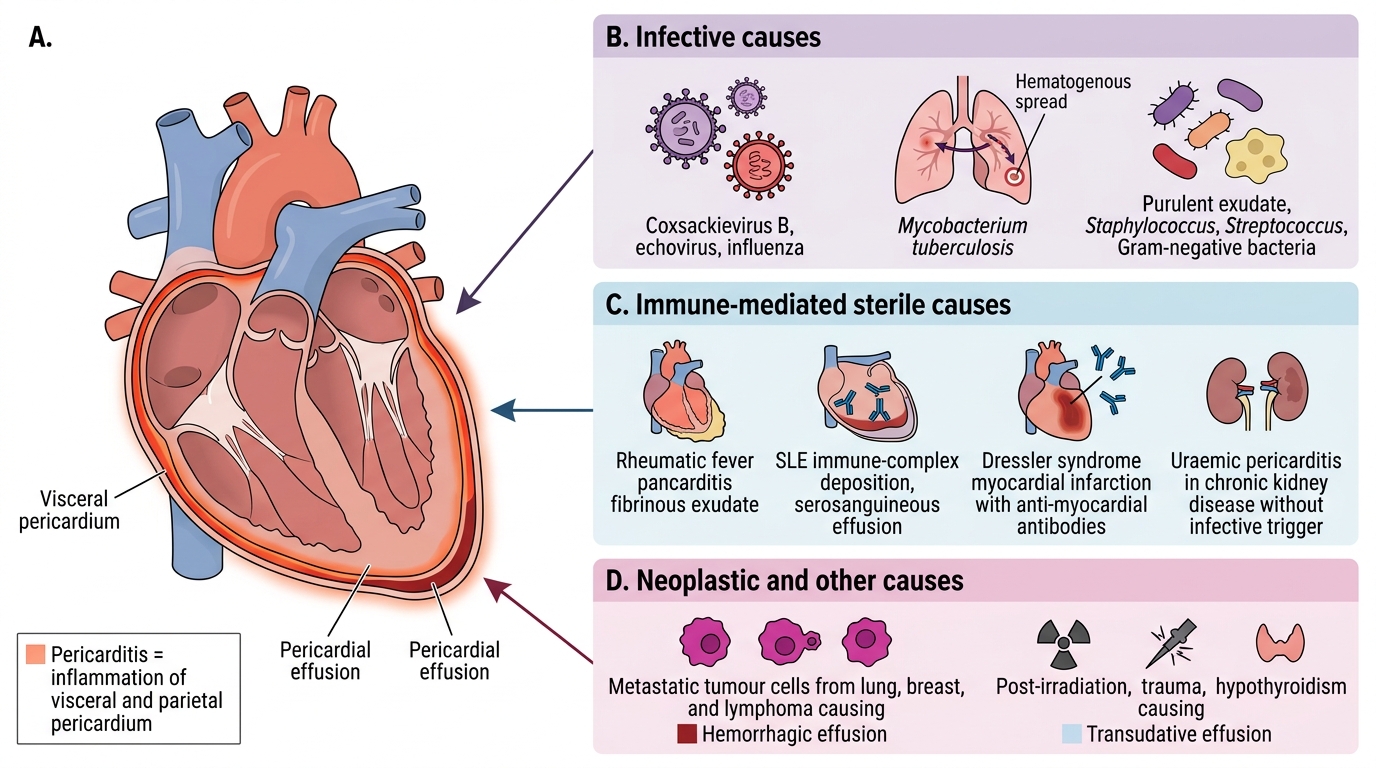
Pericarditis is inflammation of the pericardium. Causes are grouped into three broad categories:
1. Infective
• Viral — Coxsackievirus B, echovirus, influenza (commonest in young adults; often self-limiting)
• Tuberculous — Mycobacterium tuberculosis; haematogenous spread from pulmonary focus; important in India; tends to progress to constrictive disease
• Pyogenic/bacterial — Staphylococcus, Streptococcus, Gram-negatives; secondary to pneumonia, septicaemia, or mediastinitis; produces frank pus
2. Immune-mediated (sterile)
• Rheumatic fever — part of pancarditis; fibrinous exudate
• Systemic lupus erythematosus (SLE) — immune-complex deposition; serosanguineous effusion
• Dressler syndrome — autoimmune pericarditis 2–10 weeks post-myocardial infarction; anti-myocardial antibodies
• Uraemic pericarditis — in chronic kidney disease; "metabolic" sterile exudate; unique because it occurs without infective trigger
3. Neoplastic / other
• Metastatic tumours (lung, breast, lymphoma) — haemorrhagic effusion
• Post-irradiation, trauma, hypothyroidism (transudative effusion)
Morphological Types of Pericarditis
Morphological Types of Pericarditis
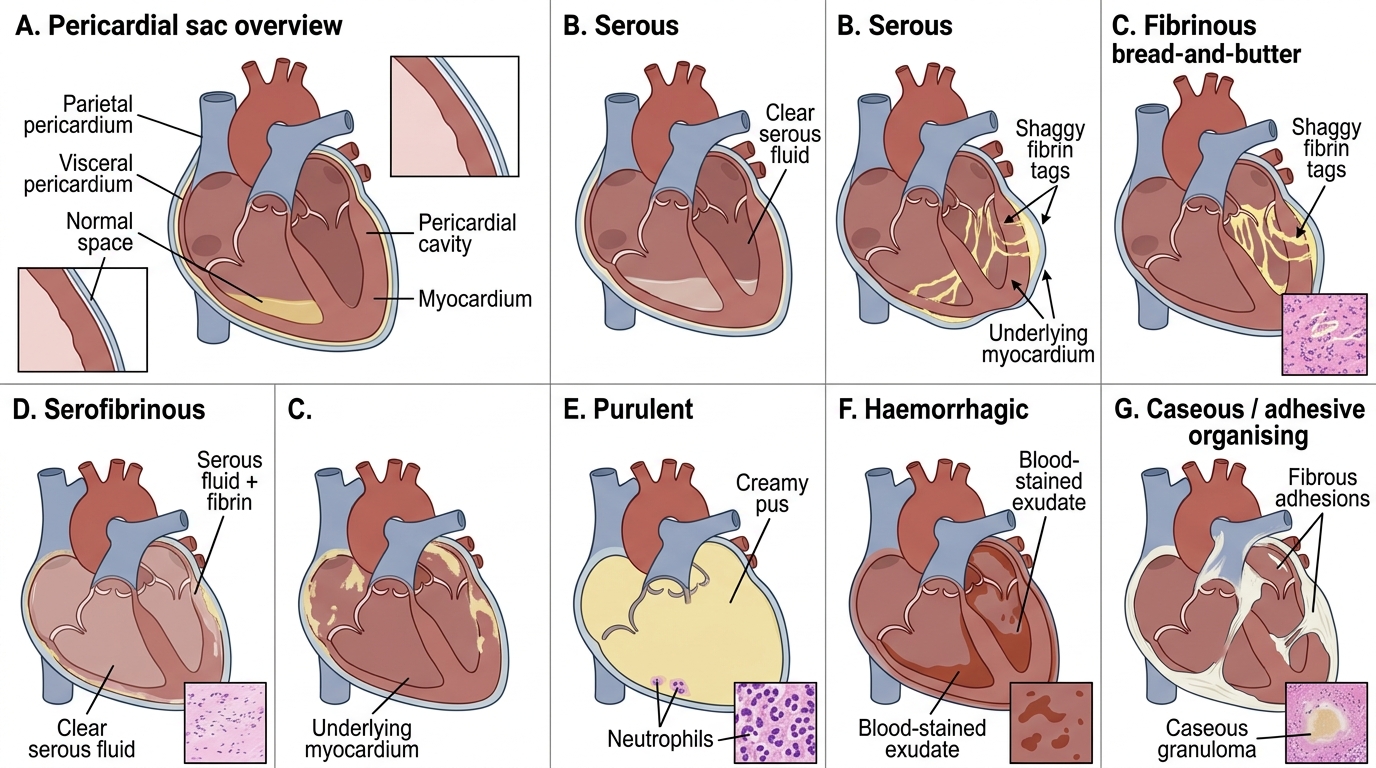
The exudate type determines the gross and microscopic appearance. Six patterns must be known:
1. Serous pericarditis
Clear, straw-coloured fluid (mostly protein-poor). Seen in viral, rheumatic, SLE, uraemic early. Visceral surface looks normal or mildly injected. Minimal fibrin. Usually resolves without sequelae.
2. Fibrinous ("bread-and-butter") pericarditis
The classic. Exudate rich in fibrin forms shaggy, rough, irregular tags on both pericardial surfaces. When the surfaces are pulled apart at autopsy it looks exactly like two pieces of buttered bread being separated — hence the eponym. Seen in: MI (early), rheumatic fever, uraemia, viral. Friction rub on auscultation. May resolve or organise to adhesions.
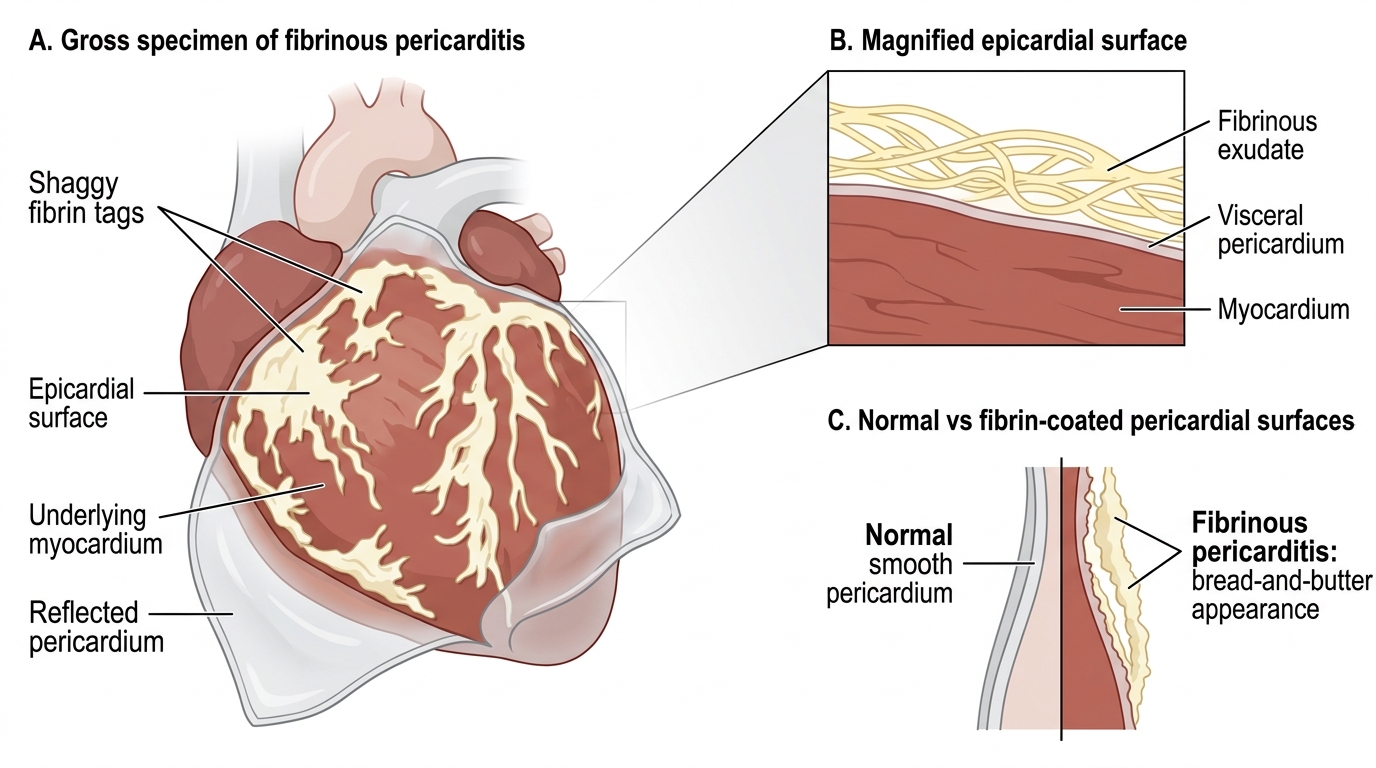
Fibrinous Pericarditis: Bread-and-Butter Appearance
3. Serofibrinous pericarditis
Mixture: serous transudate plus fibrinous deposits. Most common overall type. Same causes as fibrinous.
4. Purulent (suppurative) pericarditis
Thick, creamy pus fills the pericardial sac. Neutrophil-rich exudate on histology. Caused by pyogenic bacteria. Risk of organisation → fibrous obliteration. High mortality if untreated.
5. Haemorrhagic pericarditis
Blood-stained fluid ± fibrin. Key causes: TB (also caseous — see below), malignancy (metastatic or primary cardiac), anticoagulant therapy, ruptured aortic aneurysm. Distinguish from haemopericardium (pure blood, e.g., trauma, aortic dissection).
6. Caseous pericarditis
Specific to TB. Central caseation with epithelioid granulomas and Langhans giant cells on histology. Strong tendency to organise and calcify → constrictive pericarditis. AFB (acid-fast bacilli) demonstrable by Ziehl-Neelsen stain.
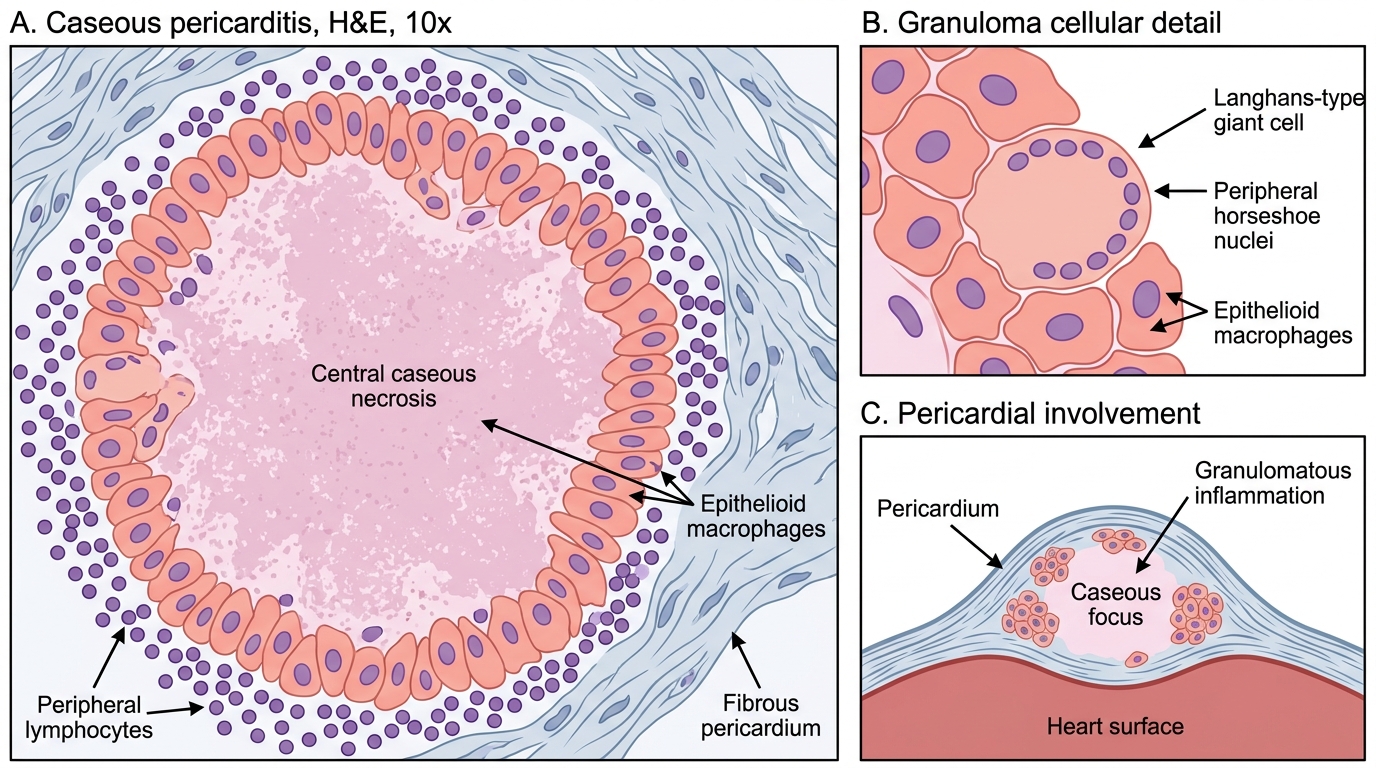
Caseous Pericarditis: Histology at 10x
SELF-CHECK
A 35-year-old presents with fever, chest pain, and a pericardial friction rub. At autopsy the pericardial surfaces show shaggy fibrin strands that separate like buttered bread. This morphological type is most characteristically associated with which condition?
A. Pyogenic bacterial infection
B. Acute myocardial infarction
C. Metastatic carcinoma
D. Chylothorax
Reveal Answer
Answer: B. Acute myocardial infarction
Fibrinous ('bread-and-butter') pericarditis is classically seen in acute MI, rheumatic fever, and uraemia. The shaggy fibrin exudate without frank pus or haemorrhage is the hallmark. Pyogenic infection produces purulent (suppurative) pericarditis; metastases cause haemorrhagic effusion; chylothorax is a pleural, not pericardial, finding.
Pericardial Effusion
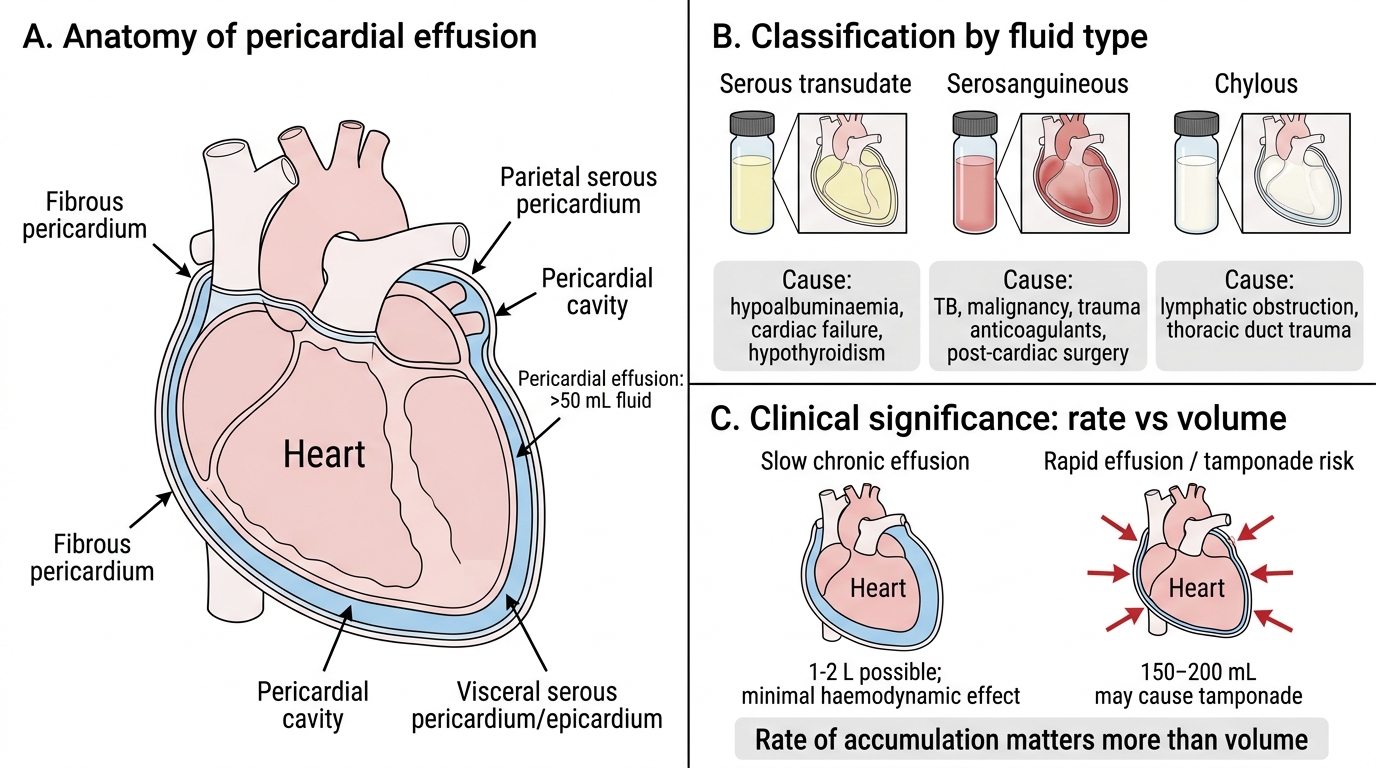
Pericardial Effusion: Fluid Type and Tamponade Risk
A pericardial effusion is excess fluid in the pericardial cavity (>50 mL). Classification by fluid type:
| Type | Appearance | Mechanism / Causes |
|---|---|---|
| Serous (transudate) | Clear, pale yellow | Low oncotic pressure (hypoalbuminaemia, nephrotic), high hydrostatic pressure (cardiac failure), hypothyroidism |
| Serosanguineous | Blood-tinged | TB, malignancy, trauma, anticoagulants, post-cardiac surgery |
| Chylous | Milky white | Lymphatic obstruction (mediastinal tumour, thoracic duct trauma) |
Rate of accumulation matters more than volume. The pericardium can accommodate 1–2 L if it distends slowly (chronic effusion) with minimal haemodynamic effect. Rapid accumulation of as little as 150–200 mL can cause tamponade because the pericardium cannot stretch fast enough.