Page 26 of 34
PA26.{8,10} | Pericardial Disease & Cardiac Tumours — SDL Guide (Part 2)
Cardiac Tamponade
Cardiac Tamponade: Pathophysiology and Clinical Signs
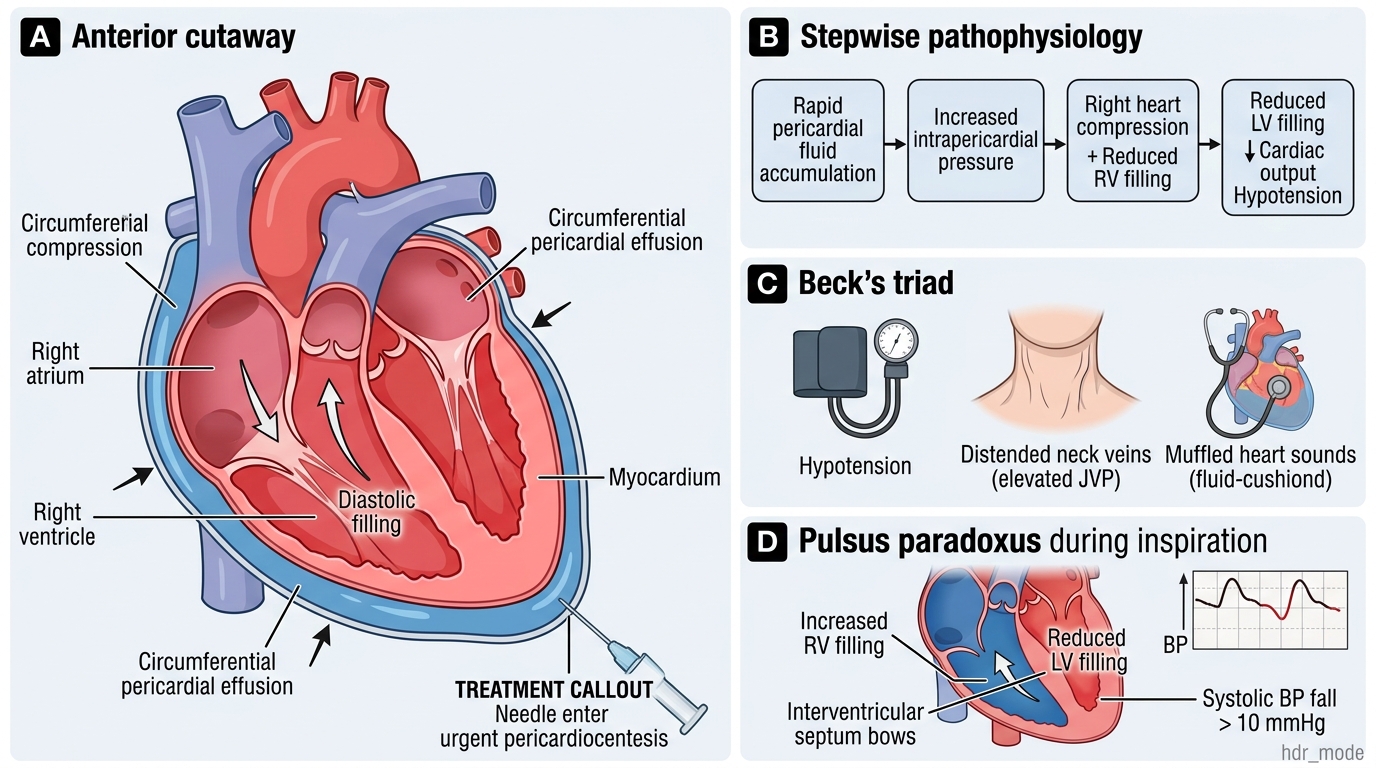
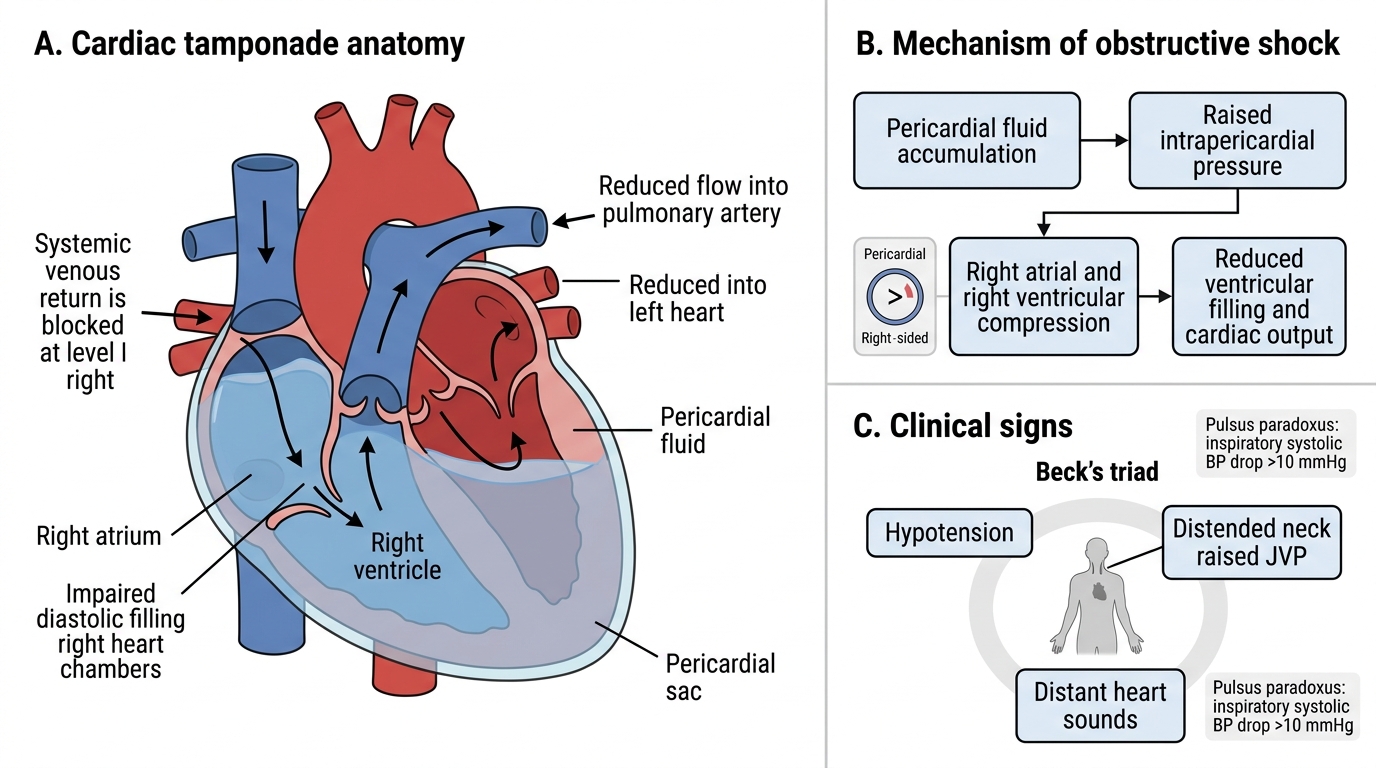
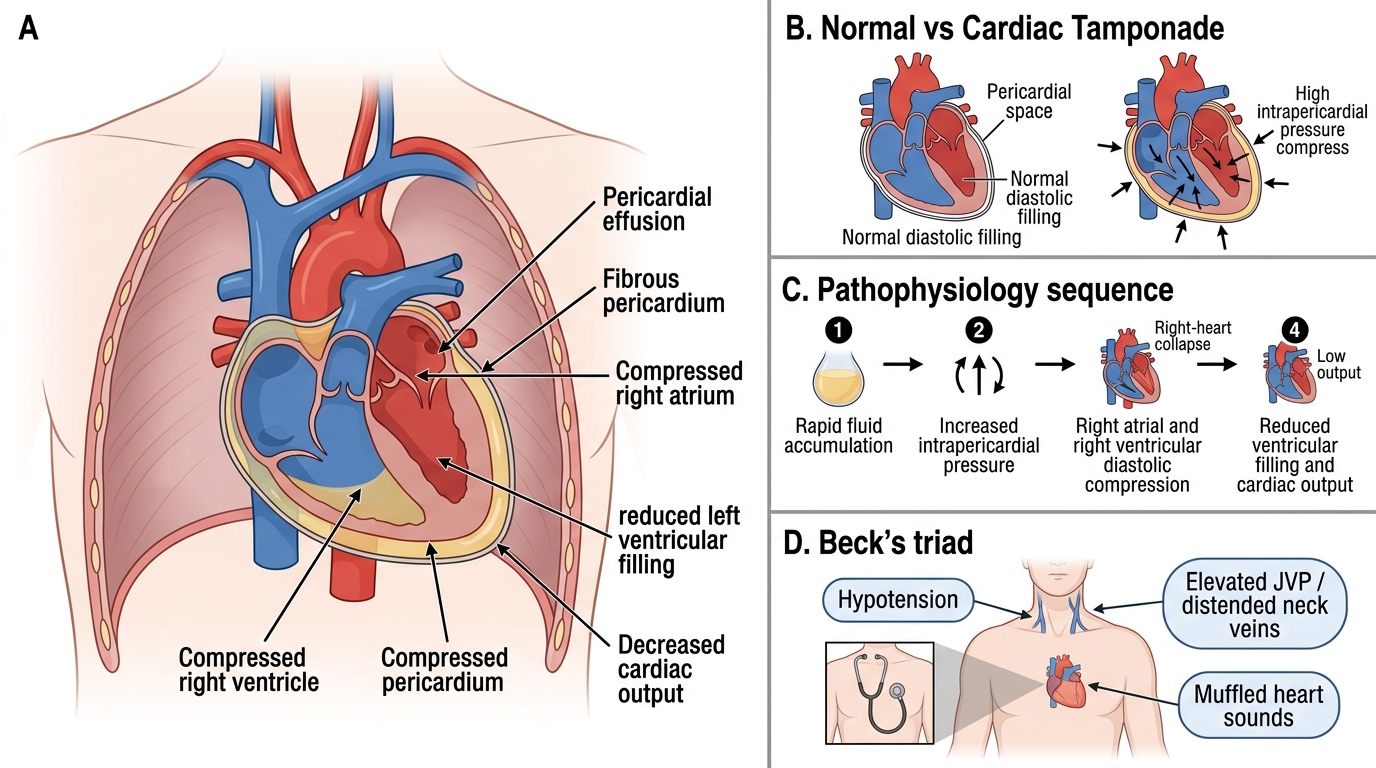
Cardiac tamponade is life-threatening compression of the heart by a rapidly accumulating pericardial effusion, leading to obstructive shock.
Pathophysiology (step by step):
1. Rapid fluid accumulation → ↑ intrapericardial pressure
2. Pressure exceeds right atrial and right ventricular diastolic pressure → compression of right heart
3. ↓ Right ventricular filling → ↓ pulmonary venous return → ↓ left ventricular filling
4. ↓ Cardiac output → hypotension, tachycardia, compensatory peripheral vasoconstriction
Beck's triad (classic clinical signs):
1. Hypotension (↓ stroke volume)
2. Elevated JVP / distended neck veins (↑ venous back-pressure)
3. Muffled / distant heart sounds (fluid cushion around heart)
Pulsus paradoxus — inspiratory fall in systolic BP >10 mmHg. Mechanism: inspiration → ↑ RV filling (intrathoracic pressure ↓) → interventricular septum bows left → ↓ LV filling → ↓ LV stroke volume during inspiration. Exaggerated in tamponade because the pericardial space is fixed.
Treatment: urgent pericardiocentesis (needle aspiration of fluid).
Pathophysiology of Cardiac Tamponade
CLINICAL PEARL
Pulsus paradoxus is not 'paradoxical' in the sense of being absent — it is an exaggeration of the normal inspiratory dip in blood pressure. In tamponade the dip exceeds 10 mmHg and can be measured at the bedside with a standard sphygmomanometer. Also remember: Beck's triad is incompletely present in many cases — distended neck veins alone in a hypotensive patient after trauma should raise immediate suspicion of tamponade.
SELF-CHECK
A 45-year-old with known lung cancer develops worsening dyspnoea and hypotension. JVP is markedly elevated and heart sounds are distant. An inspiratory drop of 18 mmHg in systolic BP is noted. Which mechanism best explains the elevated JVP?
A. Left ventricular systolic failure causing pulmonary oedema and back-pressure
B. Increased intrapericardial pressure compressing the right heart and obstructing venous return
C. Constrictive fibrosis of the pericardium preventing diastolic expansion
D. Tricuspid valve regurgitation from right ventricular volume overload
Reveal Answer
Answer: B. Increased intrapericardial pressure compressing the right heart and obstructing venous return
Cardiac tamponade causes obstructive shock. Elevated intrapericardial pressure compresses the right atrium and ventricle, preventing venous drainage into the heart — hence JVP rises. This is distinct from LV failure (option A, where pulmonary oedema rather than elevated JVP dominates early) or constrictive pericarditis (option C, which is chronic, not acute). The scenario — malignancy, haemorrhagic effusion, rapid onset — is classic for tamponade.
Constrictive Pericarditis
Constrictive Pericarditis: Pathology and Hemodynamics
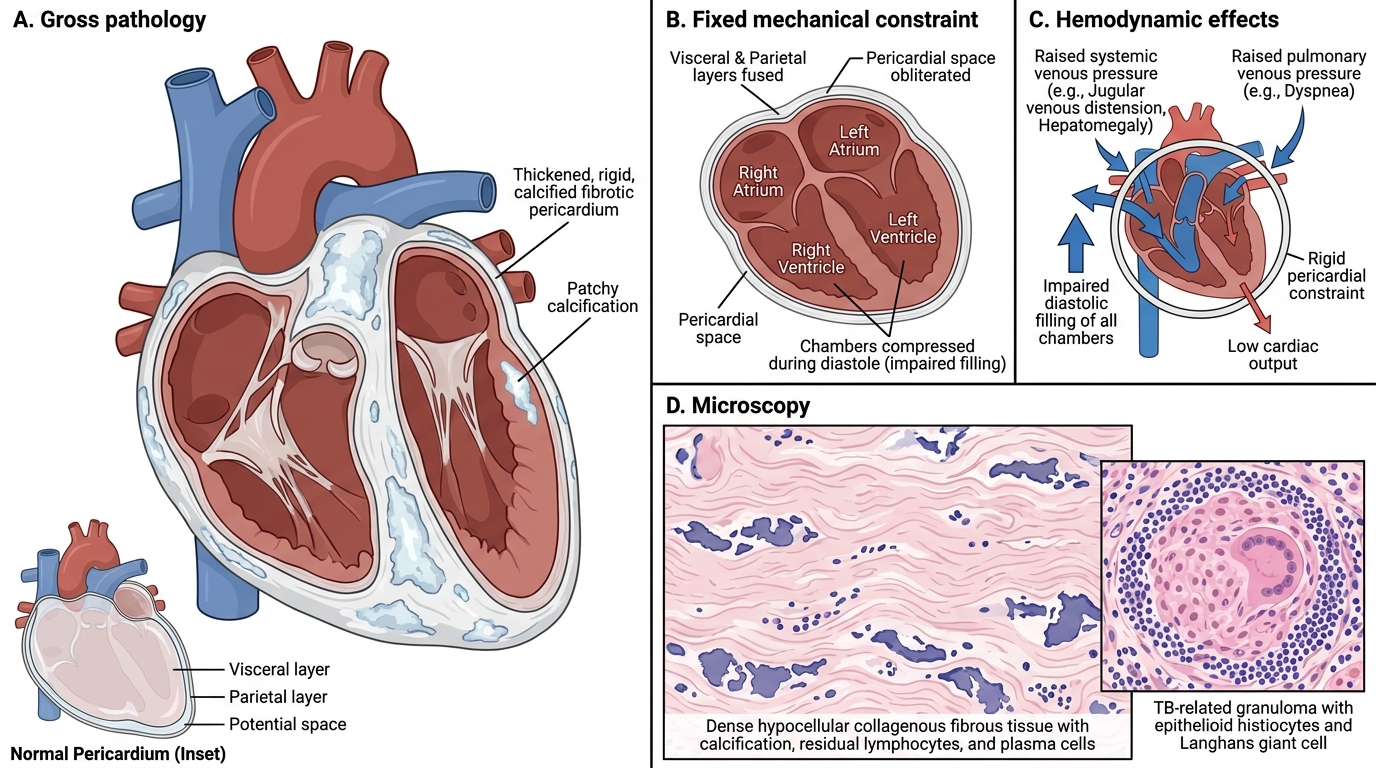
Constrictive pericarditis results from dense fibrous (and often calcified) encasement of the heart following chronic pericardial inflammation. The rigid shell prevents diastolic filling of all four chambers.
Etiology: TB is the most important cause in India and the developing world. Others: post-surgical, post-irradiation, haemopericardium organisation, idiopathic.
Gross: Pericardium is markedly thickened, often >1 cm (normal <3 mm), dense white fibrous tissue, frequently with calcification (visible on chest X-ray as 'eggshell' calcification or on CT). Visceral and parietal layers are fused — pericardial space is obliterated.
Microscopy: Dense hypocellular collagenous fibrous tissue with variable calcification. Residual lymphocytes and plasma cells. In TB cases, granulomas may still be identifiable.
Haemodynamic consequence: Impaired diastolic filling of all chambers simultaneously → raised venous pressure (bilateral — both systemic and pulmonary), low cardiac output. Unlike tamponade, this is a fixed mechanical constraint.
Treatment: Pericardiectomy (surgical stripping) — the only definitive treatment.
Cardiac Tumours — Overview & Metastases
Cardiac Tamponade: Mechanism and Clinical Signs
Metastases are far more common than primary cardiac tumours — ratio approximately 20–40:1. Any malignant tumour can metastasise to the heart via haematogenous, lymphatic, or direct extension routes.
- Commonest primary sites metastasising to heart: lung carcinoma, breast carcinoma, malignant melanoma, lymphoma, leukaemia
- Melanoma has the highest rate of cardiac metastasis relative to other tumours
- Clinically silent until large or until they cause effusion, arrhythmia, or obstruction
Primary cardiac tumours are rare but high-yield for examinations because each type has a distinctive pathological picture:
| Category | Tumour | Key features |
|---|---|---|
| Benign | Myxoma (commonest overall primary) | Left atrium, gelatinous, ball-valve obstruction |
| Benign | Rhabdomyoma (commonest in children) | Ventricular septum/walls; tuberous sclerosis |
| Benign | Lipoma | Any chamber, subepicardial fat |
| Benign | Papillary fibroelastoma | Valves; risk of embolism |
| Malignant | Angiosarcoma (commonest primary malignant) | Right atrium; haemorrhagic; aggressive |