Page 27 of 34
PA26.{8,10} | Pericardial Disease & Cardiac Tumours — SDL Guide (Part 3)
Cardiac Myxoma
Cardiac Myxoma: Morphology and Clinical Effects
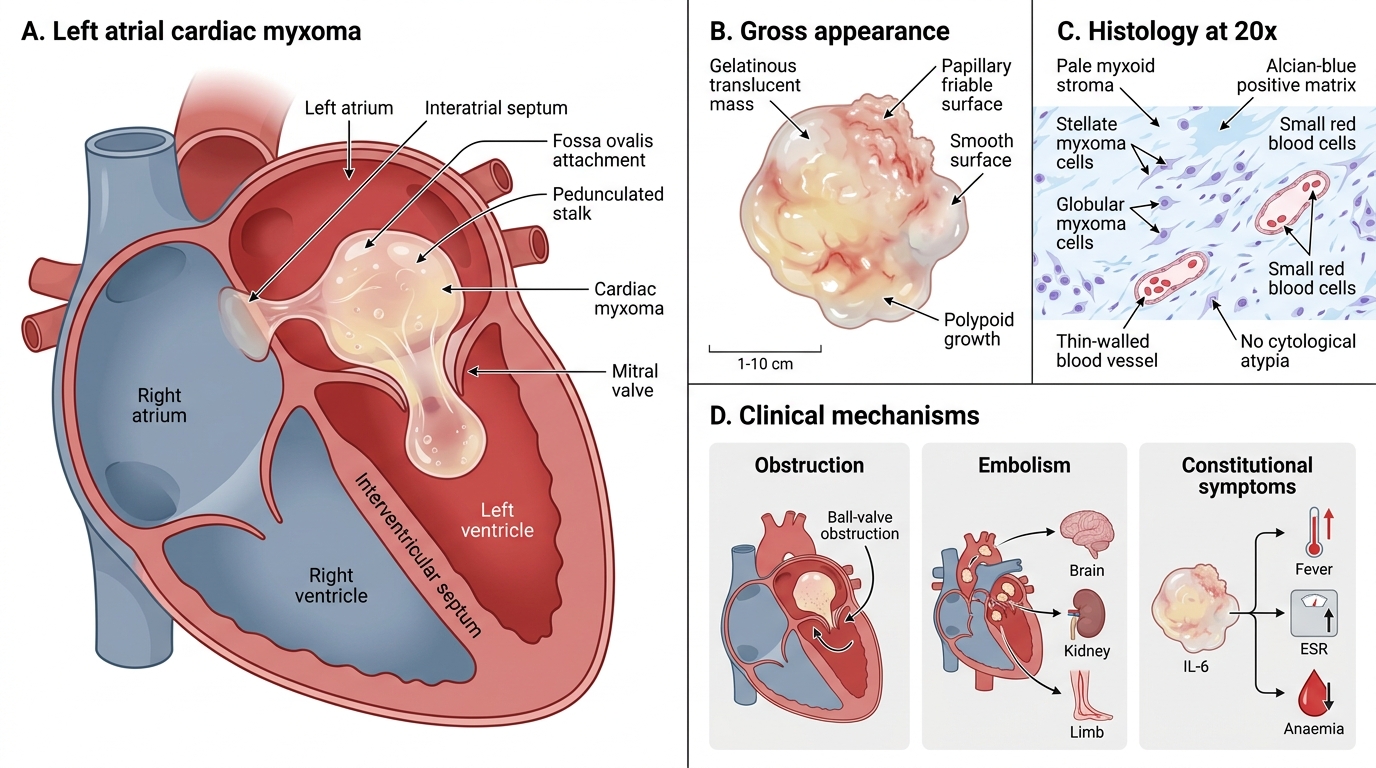
Cardiac myxoma is the commonest primary tumour of the heart in adults.
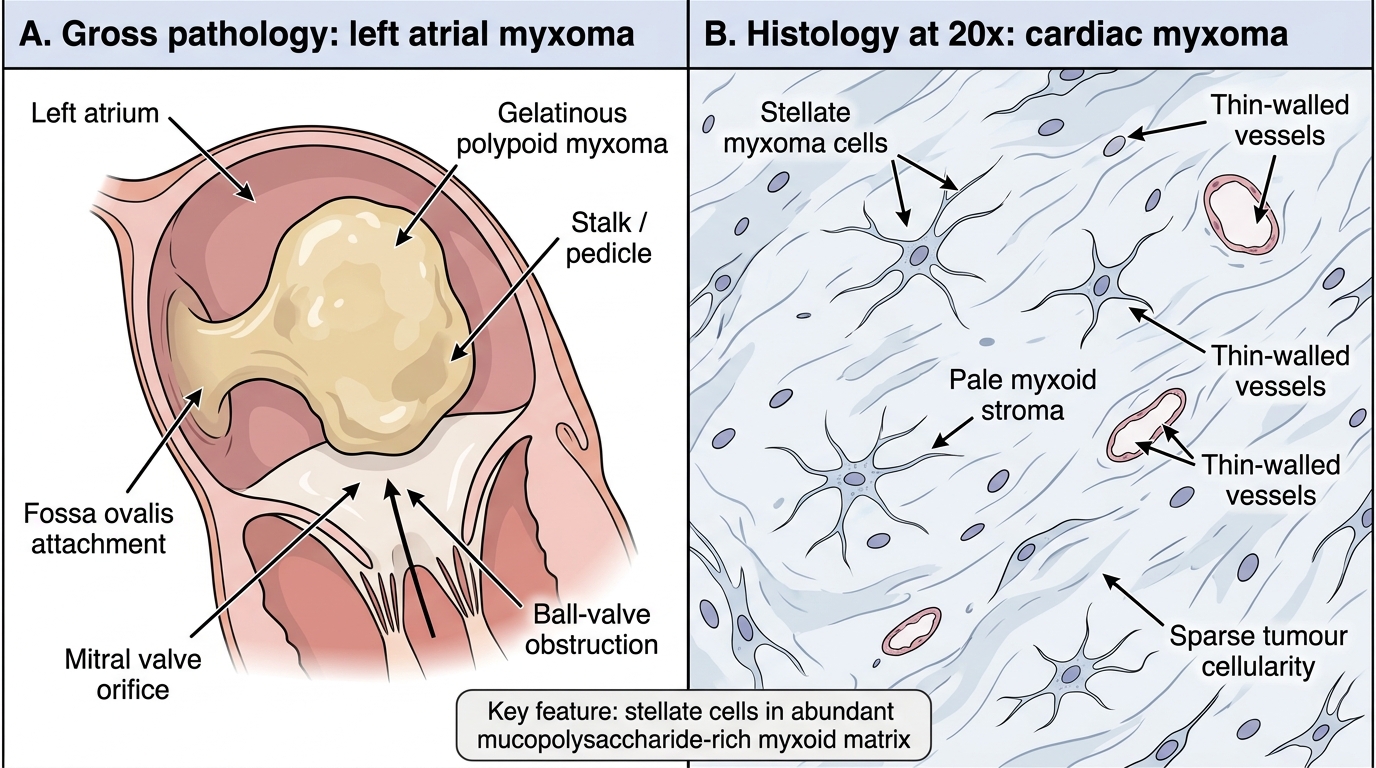
Location: ~75% arise in the left atrium, attached to the interatrial septum near the fossa ovalis by a broad or pedunculated stalk. Right atrium ~20%; ventricles rare.
Gross appearance:
• Soft, gelatinous, glistening, translucent mass
• Surface may be smooth or papillary (friable — embolic risk)
• Size: 1–10 cm diameter
• Polypoid or sessile; pedunculated forms can prolapse through the mitral valve
Histology:
• Myxoma cells (stellate or globular cells) scattered within abundant myxoid (mucopolysaccharide-rich) stroma
• Cells embedded in a pale basophilic matrix (Alcian-blue positive)
• Thin-walled blood vessels; occasional smooth muscle, haematopoietic cells
• No cytological atypia (benign)
Left Atrial Myxoma: Gross and Histological Features
Clinical presentation (three mechanisms):
1. Obstruction — pedunculated myxoma intermittently occludes the mitral valve → syncope, dyspnoea that varies with posture ('ball-valve' obstruction); mimics mitral stenosis
2. Embolism — friable surface fragments detach → systemic emboli (stroke, limb ischaemia, renal infarcts)
3. Constitutional — fever, weight loss, elevated ESR, anaemia (interleukin-6 secretion by tumour cells)
Treatment: surgical excision — curative in most cases.
SELF-CHECK
A 52-year-old woman presents with syncopal episodes that occur when she bends forward, progressive dyspnoea, and an early diastolic 'tumour plop' on auscultation. Echocardiography shows a mobile left atrial mass attached near the fossa ovalis. Which histological feature is MOST characteristic of this tumour?
A. Sheets of small round cells with hyperchromatic nuclei and scanty cytoplasm
B. Multinucleated giant cells in an inflammatory stroma
C. Stellate cells within an abundant pale myxoid (mucopolysaccharide-rich) matrix
D. Intracytoplasmic vacuoles distending the cell (spider cells)
Reveal Answer
Answer: C. Stellate cells within an abundant pale myxoid (mucopolysaccharide-rich) matrix
The clinical picture — left atrial mass near the fossa ovalis, postural syncope, tumour plop — is classic for myxoma. Histologically it is defined by stellate/globular myxoma cells scattered in an abundant Alcian-blue-positive myxoid stroma with thin-walled vessels (option C, index 2). Option A describes small round blue-cell tumours (e.g., lymphoma); option B describes granulomatous inflammation; option D (spider cells with vacuoles) is characteristic of rhabdomyoma.
Other Primary Cardiac Tumours
Other Primary Cardiac Tumours
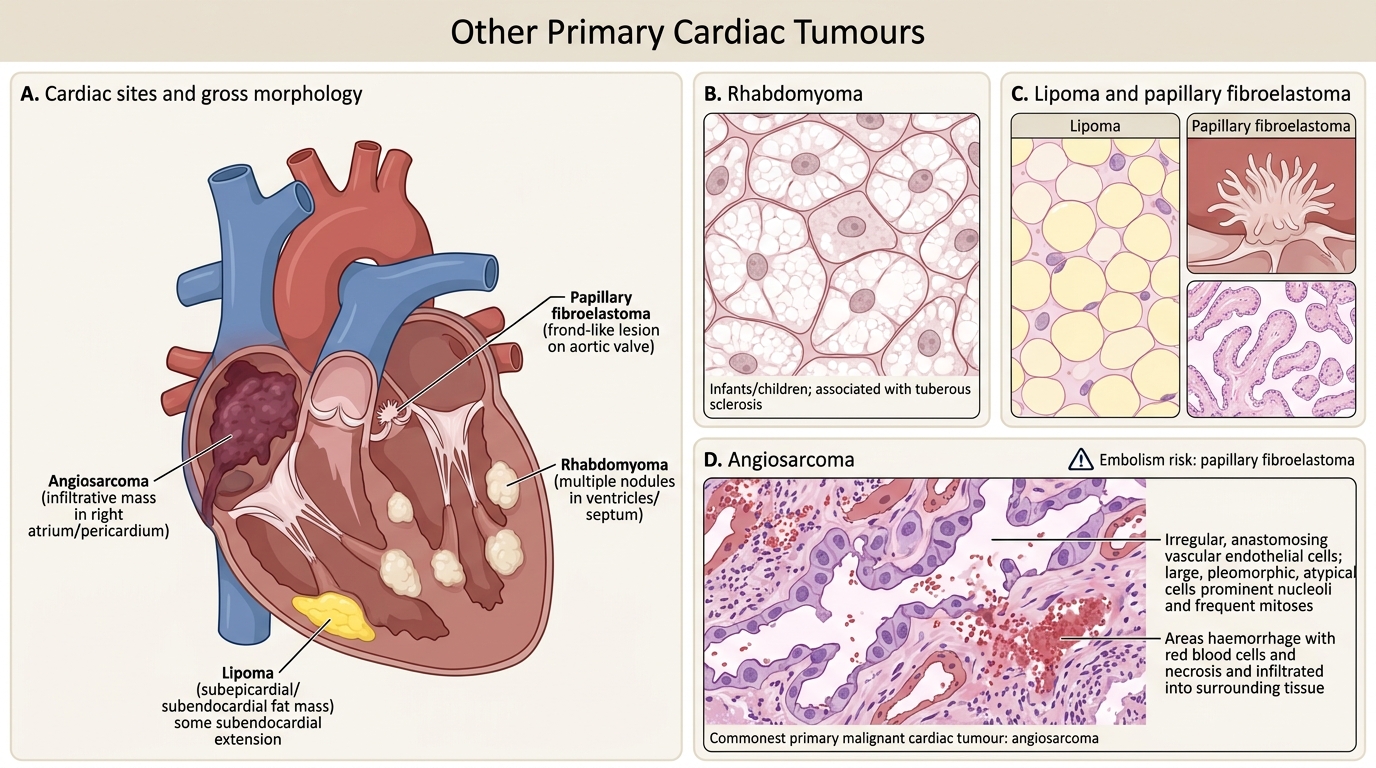
Rhabdomyoma — commonest cardiac tumour in infants and children. Hamartomatous; strongly associated with tuberous sclerosis complex (~50% of patients with tuberous sclerosis have rhabdomyomas). Located in ventricular myocardium / septum. Histology: large, vacuolated spider cells (glycogen-distended myocytes with cytoplasmic strands extending to the cell membrane). Usually multiple, often regress spontaneously.
Lipoma — benign; subepicardial or subendocardial; mature adipocytes; usually asymptomatic incidental finding.
Papillary fibroelastoma — tiny, frond-like tumour on valve surface (aortic > mitral). Grossly resembles a sea anemone. Risk: embolism (stroke). On histology: papillary projections lined by endothelium; avascular elastic core.
Angiosarcoma (primary cardiac malignant)
• Commonest primary malignant cardiac tumour
• Usually right atrium; infiltrates pericardium early
• Haemorrhagic, necrotic mass
• Histology: anastomosing vascular channels lined by atypical endothelial cells; mitoses; necrosis
• Prognosis poor; usually presents late
• Note: angiosarcoma also occurs in soft tissue, liver (vinyl chloride exposure), breast, and skin (post-mastectomy lymphoedema — Stewart–Treves syndrome)
Vascular Tumours
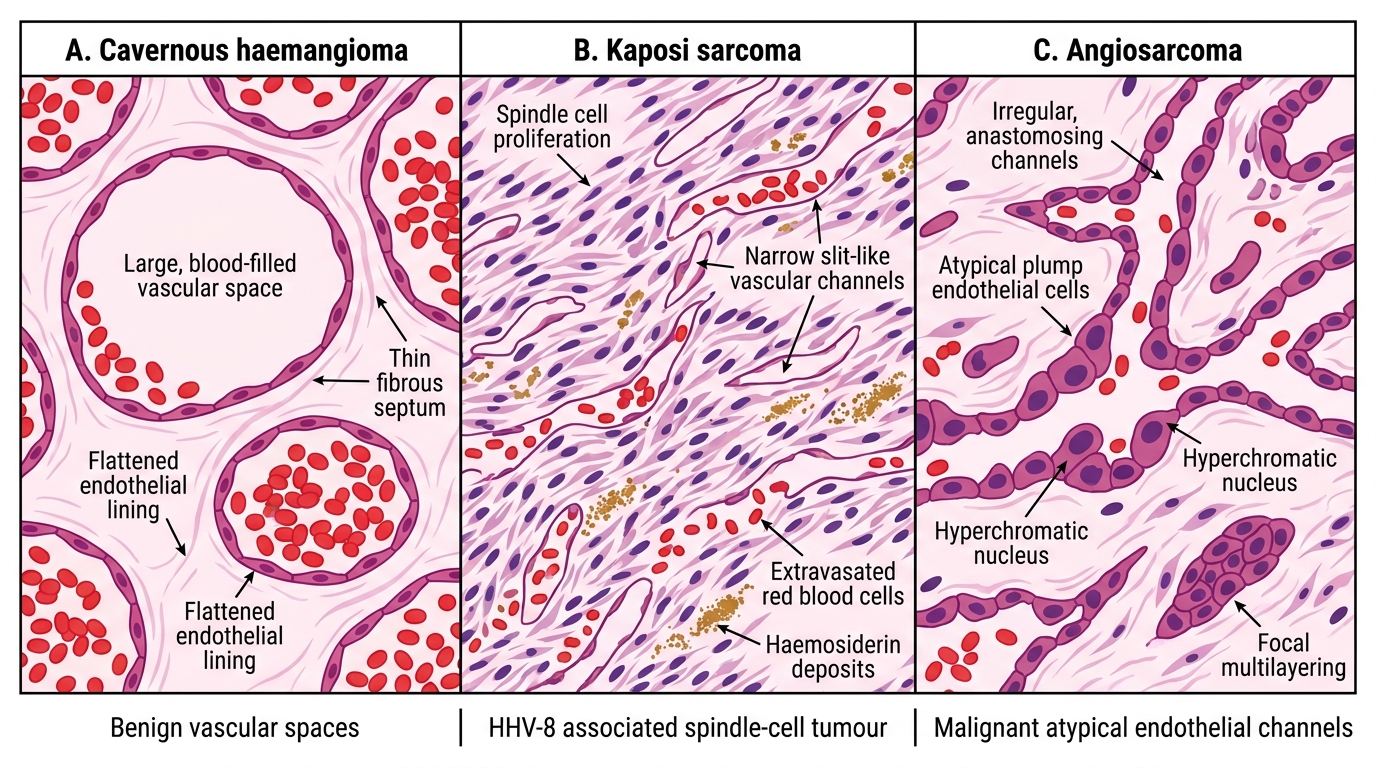
Vascular Tumours: Classification and Key Morphology
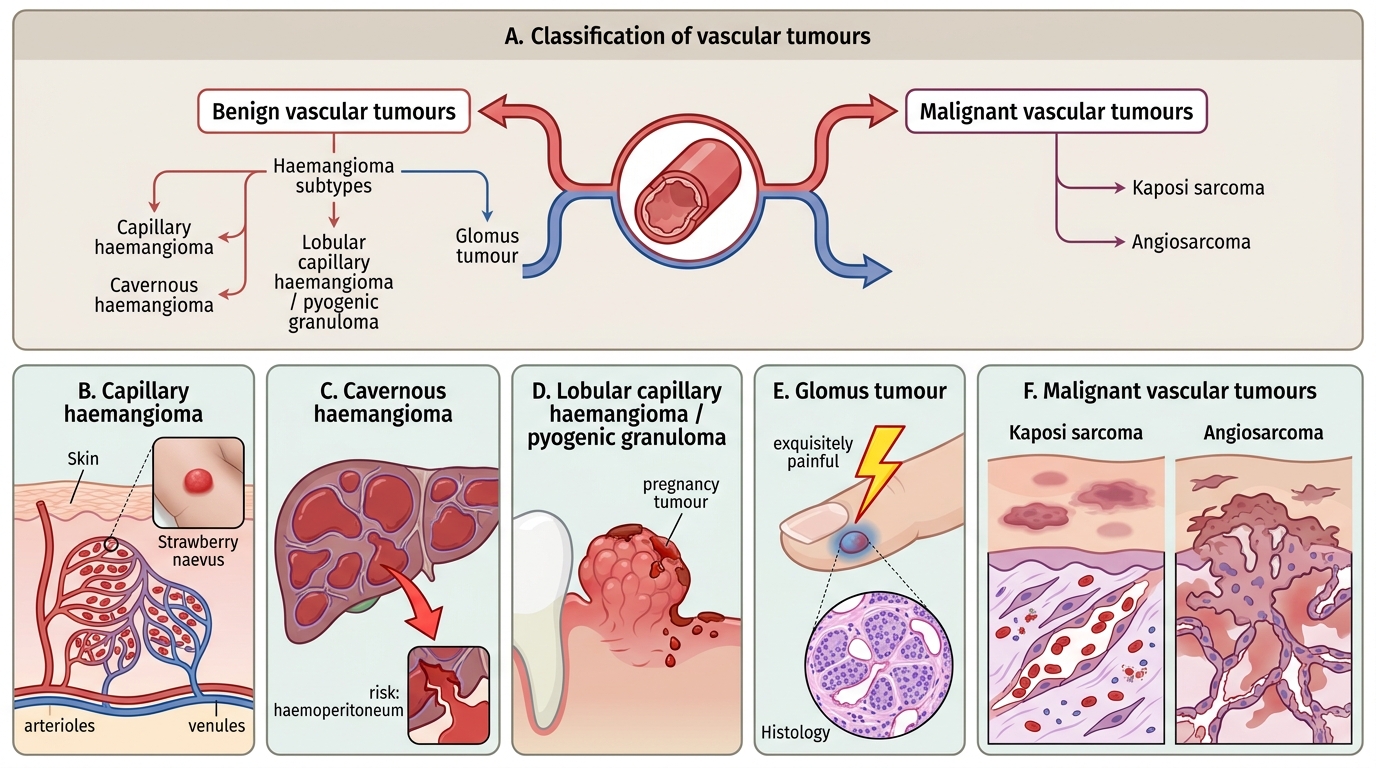
Vascular tumours arise from the endothelium or pericytes of blood vessels. A brief but exam-relevant classification:
Benign vascular tumours
Haemangioma — commonest benign vascular tumour overall; often congenital.
• Capillary haemangioma: lobules of thin-walled capillaries; appears in skin/liver/mucosa; often involutes in childhood ("strawberry naevus")
• Cavernous haemangioma: large, thin-walled vascular spaces engorged with blood; liver is common site; risk of rupture + haemoperitoneum
• Lobular capillary haemangioma (pyogenic granuloma): polypoid, bleeds easily; gingiva, skin; associated with pregnancy ("pregnancy tumour")
Glomus tumour (glomangioma) — benign, derived from glomus body (arteriovenous thermoregulatory unit). Exquisitely painful. Subungual location (under fingernail) classic. Histology: nests of small round glomus cells (modified smooth muscle) around dilated vascular channels.
Malignant vascular tumours
Kaposi sarcoma — low-grade endothelial malignancy caused by Human Herpesvirus 8 (HHV-8). Four clinical forms:
1. Classic: elderly Eastern European men; lower limbs; indolent
2. AIDS-related (epidemic): most common AIDS-defining malignancy; skin, mucosa, viscera; aggressive
3. African endemic: children and young adults in sub-Saharan Africa
4. Iatrogenic: immunosuppressed transplant recipients
Histology: spindle cell proliferation + slit-like vascular spaces + red cell extravasation + haemosiderin.
Angiosarcoma — malignant tumour of endothelial cells. Can arise in liver (vinyl chloride, thorotrast), breast (post-irradiation), skin (post-mastectomy lymphoedema — Stewart–Treves), or heart (right atrium). Histology: irregular anastomosing channels lined by pleomorphic endothelial cells; haemorrhage; necrosis; mitoses. Aggressive; poor prognosis.
Vascular Tumour Histology Comparison
SELF-CHECK
A 34-year-old HIV-positive man develops multiple purplish skin nodules on his lower limbs and palate. Histology shows spindle cell proliferation with slit-like vascular spaces and haemosiderin deposits. Which virus is the primary aetiological agent?
A. Human Herpesvirus 8 (HHV-8)
B. Epstein-Barr virus (EBV)
C. Human papillomavirus (HPV)
D. Hepatitis B virus (HBV)
Reveal Answer
Answer: A. Human Herpesvirus 8 (HHV-8)
Kaposi sarcoma is caused by Human Herpesvirus 8 (HHV-8), also called Kaposi sarcoma-associated herpesvirus (KSHV). The clinical picture — AIDS, violaceous skin/mucosa nodules, spindle cells with slit-like spaces and haemosiderin on histology — is diagnostic. EBV causes lymphomas and nasopharyngeal carcinoma; HPV causes cervical and oropharyngeal carcinomas; HBV is associated with hepatocellular carcinoma.
CLINICAL PEARL
A useful exam framework: when asked about 'cardiac tumour' remember the 3-2-1 rule. 3 categories of primary benign tumours to know in detail (myxoma, rhabdomyoma, papillary fibroelastoma). 2 malignant cardiac associations (angiosarcoma = primary; any carcinoma/lymphoma = metastatic). 1 key ratio: metastases outnumber primary tumours 20–40:1. In any clinical scenario where a cardiac mass is found in a patient with known extracardiac malignancy, metastasis is always the first diagnosis to consider.
Complications — Summary Table
Complications of Pericardial, Cardiac, and Vascular Lesions
| Condition | Key Complications |
|---|---|
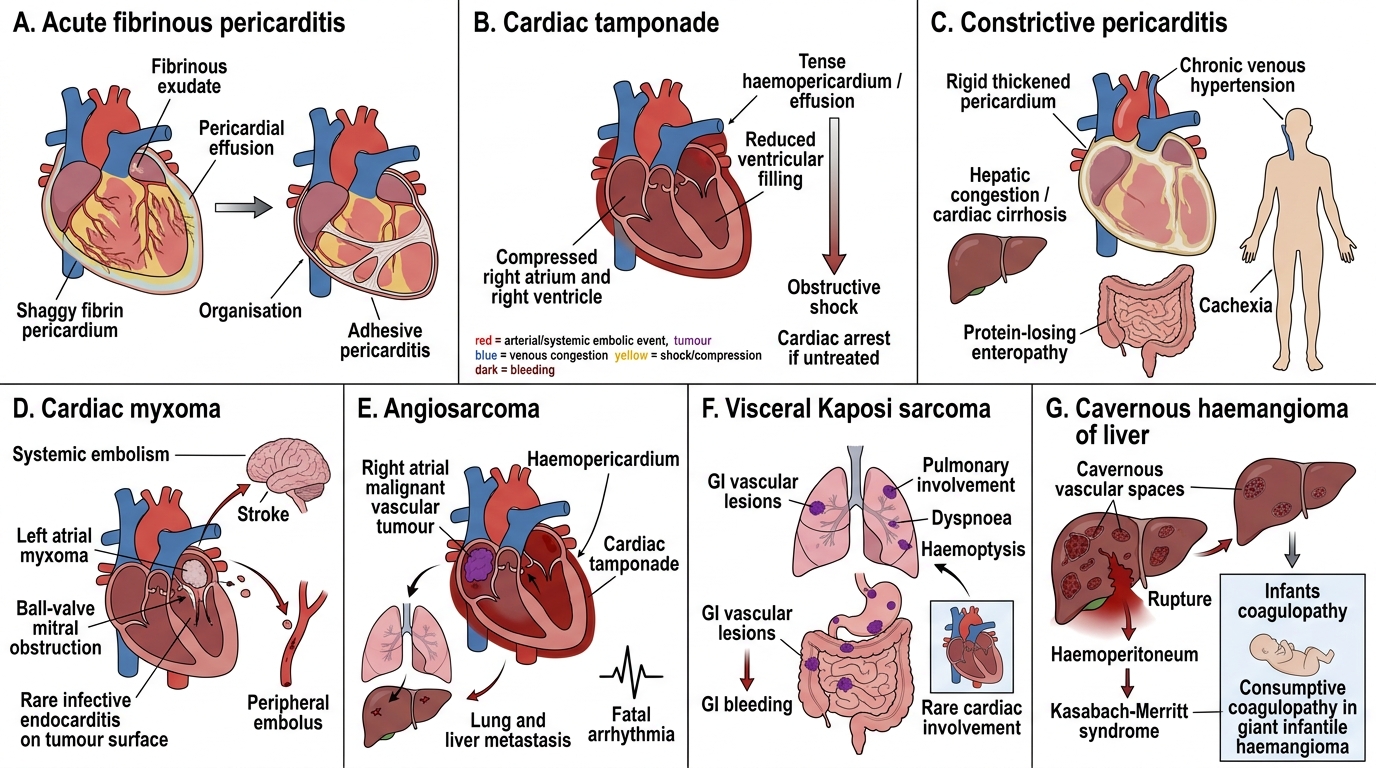
| Acute fibrinous pericarditis | Pericardial effusion; organisation → adhesive pericarditis |
| Cardiac tamponade | Obstructive shock; cardiac arrest if untreated |
| Constrictive pericarditis | Chronic venous hypertension; hepatic congestion (cardiac cirrhosis); protein-losing enteropathy; cachexia |
| Cardiac myxoma | 'Ball-valve' mitral obstruction; systemic embolism (stroke, peripheral); rarely infectious endocarditis on tumour surface |
| Angiosarcoma | Haemopericardium; cardiac tamponade; metastasis (lung, liver); fatal arrhythmia |
| Kaposi sarcoma (visceral) | GI bleeding; pulmonary involvement (dyspnoea, haemoptysis); rarely cardiac involvement |
| Cavernous haemangioma (liver) | Rupture → haemoperitoneum; Kasabach-Merritt syndrome (consumptive coagulopathy in giant haemangiomas in infants) |