Page 15 of 34
PA26.{5,7} | Rheumatic Heart Disease & Infective Endocarditis — SDL Guide
Learning Objectives
- Describe the etiology and molecular pathogenesis of acute rheumatic fever, including molecular mimicry and the role of group-A Streptococcus
- Apply the Jones criteria to diagnose acute rheumatic fever (major and minor criteria)
- Identify the pathological features of pancarditis — Aschoff bodies, MacCallum plaques, and verrucae
- Explain the progression from acute rheumatic carditis to chronic rheumatic heart disease and mitral stenosis
- Distinguish acute from subacute infective endocarditis by organism, valve substrate, vegetation morphology, and clinical course
- Apply the Duke criteria to the clinical diagnosis of infective endocarditis
- List the major complications of both chronic rheumatic heart disease and infective endocarditis
- Compare vegetation types: rheumatic, acute IE, subacute IE, NBTE, and Libman-Sacks endocarditis
INSTRUCTIONS
Rheumatic heart disease remains the leading cause of acquired heart disease in young people across India and the developing world. Understanding the molecular events that follow a simple throat infection — and how they silently scar a valve over years — is essential clinical knowledge. Infective endocarditis layers a life-threatening infection on top of already-damaged valves. These two conditions together account for most valve surgery in this country. This module builds from strep pharyngitis all the way to septic emboli and glomerulonephritis — master it and you will understand the pathological basis of the cardiology ward.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 12 — Heart (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch. 16 — Cardiovascular System (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-year-old girl presents with fever, fleeting joint pains, and a new heart murmur two weeks after a sore throat. She recovers — but 20 years later she is breathless climbing stairs, with a loud S1 and a rumbling mid-diastolic murmur. Her echocardiogram shows a valve area of 0.8 cm². Between that adolescent sore throat and this middle-aged breathlessness lies an elegant and cruel story of molecular mimicry, chronic scarring, and haemodynamic compensation. This module tells that story — and adds infective endocarditis, which is waiting in the wings every time the valve is bacteraemic.
WHY THIS MATTERS
India carries over 30% of the global burden of rheumatic heart disease. In the medical wards and OPD you will encounter mitral stenosis, infective endocarditis, and their complications weekly. The Jones criteria, Duke criteria, and the vegetations comparison table are direct exam favourites. Understanding why a damaged valve is the substrate for endocarditis — and why strep and staph cause entirely different pictures — gives you the clinical framework to risk-stratify, diagnose, and refer appropriately.
RECALL
Before proceeding, recall:
• Group-A β-haemolytic Streptococcus (Streptococcus pyogenes) and its M-protein antigenicity
• Type II hypersensitivity — antibody-mediated cytotoxicity (antigen–antibody on cell surface → complement + macrophage attack)
• Basic cardiac anatomy: endocardium, myocardium, pericardium; location and function of mitral, aortic, tricuspid, and pulmonary valves
• Concept of valvular stenosis vs. regurgitation and their haemodynamic consequences
• From Year-1 Microbiology: streptococcal M-protein, ASO titre, throat culture
If any of these feel shaky, spend 5 minutes with your Year-1 notes before continuing — the pathogenesis section will make far more sense.
Acute Rheumatic Fever — Etiology and Epidemiology
Acute Rheumatic Fever: Etiology and Epidemiology
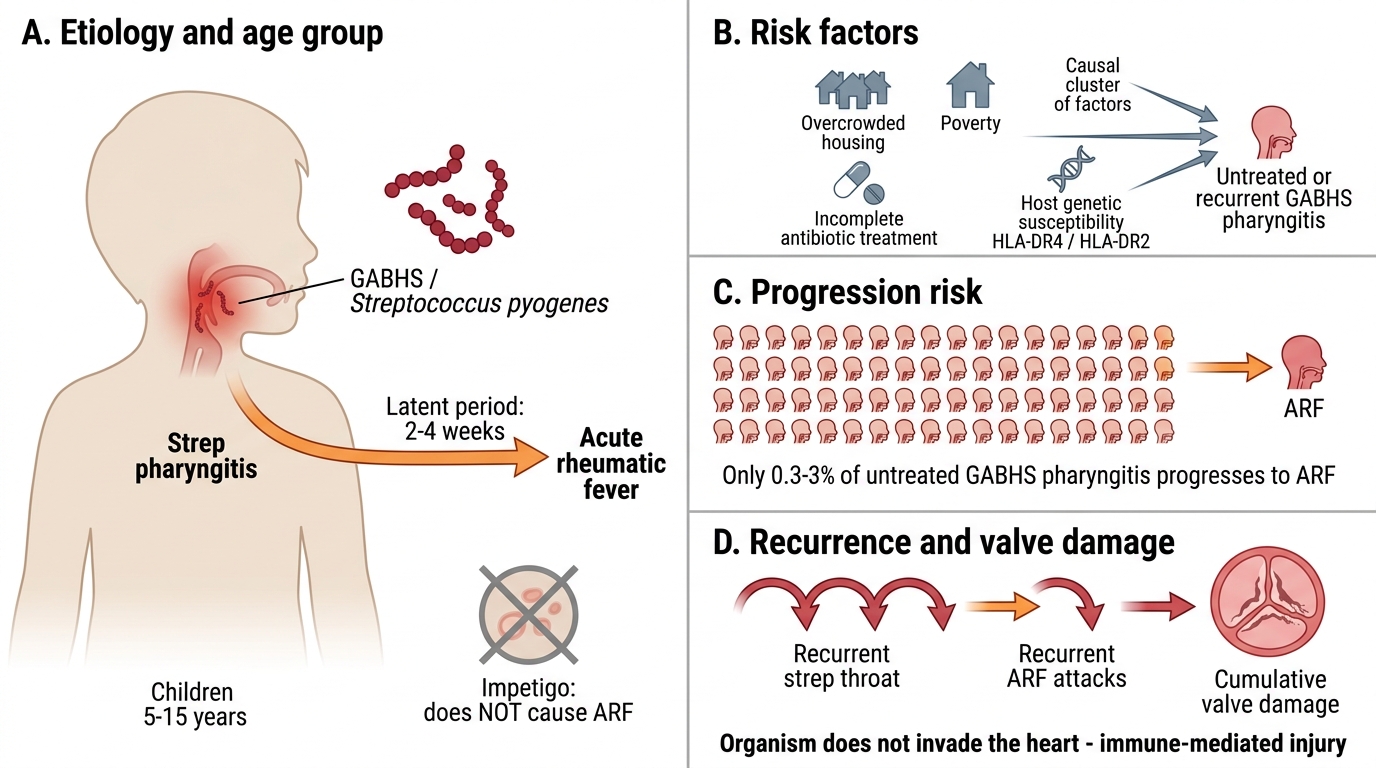
Acute rheumatic fever (ARF) is a systemic inflammatory disease that follows pharyngeal infection (not skin infection) with group-A β-haemolytic Streptococcus (GABHS), Streptococcus pyogenes. It affects children aged 5–15 years most commonly; the latent period between strep pharyngitis and ARF is 2–4 weeks.
Key epidemiological points:
• ARF does NOT follow streptococcal skin infection (impetigo) — the pharyngeal mucosal immune response is required
• Only 0.3–3% of untreated GABHS pharyngitis cases progress to ARF — host genetic susceptibility (HLA-DR4, DR2) plays a role
• Overcrowding, poverty, and inadequate antibiotic treatment are major risk factors
• Recurrent strep throat infections cause recurrent ARF attacks with cumulative valve damage
The organism itself never invades the heart — the damage is entirely immune-mediated.
Pathogenesis of Acute Rheumatic Fever — Molecular Mimicry
Molecular Mimicry in Acute Rheumatic Fever
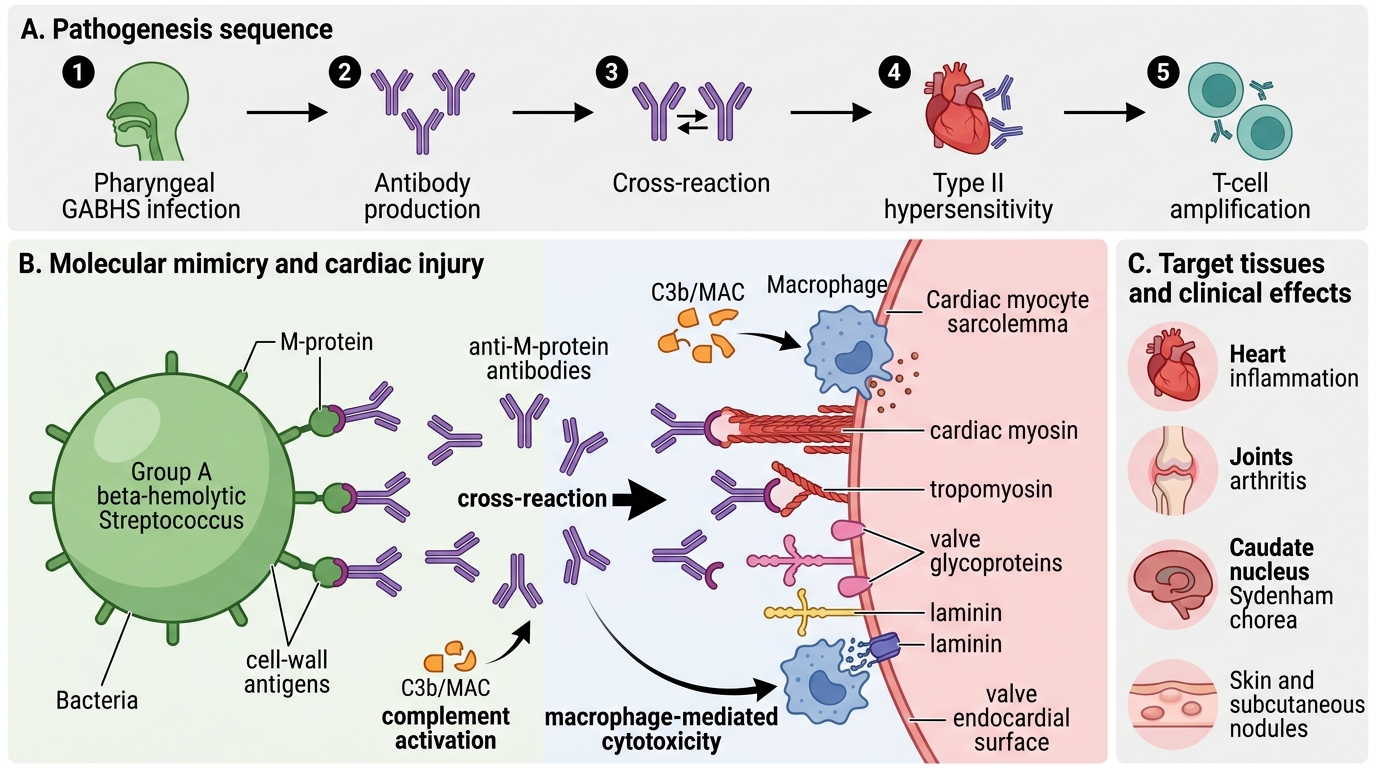
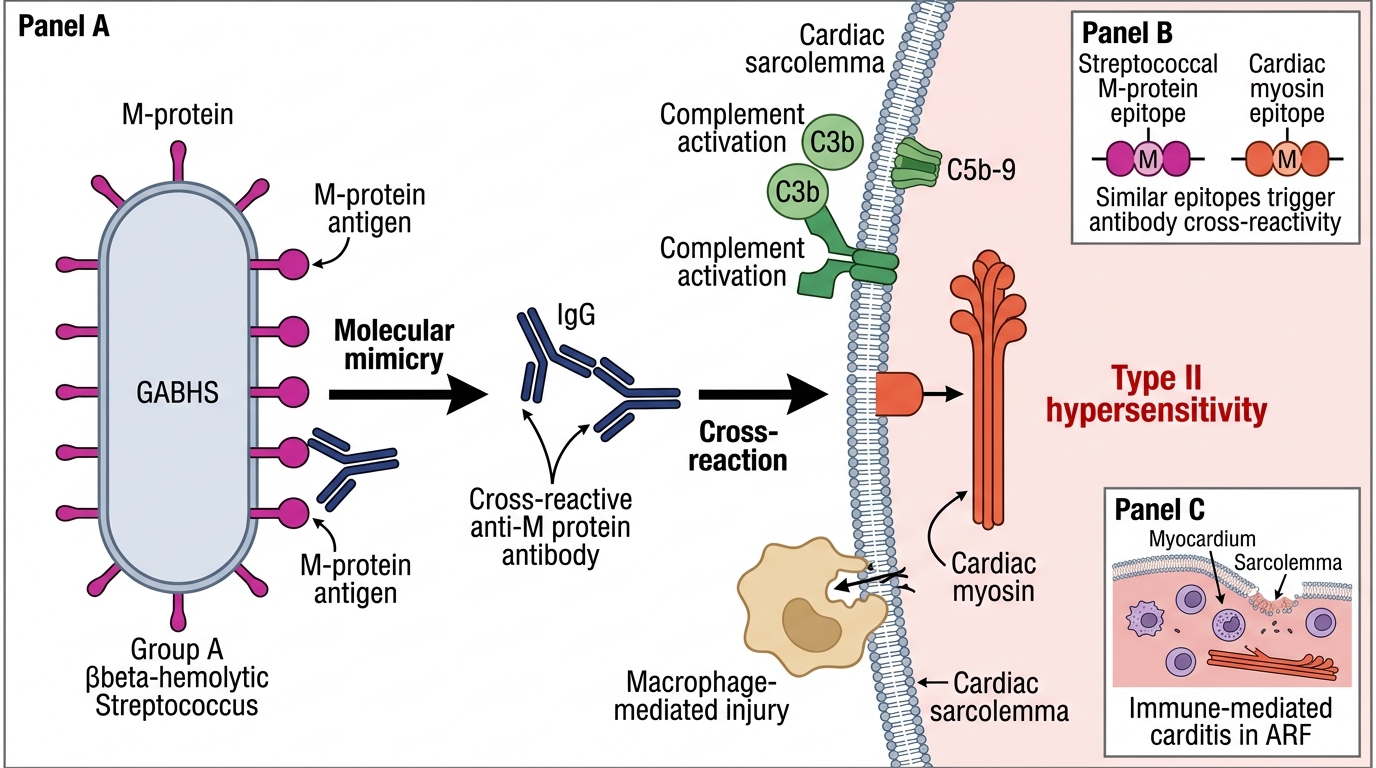
The pathogenesis of ARF is the classic example of molecular mimicry — a mechanism by which an immune response directed against a pathogen cross-reacts with self-antigens.
Step 1 — Streptococcal infection: GABHS M-protein and other cell-wall antigens (N-acetyl glucosamine, hyaluronate) are presented to the pharyngeal immune system.
Step 2 — Antibody production: The host generates antibodies directed against M-protein epitopes.
Step 3 — Cross-reaction: These antibodies structurally resemble epitopes on:
• Cardiac myosin and tropomyosin (myocarditis)
• Valve glycoproteins and laminin (endocarditis)
• Neuronal antigens in the caudate nucleus (Sydenham chorea)
• Synovial antigens (arthritis)
Step 4 — Type II hypersensitivity: Antibodies bind to self-antigens on cardiac tissue → complement activation and macrophage-mediated cytotoxicity → inflammation.
Step 5 — T-cell amplification: CD4⁺ T cells infiltrate cardiac tissue and mount a delayed hypersensitivity (Type IV) response, amplifying tissue damage.
The result: a non-suppurative inflammatory process affecting heart, joints, brain, skin, and subcutaneous tissue — driven entirely by the immune system, not by bacterial invasion.
Molecular Mimicry in Acute Rheumatic Fever
Jones Criteria for Diagnosis of Acute Rheumatic Fever
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Jones Criteria for Acute Rheumatic Fever
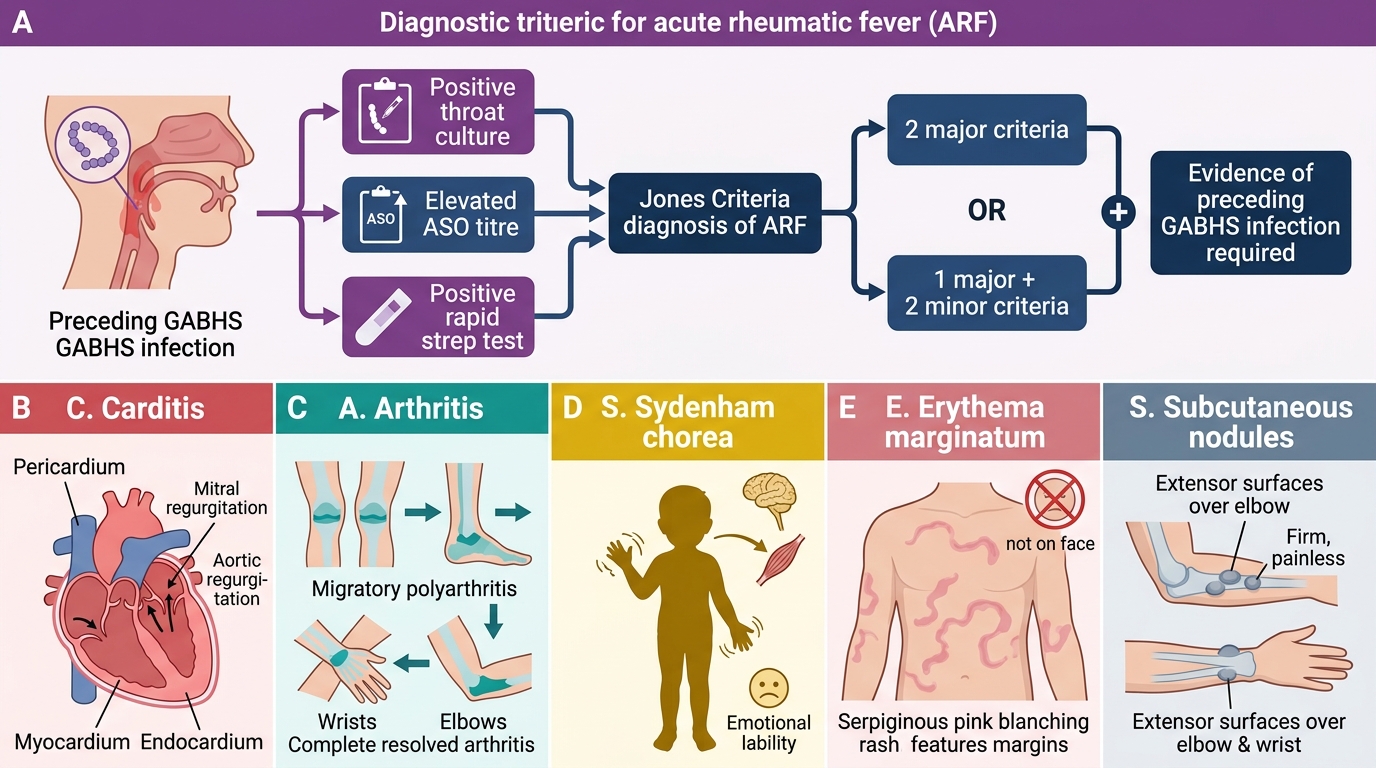
The Jones criteria (updated 2015, AHA) provide the diagnostic framework for ARF. Diagnosis requires 2 major, or 1 major + 2 minor criteria, PLUS evidence of preceding GABHS infection (positive throat culture, elevated ASO titre, or positive rapid strep test).
MAJOR criteria (mnemonic: CASES):
| Criterion | Details |
|---|---|
| Carditis | Pancarditis — pericarditis, myocarditis, endocarditis; new murmur (mitral/aortic regurgitation most common); subclinical carditis detectable by echo |
| Arthritis | Migratory polyarthritis — large joints (knees, ankles, wrists, elbows) in sequence; exquisitely painful; resolves completely; does NOT cause permanent joint damage |
| Sydenham chorea | Involuntary, purposeless movements; emotional lability; late manifestation (months after strep); may be only sign |
| Erythema marginatum | Fleeting, non-pruritic rash on trunk; serpiginous pink margins; blanches on pressure; NOT on face |
| Subcutaneous nodules | Firm, painless, pea-sized nodules over bony prominences (elbows, knees, scalp); associated with severe carditis |
MINOR criteria: Fever, elevated ESR/CRP, prolonged PR interval on ECG, arthralgia (only if arthritis not already counted as major).
Carditis is the most dangerous major criterion because it causes permanent valve damage; the other manifestations resolve completely.
SELF-CHECK
A 12-year-old boy has fleeting joint pains moving from his right knee to his left ankle, fever, and a new mid-systolic murmur 3 weeks after a sore throat. His ASO titre is markedly elevated. His ECG shows a PR interval of 0.24 seconds. How many major Jones criteria does he satisfy?
A. One (carditis only)
B. Two (carditis + arthritis)
C. Three (carditis + arthritis + prolonged PR)
D. One (arthritis only — murmur may be functional)
Reveal Answer
Answer: B. Two (carditis + arthritis)
He satisfies TWO major criteria: carditis (new murmur — the murmur of mitral regurgitation is the earliest sign of carditis) and migratory polyarthritis (fleeting, moves from joint to joint). A prolonged PR interval is a MINOR criterion (ECG change), not a major one. With 2 major criteria + elevated ASO titre (evidence of preceding strep), the diagnosis of acute rheumatic fever is established.