Page 16 of 34
PA26.{5,7} | Rheumatic Heart Disease & Infective Endocarditis — SDL Guide (Part 2)
Pancarditis — Pathology of Acute Rheumatic Heart Disease
Acute Rheumatic Pancarditis
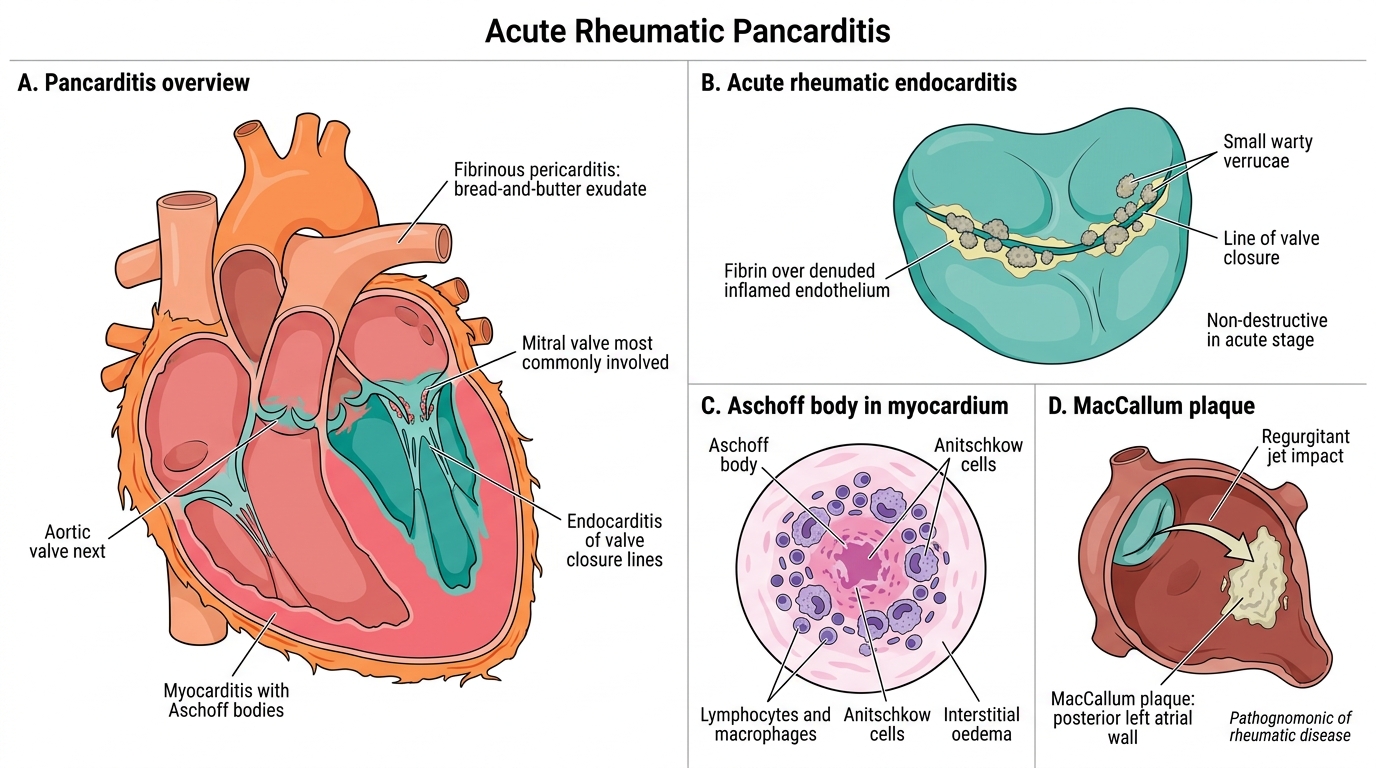
ARF causes pancarditis — inflammation of all three layers of the heart. The endocarditis component causes the clinically significant lasting damage.
Pericarditis:
• Fibrinous or serofibrinous exudate — 'bread-and-butter' appearance on gross examination
• Resolves completely; rarely progresses to constrictive pericarditis
Myocarditis:
• Pathognomonic lesion: the Aschoff body
• Interstitial oedema and Aschoff bodies throughout myocardium
Endocarditis:
• Small, warty verrucae (1–2 mm) along the lines of valve closure — most commonly the mitral valve, followed by the aortic valve
• Verrucae represent areas of fibrin deposition over inflamed, denuded endothelium
• These are NOT destructive at this stage — but they set the stage for chronic scarring
MacCallum's plaque: Irregular roughened plaque on the posterior left atrial wall at the jet-stream impact zone of mitral regurgitation — formed by organisation of endocardial inflammation; pathognomonic of rheumatic disease
Remember: in ARF, the inflammation is exudative and reversible in pericardium and joints, but the endocardial and myocardial changes set in motion a chronic fibrotic process in the valves.
The Aschoff Body — Pathognomonic Lesion of Rheumatic Fever
Aschoff Body in Rheumatic Myocarditis
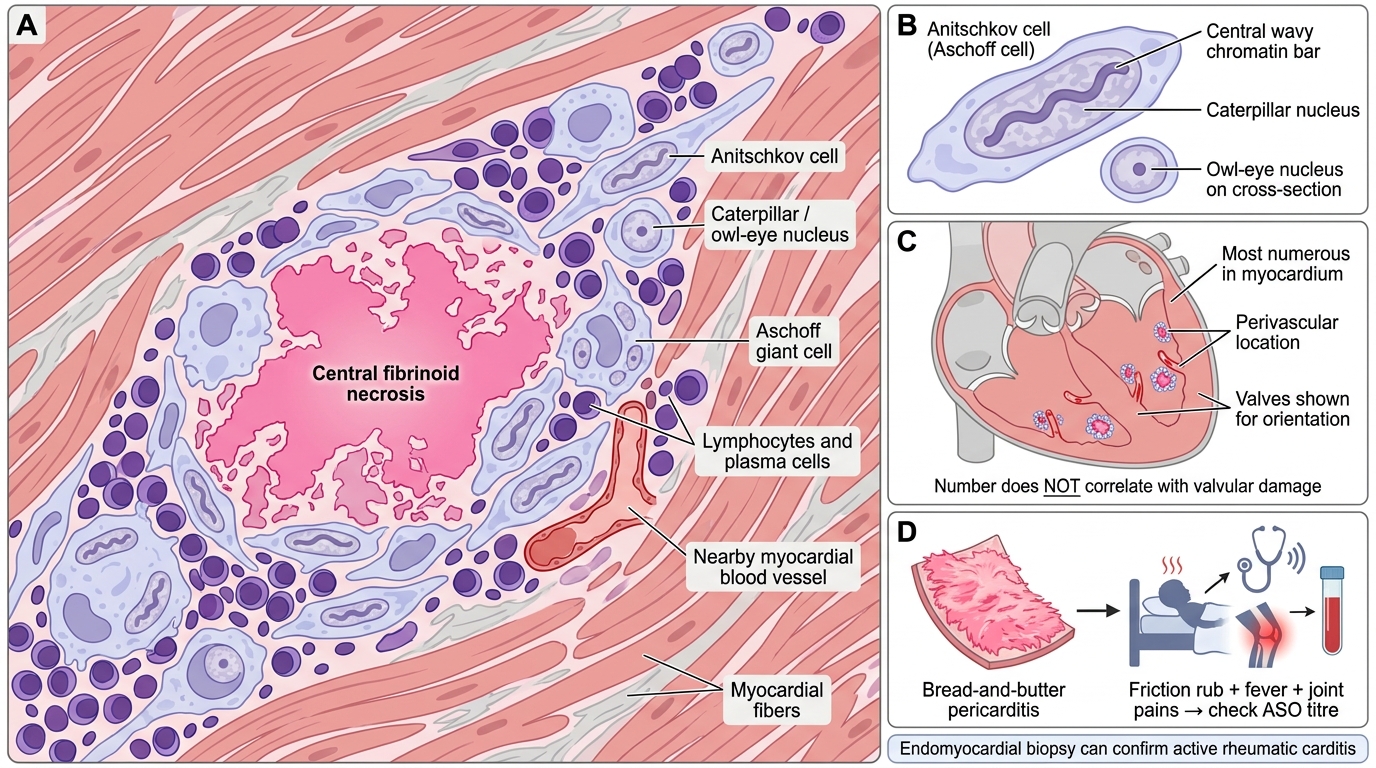
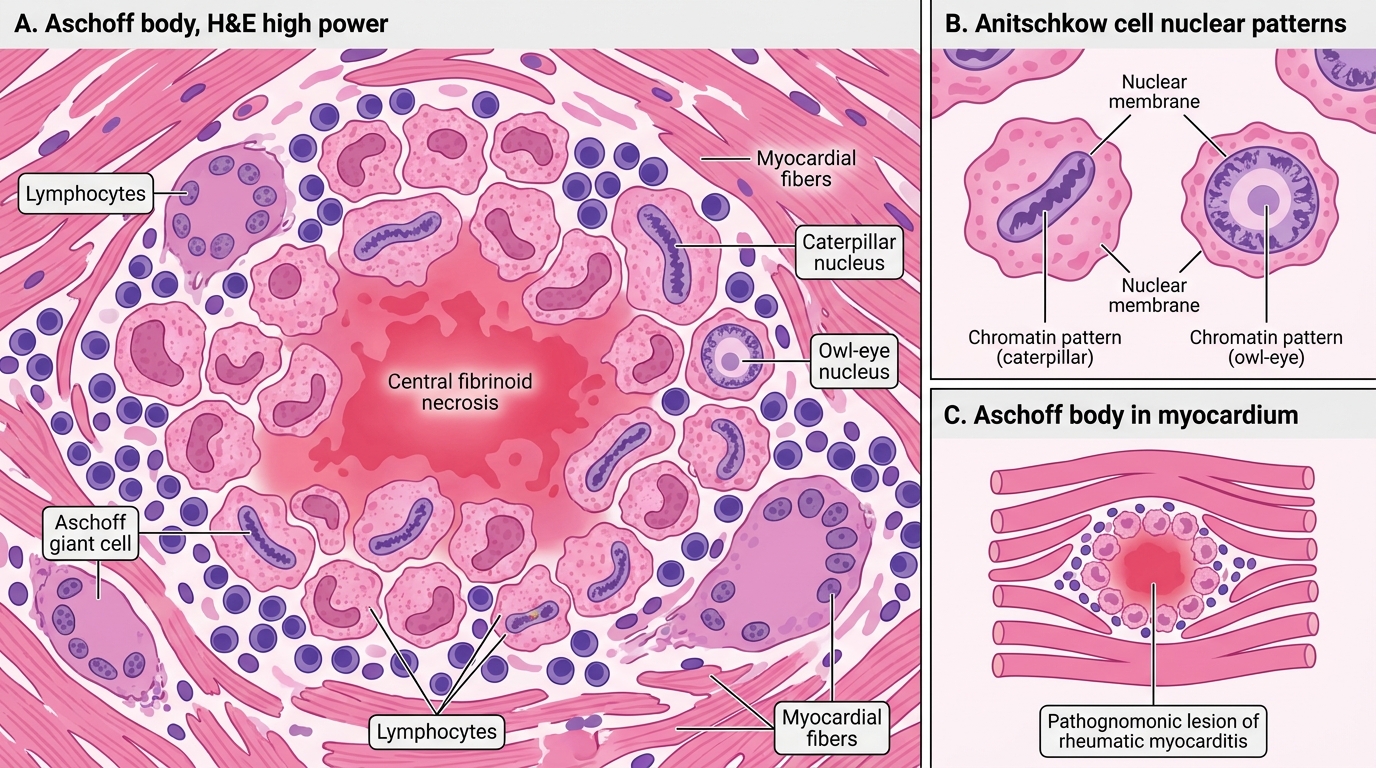
The Aschoff body is the hallmark microscopic lesion of rheumatic myocarditis. It is a granuloma-like lesion consisting of:
- Central zone of fibrinoid necrosis — eosinophilic, amorphous material (denatured collagen + fibrin)
- Anitschkov cells (also called Aschoff cells): large, activated macrophages with a characteristic nucleus — the chromatin is arranged in a central wavy bar resembling a caterpillar (owl-eye or caterpillar nucleus on cross-section). These are pathognomonic — no other disease produces them.
- Aschoff giant cells: multinucleate forms of Anitschkov cells
- Peripheral lymphocytes and plasma cells
Aschoff bodies are most numerous in the myocardium, particularly around blood vessels. They heal by fibrosis over months to years, leaving small scars.
Clinical correlate: Because Aschoff bodies are in the myocardium (not valves), their number does NOT correlate with the degree of valvular damage. Endomyocardial biopsy can confirm active rheumatic carditis even years after the initial episode.
Aschoff Body in Acute Rheumatic Myocarditis
CLINICAL PEARL
The 'bread-and-butter' pericarditis of ARF is a clinical red flag — friction rub on auscultation in a child with fever and joint pains should prompt immediate ASO titre and throat culture. Do not dismiss it as viral — the pericarditis itself resolves, but the concurrent endocarditis is silently starting the valve's 20-year journey to stenosis.
Chronic Rheumatic Heart Disease — Mitral Stenosis
Chronic Rheumatic Mitral Stenosis
Repeated episodes of ARF cause cumulative valve scarring, leading to chronic rheumatic heart disease (CRHD). The mitral valve is affected in >90% of cases; isolated mitral stenosis accounts for ~25% of all valvular disease.
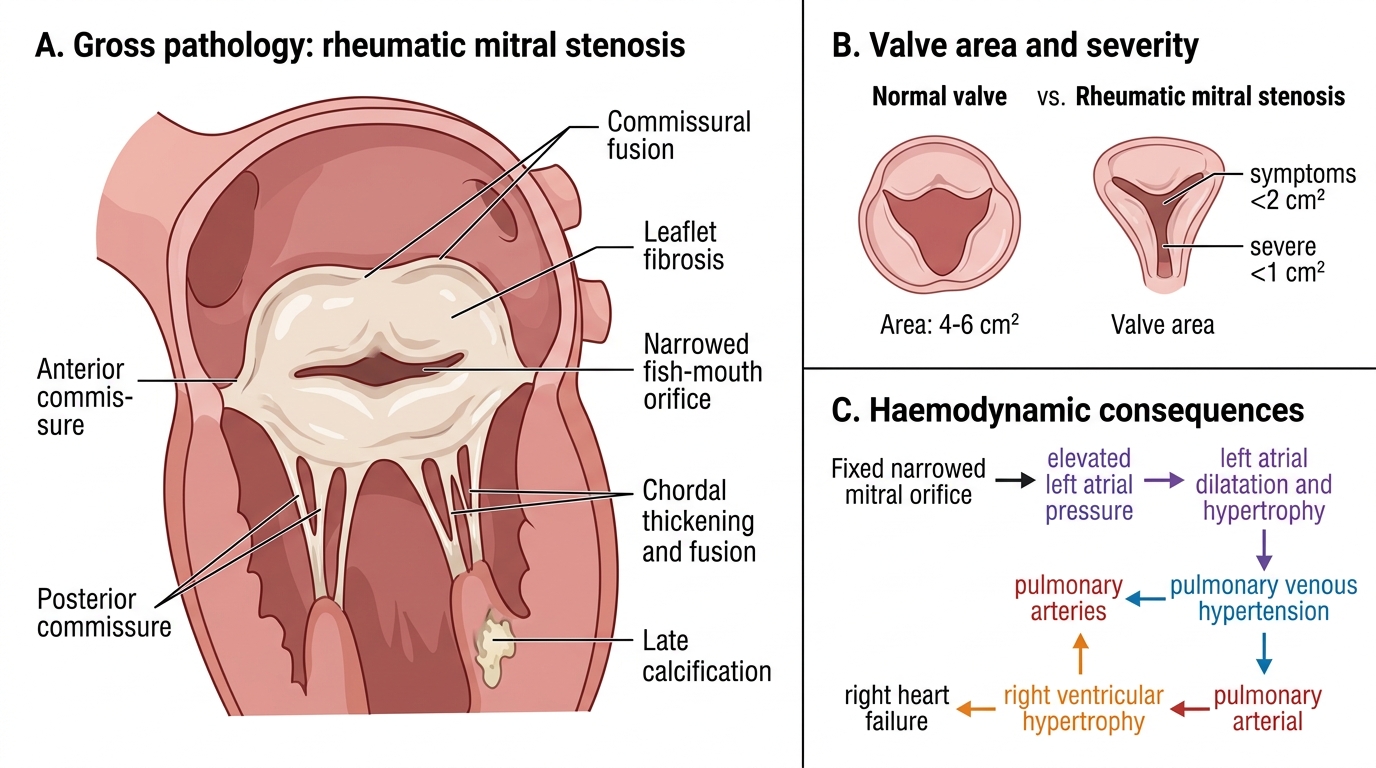
Gross pathology of rheumatic mitral stenosis:
• Leaflet thickening and fibrosis — due to repeated fibrin deposition and organisation
• Commissural fusion — the leaflet edges fuse along the anterior and posterior commissures, narrowing the orifice
• Chordae tendineae thickening and fusion — the subvalvular apparatus is pulled into the ventricle
• Calcification — late feature; reduces leaflet mobility further
• The result: a fixed, narrowed orifice with the characteristic 'fish-mouth' or 'buttonhole' appearance on gross examination
Normal mitral valve area: 4–6 cm². Symptoms begin when area falls below 2 cm²; severe stenosis: <1 cm².
Haemodynamic consequences:
• Elevated left atrial pressure → left atrial dilatation and hypertrophy
• Pulmonary venous hypertension → breathlessness, orthopnoea, PND
• Progressive pulmonary arterial hypertension → right ventricular hypertrophy and failure
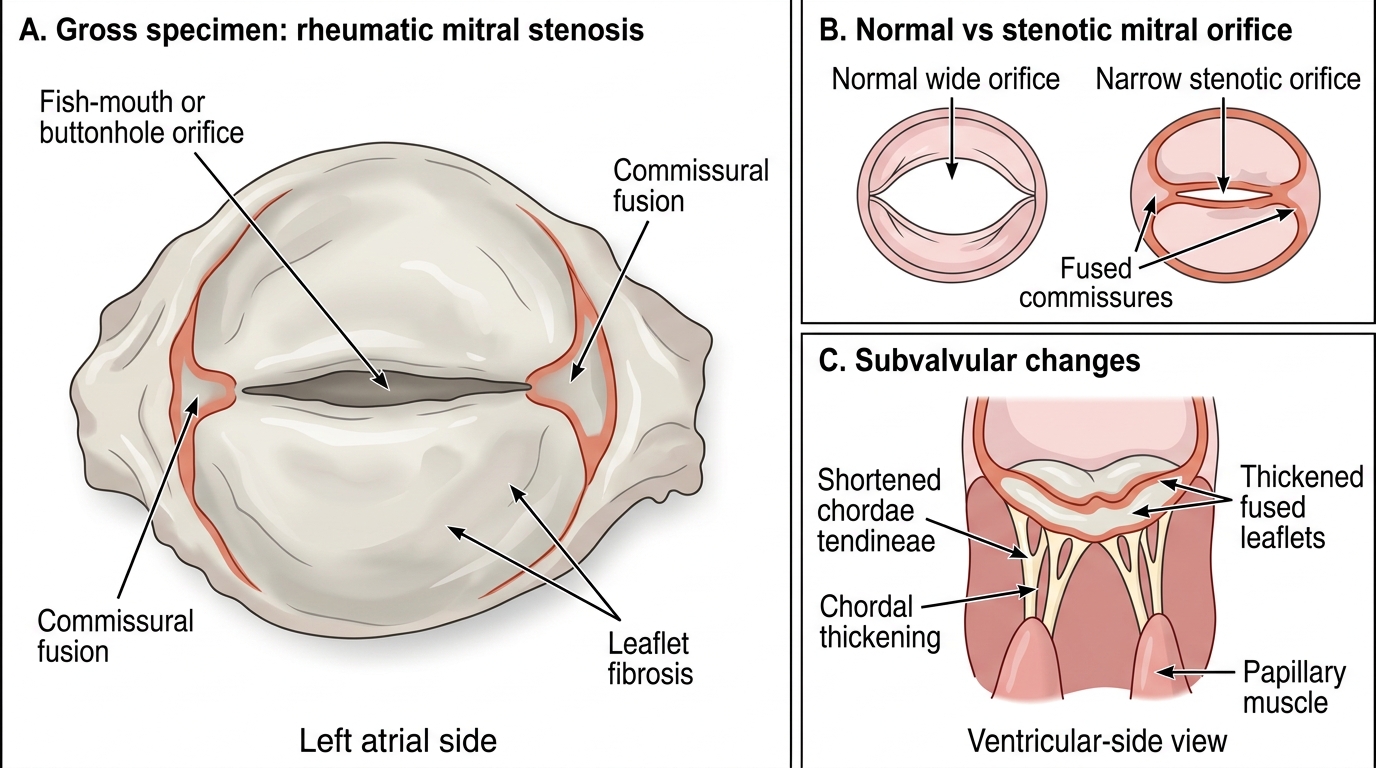
Rheumatic Mitral Stenosis: Gross Morphology