Page 17 of 34
PA26.{5,7} | Rheumatic Heart Disease & Infective Endocarditis — SDL Guide (Part 3)
Complications of Chronic Rheumatic Heart Disease
Complications of Chronic Rheumatic Heart Disease
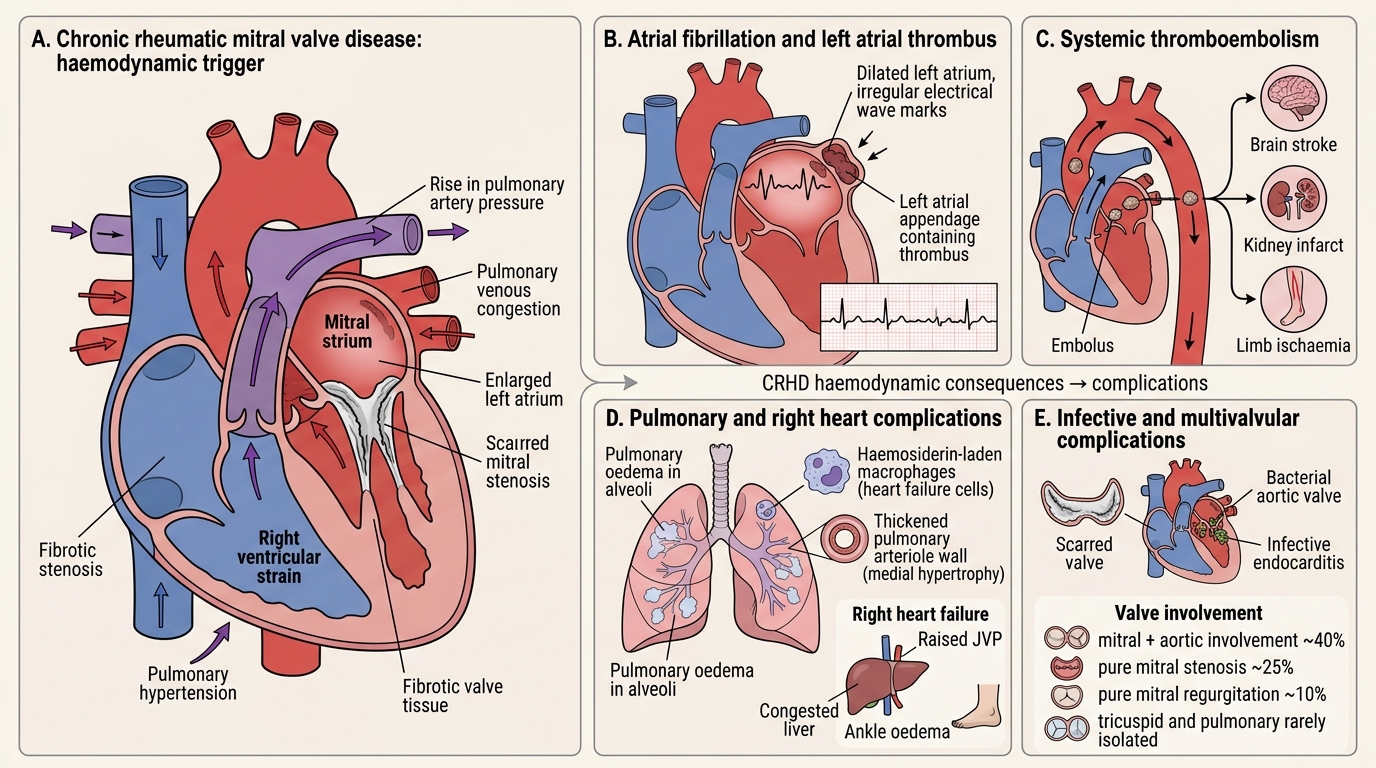
CRHD and its haemodynamic consequences lead to a cascade of complications:
Cardiac complications:
• Atrial fibrillation (AF): Left atrial dilatation from chronic pressure overload → electrical remodelling → AF. Occurs in ~40% of mitral stenosis patients. AF dramatically worsens haemodynamics (loss of atrial kick + fast rate).
• Right heart failure: Progressive pulmonary hypertension → right ventricular pressure overload → right heart failure (raised JVP, hepatomegaly, peripheral oedema)
Thromboembolic complications:
• Left atrial thrombus (especially in the left atrial appendage) in AF → systemic embolism → stroke, renal infarct, limb ischaemia
• Risk especially high when AF is present
Infective complications:
• Damaged, scarred valves provide a substrate for bacterial colonisation → infective endocarditis (IE) superimposed on CRHD — covered in the second half of this module
Lung complications:
• Pulmonary venous hypertension → pulmonary oedema (acute) and pulmonary haemosiderosis (chronic — 'heart failure cells' — haemosiderin-laden macrophages in sputum)
• Pulmonary arterial changes — medial hypertrophy → fixed pulmonary hypertension
Other valves:
• Mitral + aortic involvement in ~40%; pure mitral stenosis ~25%; pure mitral regurgitation ~10%; tricuspid and pulmonary rarely isolated
SELF-CHECK
A 38-year-old woman with known rheumatic mitral stenosis presents with sudden onset right-sided weakness and dysphasia. Her pulse is irregularly irregular. Which mechanism best explains her neurological deficit?
A. Embolic stroke from left atrial thrombus in the context of atrial fibrillation
B. Haemorrhagic stroke due to pulmonary hypertension
C. Septic embolism from infective endocarditis vegetations
D. Vasospasm from elevated left atrial pressure
Reveal Answer
Answer: A. Embolic stroke from left atrial thrombus in the context of atrial fibrillation
The irregularly irregular pulse indicates atrial fibrillation, a direct complication of chronic mitral stenosis from left atrial dilatation. AF causes stasis of blood in the left atrial appendage → thrombus formation → systemic thromboembolism — in this case, a cardioembolic stroke. Septic embolism (option C) would require features of infective endocarditis (fever, new murmur change, positive blood cultures) — not mentioned here.
Infective Endocarditis — Classification and Etiology
Infective Endocarditis: Classification and Etiology
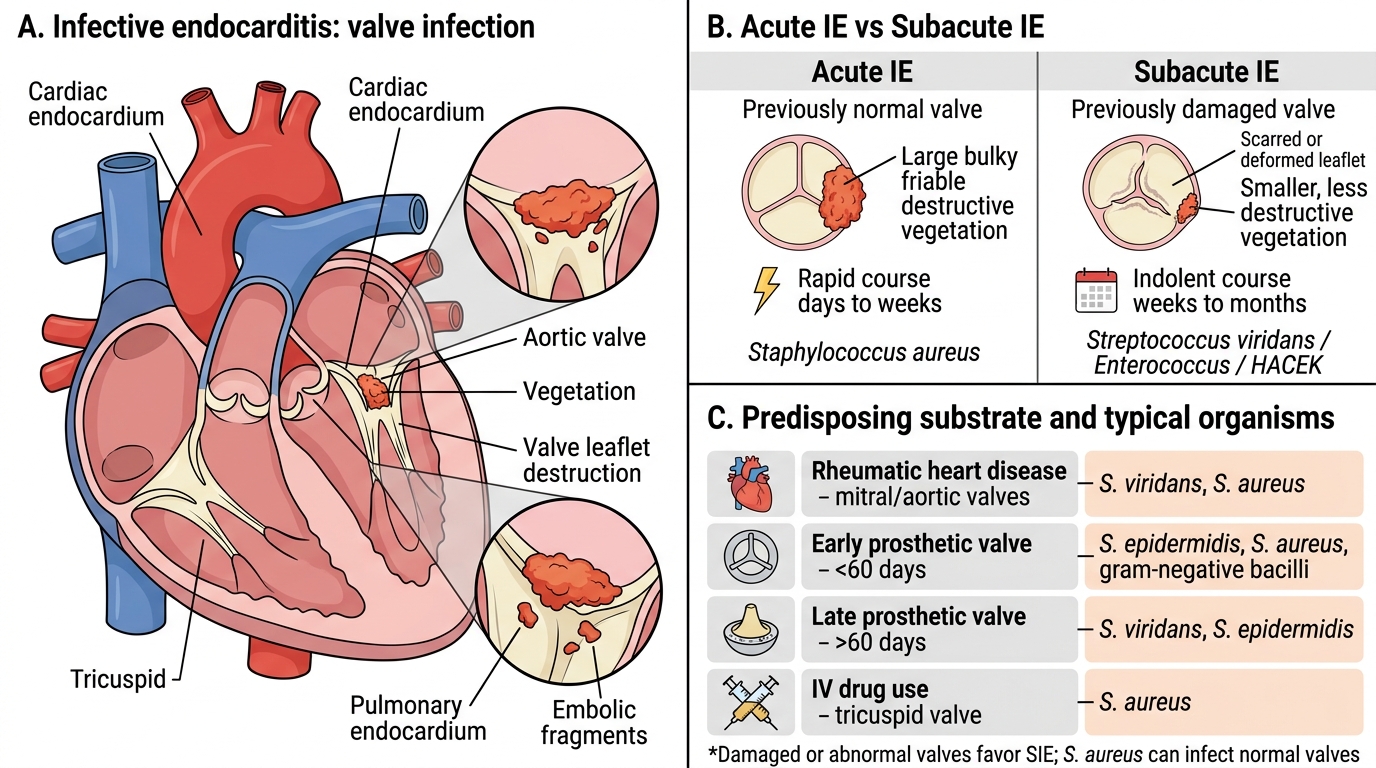
Infective endocarditis (IE) is an infection of the cardiac endocardium, predominantly affecting heart valves. It is classified by clinical course and causative organism:
Acute IE (AIE):
• Caused by highly virulent organisms — Staphylococcus aureus most common (~50% of all IE)
• Attacks previously normal valves — does not need prior damage
• Rapid, destructive course — days to weeks
• Produces large, bulky, friable, destructive vegetations
• High mortality without rapid treatment
Subacute IE (SIE):
• Caused by low-virulence organisms — Streptococcus viridans (oral flora, ~30% of IE), Enterococcus, HACEK organisms
• Almost always attacks previously damaged or abnormal valves (RHD, bicuspid aortic valve, prosthetic valve, congenital defects)
• Indolent course — weeks to months; constitutional symptoms dominate early
• Produces smaller, less destructive vegetations but with equal embolism risk
Predisposing conditions:
| Substrate | Typical organism |
|---|---|
| Rheumatic heart disease (mitral/aortic) | S. viridans, S. aureus |
| Prosthetic valve (early <60 days) | S. epidermidis, S. aureus, gram-negatives |
| Prosthetic valve (late >60 days) | S. viridans, S. epidermidis |
| IV drug use | S. aureus → right-sided, tricuspid valve |
| Congenital heart disease | S. viridans, S. aureus |
| No predisposing cause | S. aureus (community-acquired) |
Pathology of Infective Endocarditis — Vegetations
Infective Endocarditis Vegetations
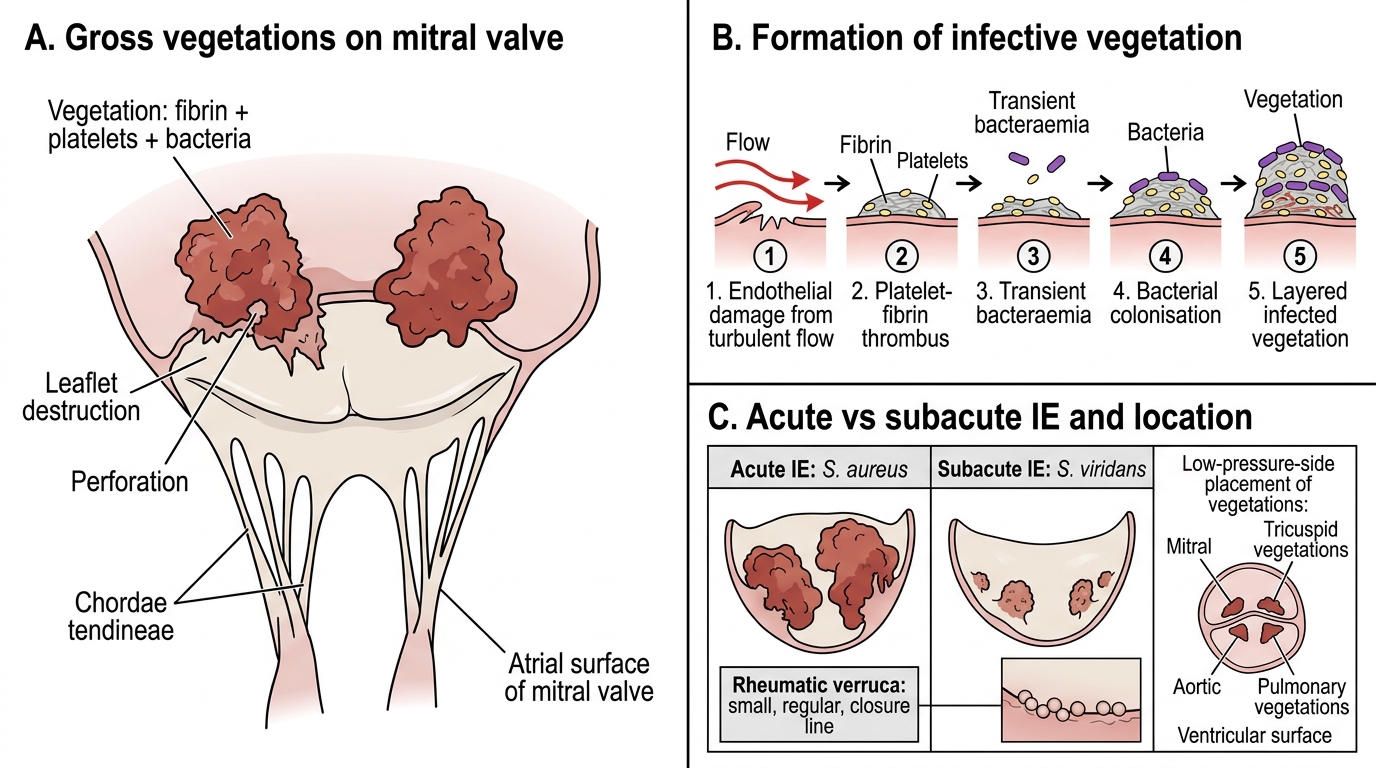
The hallmark lesion of IE is the vegetation — a mass of thrombotic material colonised by microorganisms on the valve surface.
How vegetations form:
1. Turbulent flow or direct injury creates a focus of endothelial damage
2. Platelet-fibrin thrombus forms on the denuded surface (as in NBTE)
3. Transient bacteraemia delivers organisms to the thrombus
4. Bacteria adhere, colonise, and proliferate within the fibrin-platelet matrix
5. Further layers of fibrin and platelets deposit over the infected nidus
6. Result: a complex mass of fibrin, platelets, bacteria, inflammatory cells, and necrotic debris
Gross features of IE vegetations:
• Acute IE (S. aureus): Large (up to several cm), irregular, bulky, friable, destructive — erode into the valve leaflet, cause perforation and rupture; may extend into surrounding structures (annulus, myocardium, conduction system)
• Subacute IE (S. viridans): Smaller, 'wart-like', less destructive — but still friable and prone to embolism
• Location: Most commonly on the atrial surface of the mitral/tricuspid valve and the ventricular surface of the aortic/pulmonary valve (i.e., at the low-pressure side of the jet stream)
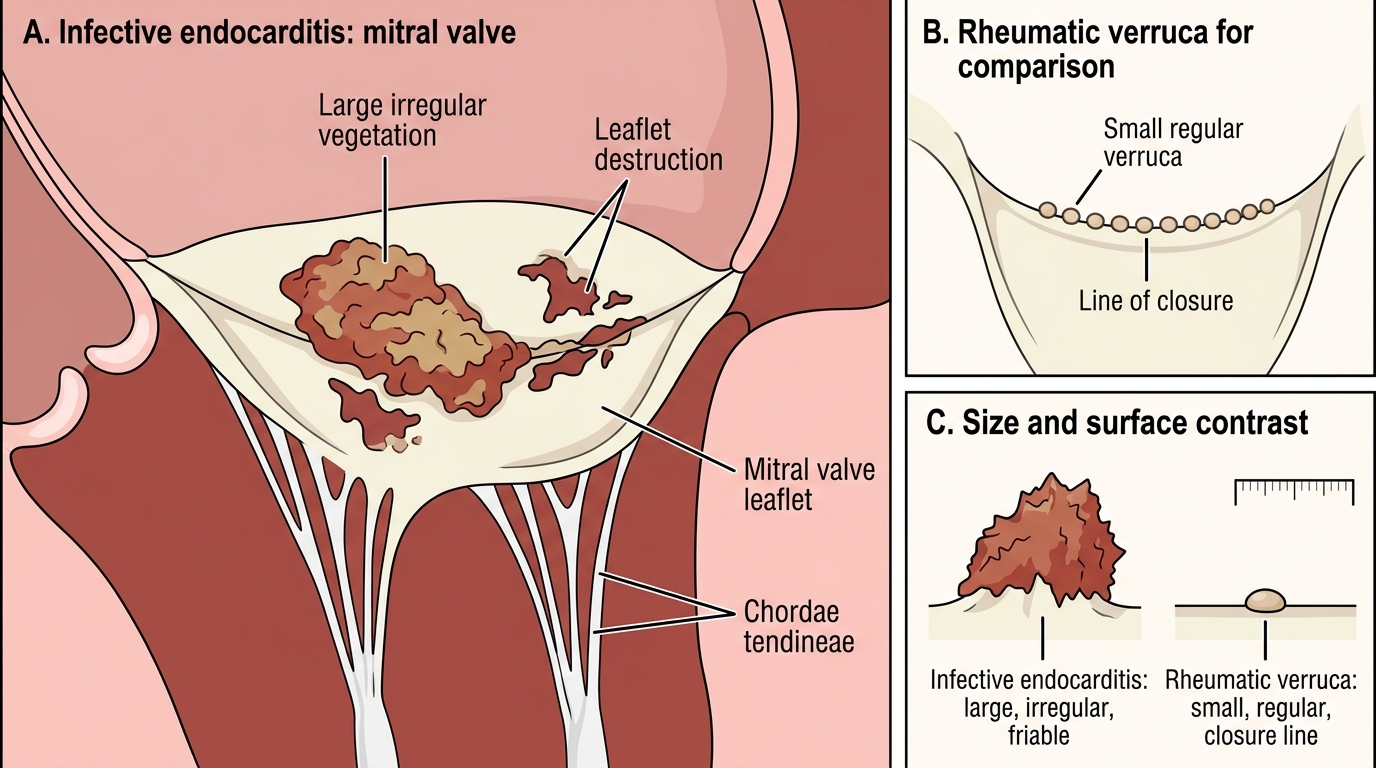
Mitral Valve Vegetations: Infective Endocarditis vs Rheumatic Verruca