Page 18 of 34
PA26.{5,7} | Rheumatic Heart Disease & Infective Endocarditis — SDL Guide (Part 4)
Duke Criteria — Clinical Diagnosis of Infective Endocarditis
Modified Duke Criteria for Infective Endocarditis
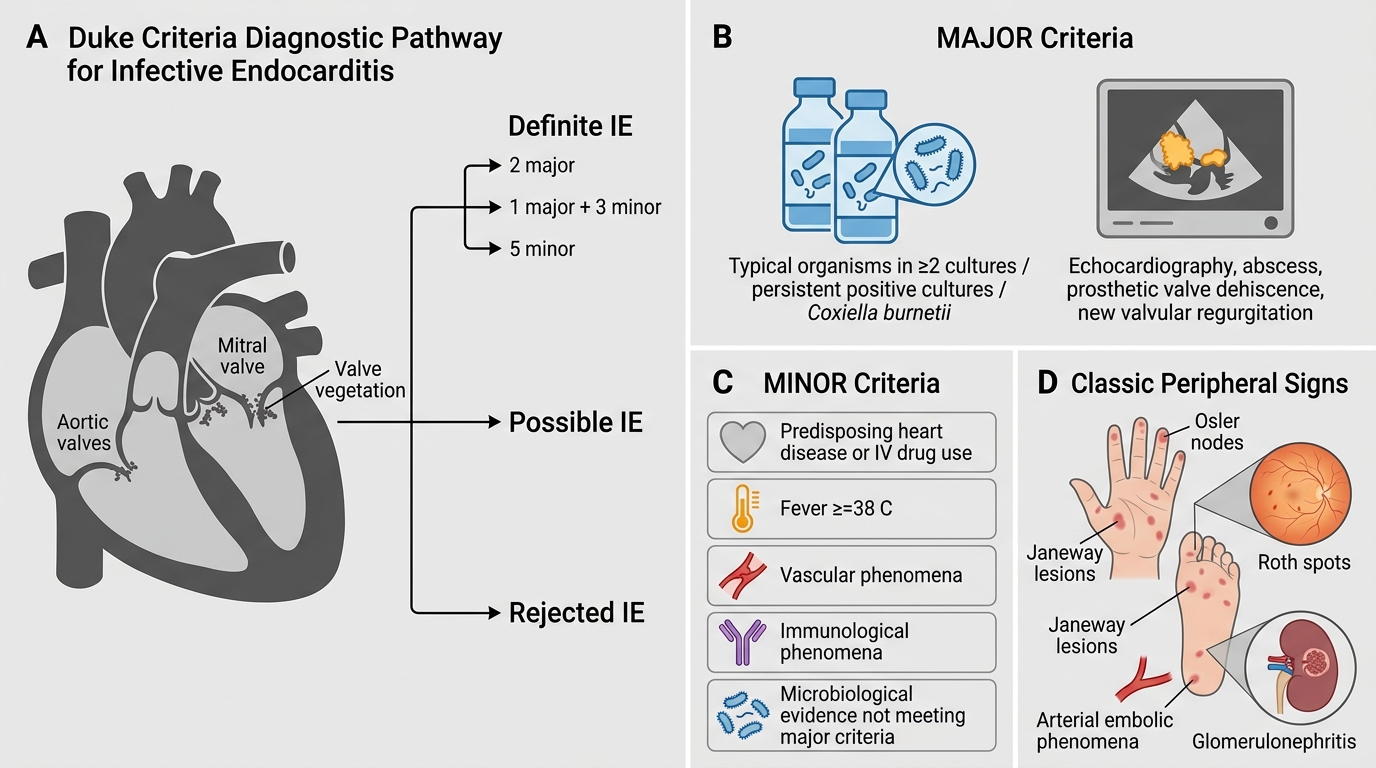
The Duke criteria (modified 2000) stratify patients as definite, possible, or rejected IE using major and minor criteria.
Definite IE = 2 major, OR 1 major + 3 minor, OR 5 minor criteria
MAJOR criteria:
1. Positive blood culture: Typical organism (S. viridans, S. bovis, HACEK, S. aureus, or Enterococcus) in ≥2 separate cultures, OR persistently positive blood cultures ≥12 hours apart, OR single positive for Coxiella burnetii
2. Positive echocardiogram: Vegetation, abscess, or new partial dehiscence of prosthetic valve, OR new valvular regurgitation (worsening of pre-existing murmur is NOT sufficient)
MINOR criteria:
• Predisposing heart condition or IV drug use
• Fever ≥38°C
• Vascular phenomena (arterial emboli, septic pulmonary infarcts, mycotic aneurysm, Janeway lesions)
• Immunological phenomena (glomerulonephritis, Osler's nodes, Roth spots, positive rheumatoid factor)
• Microbiological evidence not meeting major criteria
Classic peripheral signs (vascular/immune):
| Sign | Nature | Location |
|---|---|---|
| Janeway lesions | Non-tender, haemorrhagic macules — septic microemboli | Palms, soles |
| Osler's nodes | Tender, painful subcutaneous nodules — immune complex deposition | Fingertips, toe pads |
| Roth spots | Retinal haemorrhages with white centres | Fundus |
| Splinter haemorrhages | Linear haemorrhages — microemboli in nail-bed capillaries | Fingernails |
Memory trick: Janeway is non-tender because it is embolic (vascular); Osler is tender because it is immune-mediated (immunological).
SELF-CHECK
A 28-year-old IV drug user presents with 3 weeks of fever, night sweats, and a new tricuspid regurgitation murmur. Blood cultures grow S. aureus in 3/3 bottles. Echo shows a 12 mm mobile vegetation on the tricuspid valve. Using modified Duke criteria, this case is classified as:
A. Possible IE — only 1 major criterion (vegetation) is present
B. Definite IE — 2 major criteria (positive blood culture + vegetation on echo)
C. Possible IE — S. aureus requires 2 separate culture draws to count
D. Definite IE — 1 major (vegetation) + 3 minor criteria are met
Reveal Answer
Answer: B. Definite IE — 2 major criteria (positive blood culture + vegetation on echo)
This patient has TWO major Duke criteria: (1) Positive blood culture — S. aureus in ≥2 separate cultures satisfies the microbiological major criterion; (2) Positive echocardiogram — vegetation on the tricuspid valve. Two major criteria = Definite IE by modified Duke criteria. IV drug use (minor criterion) and fever (minor criterion) are additional supporting evidence, but the two major criteria alone establish the diagnosis.
Complications of Infective Endocarditis
Complications of Infective Endocarditis
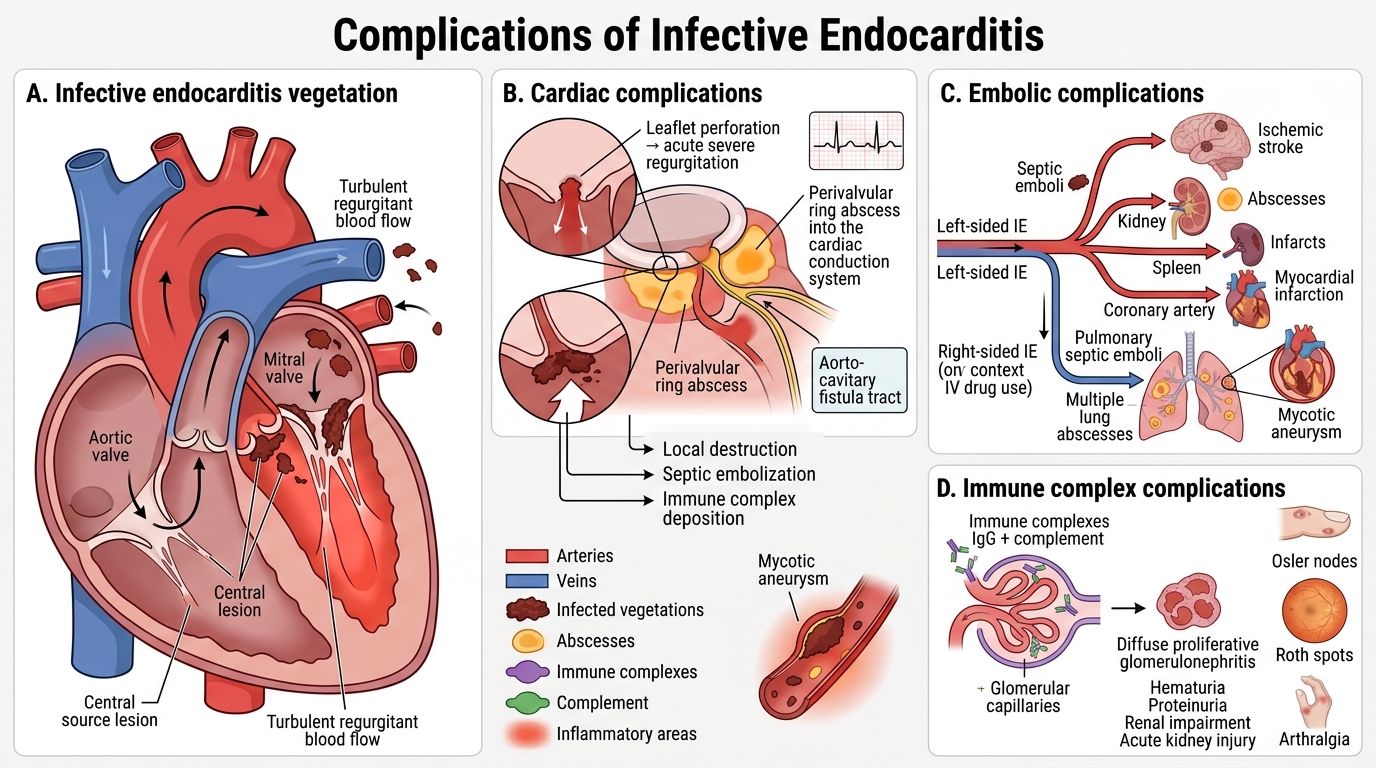
IE complications are grouped by mechanism:
Cardiac complications (local destruction):
• Valvular regurgitation — the commonest acute complication; vegetation erodes or perforates the leaflet; acute severe regurgitation → acute left heart failure
• Ring abscess (perivalvular abscess) — S. aureus spreads into the valve annulus; can involve the conduction system → new heart block
• Fistula formation — e.g., aorto-cavitary fistula
• Pericarditis — haematogenous spread or direct extension
Embolic complications:
• Friable vegetations fragment → septic emboli travel in the bloodstream
• Left-sided IE → systemic emboli: brain (ischaemic stroke, cerebral abscess), kidney (renal abscess, infarct), spleen (splenic abscess), coronary arteries (myocardial infarction)
• Right-sided IE (IV drug users) → pulmonary septic emboli → multiple lung abscesses
• Mycotic aneurysm — septic embolus lodges in vessel wall → local infection → aneurysmal dilatation → rupture risk
Immune complex complications:
• Diffuse proliferative glomerulonephritis — immune complex (IgG + complement) deposition in glomeruli → haematuria, proteinuria, renal impairment; can cause acute kidney injury
• Osler's nodes, Roth spots, and arthralgia — immune complex vasculitis
Vegetations Comparison Table — The Big Picture
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
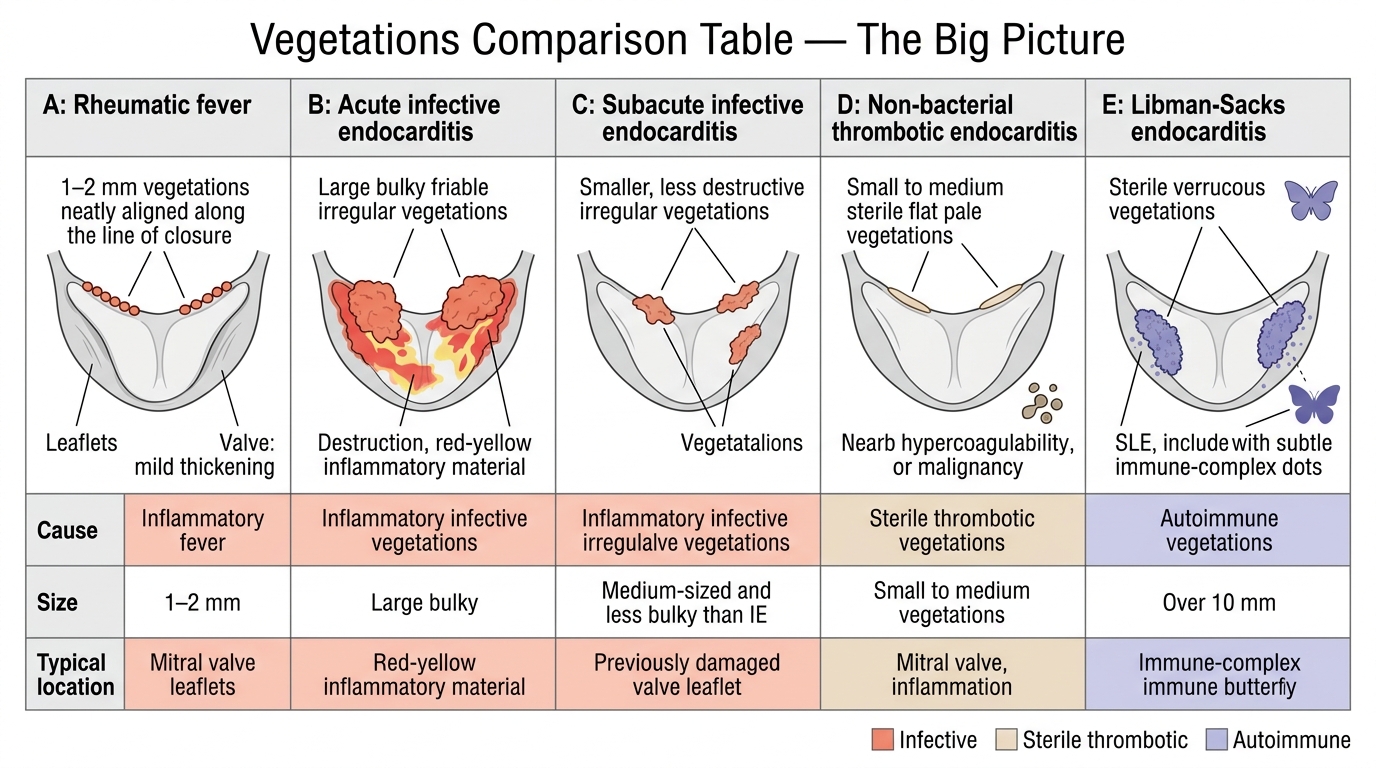
Major Types of Cardiac Vegetations
Comparing vegetation types across conditions is a favourite exam question and essential for differential diagnosis:
| Feature | Rheumatic (ARF) | Acute IE | Subacute IE | NBTE | Libman-Sacks |
|---|---|---|---|---|---|
| Cause | Autoimmune (ARF) | S. aureus, virulent organisms | S. viridans, low-virulence organisms | Hypercoagulable states, malignancy, debilitating illness | Systemic lupus erythematosus (SLE) |
| Size | Small (1–2 mm) | Large, bulky (cm) | Small-medium | Small-medium, flat | Small |
| Appearance | Warty, regular verrucae | Bulky, irregular, friable, destructive | Wart-like, less destructive | Flat, bland, sterile | Flat, may involve both surfaces |
| Location | Along valve closure lines (atrial surface mitral/tricuspid) | Atrial surface of AV valves; ventricular surface of semilunar valves | Same as acute IE | Along closure lines; any valve | Both atrial AND ventricular surface (distinctive); involves valve undersurface |
| Destruction | Minimal initially | Severe — leaflet perforation, chordal rupture | Moderate | None (sterile) | None–mild |
| Sterile/Infected | Sterile | Infected | Infected | Sterile | Sterile |
| Embolism risk | Low | High (friable) | Moderate | Moderate | Moderate |
| Sequelae | Chronic valve fibrosis → stenosis | Acute regurgitation, abscess, septic emboli | Subacute regurgitation, immune complications | Transient ischaemic attacks, stroke | Valvular dysfunction, IE risk |
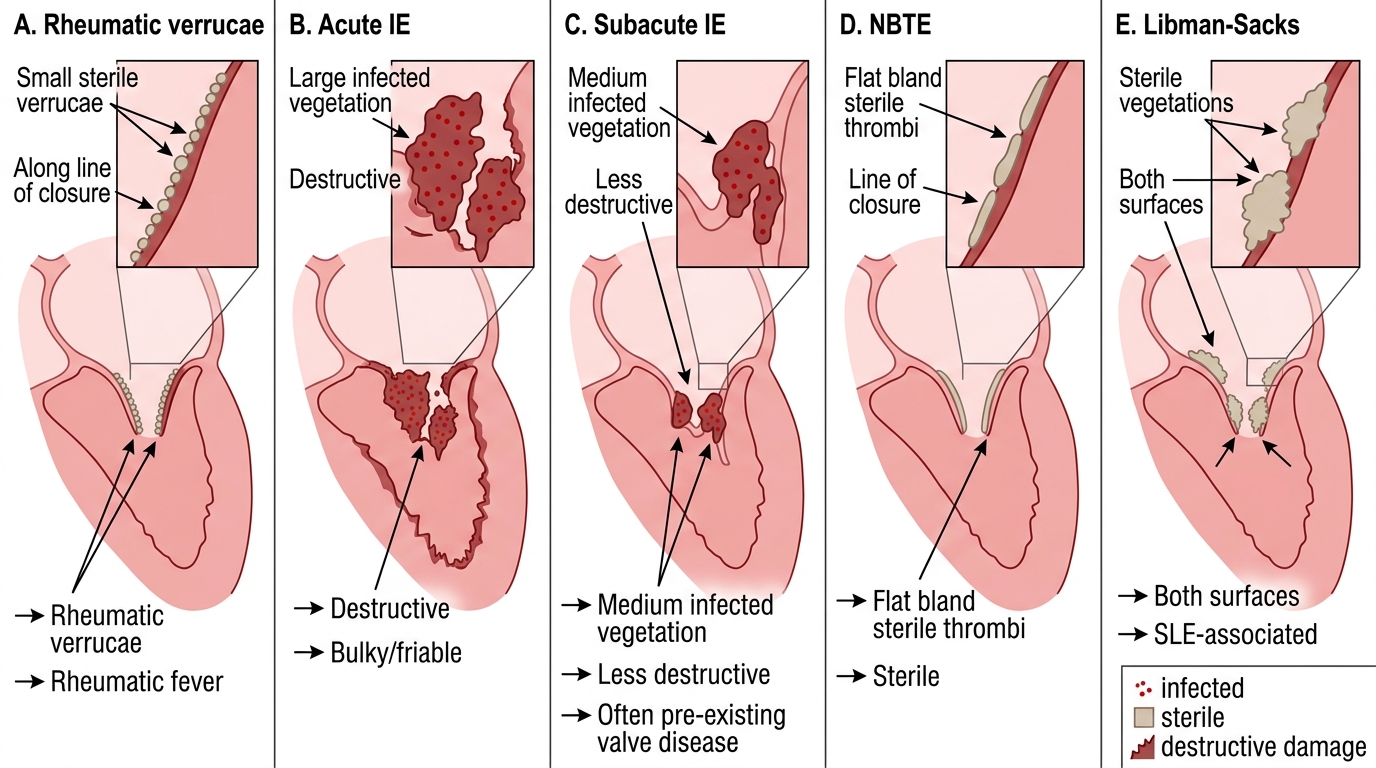
Comparison of Cardiac Valve Vegetations
CLINICAL PEARL
The IV drug user rule: Right-sided IE (tricuspid valve) with septic pulmonary emboli is virtually pathognomonic of IV drug abuse — S. aureus is the culprit in >80% of cases. These patients do NOT usually have pre-existing valve disease. Right-sided IE carries a lower in-hospital mortality than left-sided IE because pulmonary emboli are more survivable than systemic emboli — but recidivism and repeat infection make long-term prognosis poor.
SELF-CHECK
On endomyocardial biopsy of a patient with suspected chronic active rheumatic carditis, the pathologist identifies large macrophage-derived cells with a central wavy bar of chromatin. These cells are:
A. Reed-Sternberg cells — diagnostic of Hodgkin lymphoma infiltrating the myocardium
B. Anitschkov cells (caterpillar cells) — pathognomonic of rheumatic carditis
C. Langhans giant cells — indicating granulomatous myocarditis (sarcoid/TB)
D. Foam cells — indicating lipid-laden macrophages in atherosclerotic plaque
Reveal Answer
Answer: B. Anitschkov cells (caterpillar cells) — pathognomonic of rheumatic carditis
Anitschkov cells (also called caterpillar cells or owl-eye cells) are pathognomonic for rheumatic carditis. They are modified macrophages with a distinctive nucleus where the chromatin is condensed into a central wavy bar resembling a caterpillar. They are the cellular hallmark of the Aschoff body. Reed-Sternberg cells have a 'mirror-image owl-eye' bilobed nucleus; Langhans giant cells have peripherally arranged nuclei in a horseshoe; foam cells are lipid-laden and appear vacuolated.
Putting It Together — Clinico-Pathological Correlation
Clinico-Pathological Timeline of Rheumatic Heart Disease
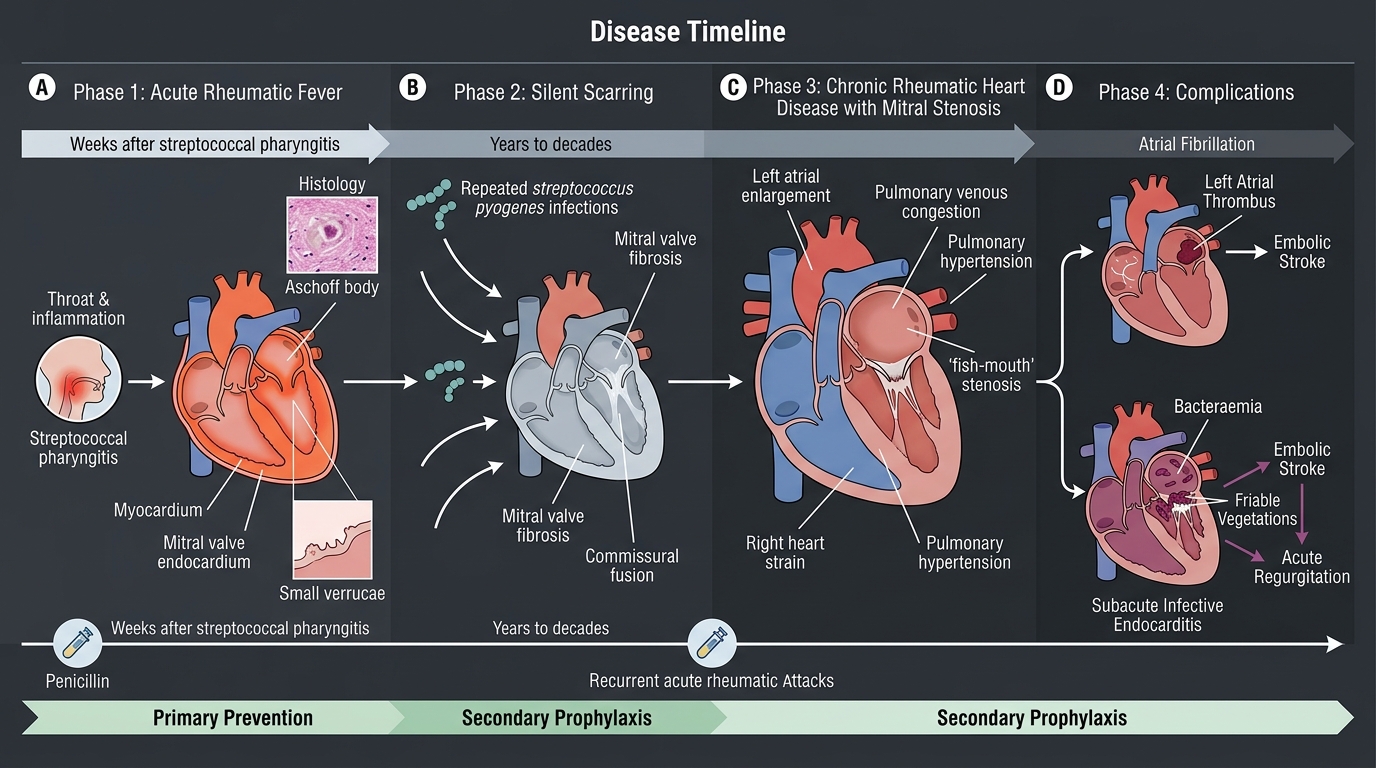
The timeline of rheumatic and endocarditic heart disease illustrates how pathology drives clinical presentation:
Phase 1 — ARF (weeks after strep pharyngitis):
• Pancarditis → pericardial friction rub + myocarditis (PR prolongation, cardiomegaly) + endocarditis (mitral regurgitation murmur)
• Aschoff bodies in myocardium; verrucae on valves
• Most patients recover fully; ~30–40% develop chronic valve disease
Phase 2 — Silent scarring (years to decades):
• Repeated strep infections → repeated ARF attacks → cumulative valve scarring
• Fibrosis + commissural fusion → progressive mitral stenosis
• No symptoms until valve area falls below ~2 cm²
Phase 3 — Chronic RHD (symptomatic mitral stenosis):
• Dyspnoea, orthopnoea, AF, haemoptysis, right heart failure
• Echocardiography: fish-mouth valve, gradient, pulmonary hypertension
• MacCallum's plaque in left atrium
Phase 4 — Complication layer:
• AF → thrombus in left atrium → stroke
• Damaged valve + bacteraemia → subacute IE (S. viridans) → Duke-criteria-positive
• IE vegetations → embolic stroke or acute regurgitation
Prevention is the key: A single course of penicillin for strep pharyngitis in Phase 1 prevents this entire cascade. Secondary prophylaxis (monthly benzathine penicillin) prevents recurrent ARF attacks and halts further valve damage — the most effective cardiovascular preventive intervention available in resource-limited settings.