Page 11 of 26
PA31.8-10 | Adrenal Gland Disorders — SDL Guide
Learning Objectives
- Describe the etiology and pathogenesis of adrenal insufficiency (primary and secondary) and explain the mechanism of hyperpigmentation in Addison disease.
- Outline the causes, clinical manifestations, laboratory investigations, and morphologic adrenal changes in Cushing syndrome.
- Distinguish between primary and secondary hyperaldosteronism (Conn syndrome) in brief.
- Classify adrenal neoplasms, differentiate cortical adenoma from adrenocortical carcinoma, and describe the key pathological features of pheochromocytoma and neuroblastoma.
INSTRUCTIONS
The adrenal gland is a high-yield topic in Year-2 pathology and MBBS university exams. Disorders here cut across endocrinology, oncology, and emergency medicine. As you work through this SDL, connect each hormonal pathway to its morphologic consequence — that pairing is the examiner's favourite question format.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 24 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman is brought to the emergency department with sudden hypotension, vomiting, and altered consciousness. She had been on high-dose prednisolone for rheumatoid arthritis for six months and stopped it abruptly three days ago. Her serum cortisol is critically low. Meanwhile, in the next ward, a 45-year-old man presents with truncal obesity, moon face, striae, hypertension, and a blood glucose of 280 mg/dL.
Same gland, opposite extremes. The adrenal — two grams of tissue above each kidney — governs your blood pressure, stress response, electrolyte balance, and glucose homeostasis simultaneously.
WHY THIS MATTERS
Adrenal pathology is core to the NMC 2024 CBUC PA31 competency group. In clinical practice, Cushing syndrome, Addison disease, and pheochromocytoma are 'great masqueraders' — they present to dermatology, cardiology, and psychiatry before the endocrinologist is called.
For your MBBS exams, expect: (a) a short-answer question on adrenal insufficiency with emphasis on morphology and Waterhouse-Friderichsen syndrome; (b) a structured question on Cushing syndrome causes and the dexamethasone suppression test; (c) a long-answer on pheochromocytoma (rule of 10s, morphology, MEN2). This SDL covers all three competencies — PA31.8, PA31.9, and PA31.10.
RECALL
Before we proceed, anchor the normal adrenal architecture.
Adrenal cortex (mesoderm-derived) — three concentric zones, memorised as GFR:
• Zona glomerulosa (outermost) — secretes mineralocorticoids (aldosterone); regulated by renin-angiotensin system and serum K⁺.
• Zona fasciculata (middle, largest, ~75%) — secretes glucocorticoids (cortisol); regulated by ACTH.
• Zona reticularis (innermost) — secretes adrenal androgens (DHEA, androstenedione); regulated by ACTH.
Adrenal medulla (neural crest-derived) — chromaffin cells secrete catecholamines (epinephrine 80%, norepinephrine 20%); regulated by preganglionic sympathetic fibres.
Pathological changes in each zone are organ-specific: cortical atrophy affects zona fasciculata and reticularis first; aldosteronoma arises from zona glomerulosa.
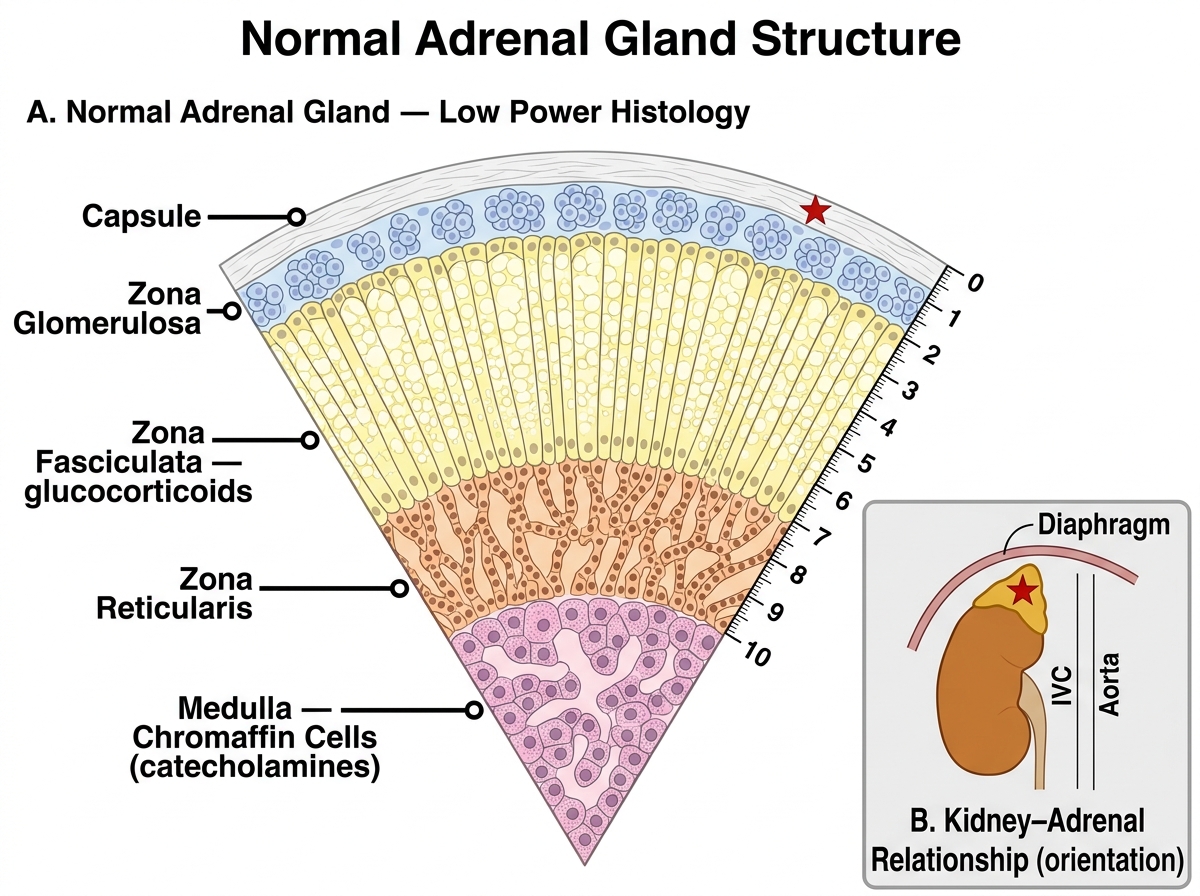
Normal Adrenal Gland — Cortical Zones and Medulla (Low Power Histology)
Cushing Syndrome — Etiology and Pathogenesis
Cushing syndrome is the clinical state produced by chronic excess of glucocorticoids, regardless of source.
Causes (memorise in frequency order):
| Cause | ACTH level | Adrenal morphology |
|---|---|---|
| Exogenous steroids (iatrogenic, commonest overall) | Suppressed (↓↓) | Bilateral cortical atrophy |
| Cushing disease — pituitary ACTH-secreting adenoma | Elevated (↑) | Bilateral cortical hyperplasia |
| Ectopic ACTH — small-cell lung carcinoma, carcinoid, others | Very elevated (↑↑↑) | Bilateral cortical hyperplasia |
| Adrenal adenoma | Suppressed (↓↓) | Contralateral atrophy |
| Adrenocortical carcinoma | Suppressed (↓↓) | Contralateral atrophy |
Pathogenesis: Excess cortisol drives a cascade:
1. Gluconeogenesis ↑ → hyperglycaemia / steroid diabetes.
2. Protein catabolism ↑ → muscle wasting (proximal myopathy), skin thinning, purple striae, poor wound healing.
3. Fat redistribution → truncal obesity, moon face, buffalo hump (dorsal fat pad).
4. Mineralocorticoid receptor activation at high cortisol levels → hypertension, hypokalaemia.
5. Immunosuppression → opportunistic infections.
6. Bone collagen loss → osteoporosis, vertebral fractures.
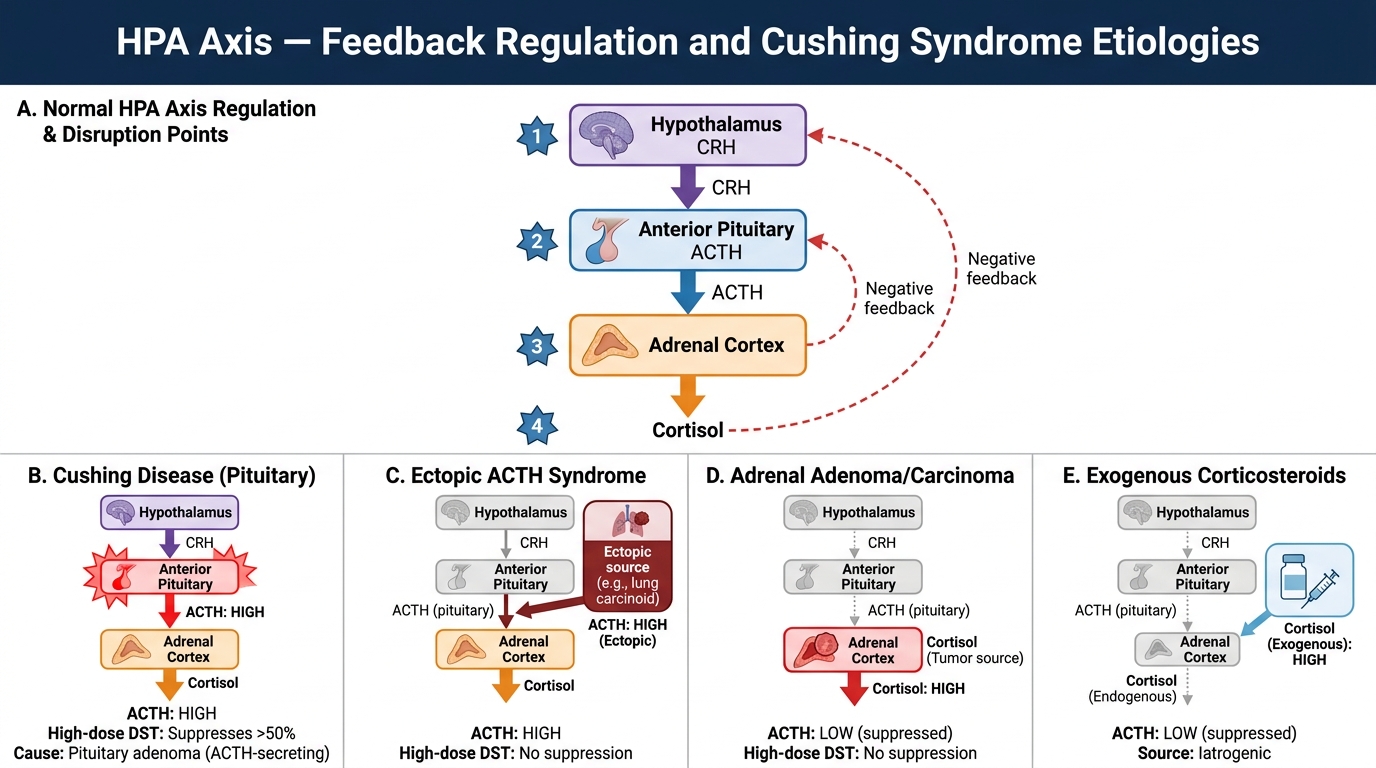
HPA Axis Feedback Regulation and Site of Disruption in Cushing Syndrome
Cushing Syndrome — Clinical Manifestations and Laboratory Diagnosis
Clinical features (know the classic triad for MCQs: truncal obesity + moon face + purple striae):
• Central (truncal) obesity with thin limbs
• Moon face (rounded face due to facial fat deposition)
• Buffalo hump (dorsocervical fat pad)
• Purple/violaceous striae (skin thinning + dermal collagen rupture)
• Hypertension (common, renin-independent)
• Proximal muscle weakness
• Hirsutism and menstrual irregularities (androgen excess from zona reticularis stimulation)
• Psychiatric disturbances (depression, psychosis)
• Osteoporosis, pathological fractures
• Impaired glucose tolerance or frank diabetes
Laboratory investigations:
- 24-hour urinary free cortisol (UFC) — screening; elevated in Cushing syndrome.
- Overnight 1-mg dexamethasone suppression test (DST) — screening; normal persons suppress cortisol below 1.8 µg/dL; Cushing syndrome patients fail to suppress.
- Low-dose DST (2 mg/48 h) — confirms Cushing syndrome if cortisol unsuppressed.
- High-dose DST (8 mg/48 h) — differentiates pituitary Cushing disease (suppresses >50%) from ectopic ACTH or adrenal tumour (does NOT suppress).
- Plasma ACTH — low/undetectable in adrenal tumours and exogenous; high in pituitary and ectopic ACTH.
- Hypokalaemic metabolic alkalosis — especially prominent in ectopic ACTH (very high cortisol activating mineralocorticoid receptors).
Imaging: MRI pituitary (Cushing disease); CT chest/abdomen (ectopic ACTH, adrenal tumour).
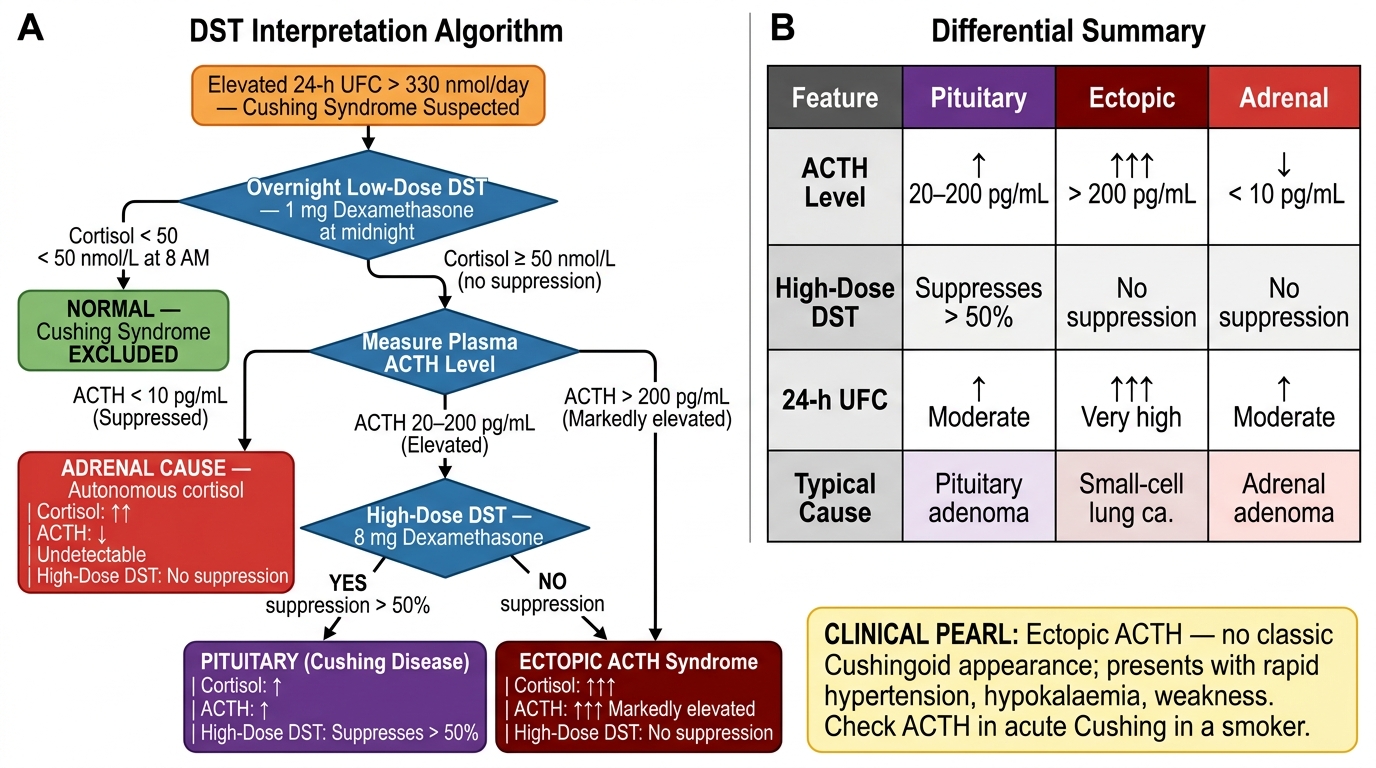
Dexamethasone Suppression Test Interpretation Algorithm
CLINICAL PEARL
The ectopic ACTH syndrome is a clinical pitfall: small-cell lung carcinoma can secrete ACTH so massively that Cushingoid fat redistribution does not have time to develop — patients present with rapid-onset hypertension, hypokalaemia, oedema, and profound weakness without the classic moon face. The very high cortisol activates mineralocorticoid receptors massively. Always check ACTH and do high-dose DST when Cushing syndrome presents acutely in a smoker.
Cushing Syndrome — Adrenal Morphology
The adrenal morphology in Cushing syndrome depends on the underlying cause:
Bilateral cortical hyperplasia (pituitary Cushing disease or ectopic ACTH):
• Both adrenals enlarged (combined weight up to 25–30 g; normal ~8–10 g).
• Cut section shows diffuse or nodular yellow-orange thickening of the cortex.
• Histology: expansion of the clear-cell zona fasciculata; all three zones preserved but hypertrophied.
Cortical atrophy (exogenous steroids — most important to know):
• Exogenous steroids suppress ACTH → zona fasciculata and reticularis undergo disuse atrophy.
• Zona glomerulosa (ACTH-independent) is spared.
• This is the morphologic correlate of adrenal crisis on abrupt steroid withdrawal.
Adrenal cortical adenoma (ACTH-independent):
• Usually unilateral, small (<5 cm), well-encapsulated, golden-yellow (lipid-rich).
• Contralateral adrenal and uninvolved ipsilateral cortex show atrophy (suppressed ACTH).
Adrenocortical carcinoma: described in the neoplasms section.
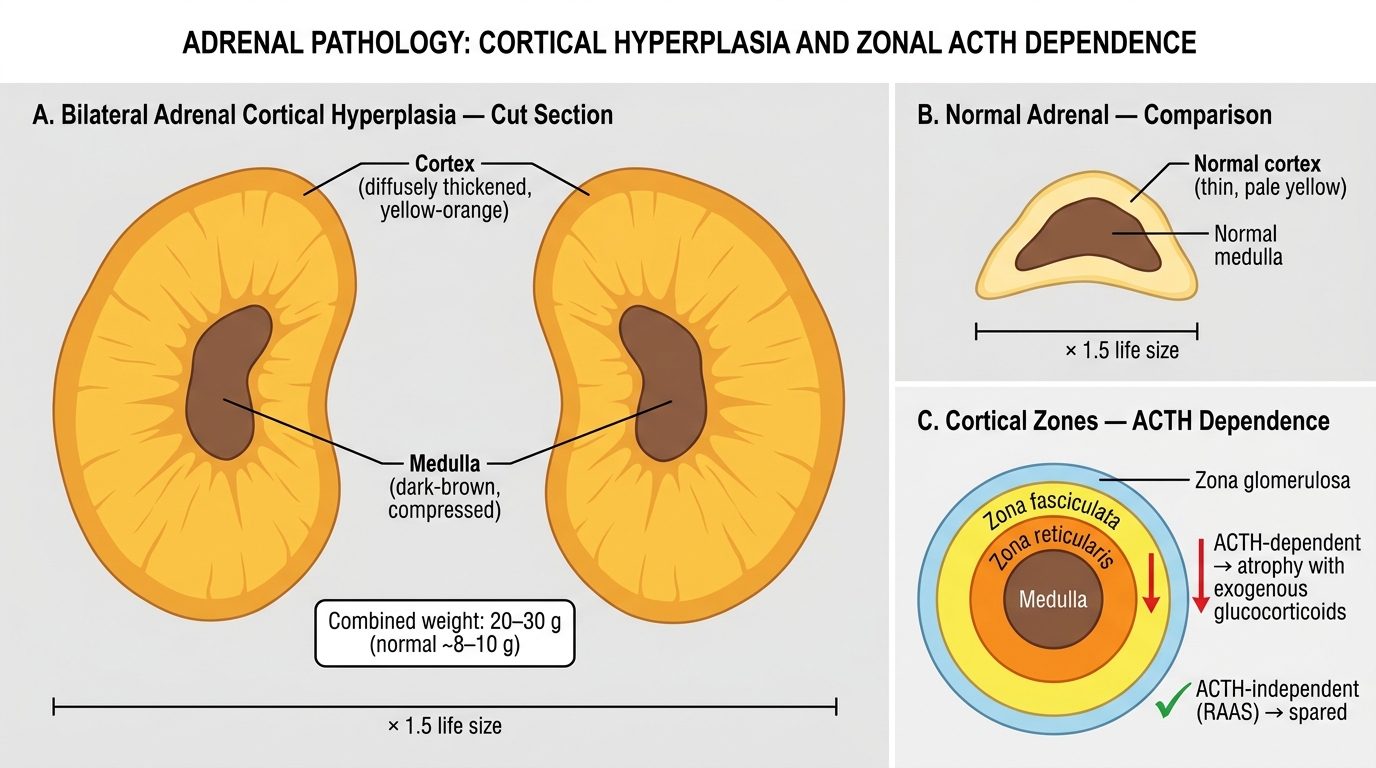
Bilateral Adrenal Cortical Hyperplasia: Gross Pathology and Cortical Zone ACTH Dependence
SELF-CHECK
A patient on long-term prednisolone for nephrotic syndrome stops the drug abruptly. Which adrenal zone is MOST affected by the resulting atrophy?
A. Zona glomerulosa only
B. Zona fasciculata and zona reticularis
C. Adrenal medulla only
D. All three cortical zones equally
Reveal Answer
Answer: B. Zona fasciculata and zona reticularis
Exogenous glucocorticoids suppress pituitary ACTH via negative feedback. Zona fasciculata and zona reticularis are ACTH-dependent and undergo disuse atrophy. Zona glomerulosa is regulated primarily by the renin-angiotensin-aldosterone system and is therefore ACTH-independent, so it is relatively spared.