Page 12 of 26
PA31.8-10 | Adrenal Gland Disorders — SDL Guide (Part 2)
Hyperaldosteronism — Conn Syndrome (Brief Overview)
Primary hyperaldosteronism (Conn syndrome) results from autonomous aldosterone excess independent of the renin-angiotensin system.
Causes:
• Aldosterone-producing adenoma (APA) — ~65% of primary cases; small (<2 cm), bright-yellow, zona glomerulosa–derived.
• Idiopathic bilateral adrenal hyperplasia (BAH) — ~30%; both glands show zona glomerulosa hyperplasia.
• Adrenocortical carcinoma producing aldosterone — rare.
Pathophysiology: Excess aldosterone → Na⁺ retention + K⁺ excretion → hypertension + hypokalaemia + suppressed plasma renin (key lab finding that distinguishes primary from secondary).
Secondary hyperaldosteronism: Renin is elevated (e.g., renal artery stenosis, congestive heart failure, cirrhosis). Both renin and aldosterone are elevated; adrenal morphology shows bilateral hyperplasia secondary to angiotensin II drive.
Key lab: Elevated aldosterone-to-renin ratio (ARR >30) with suppressed renin is diagnostic of primary hyperaldosteronism.
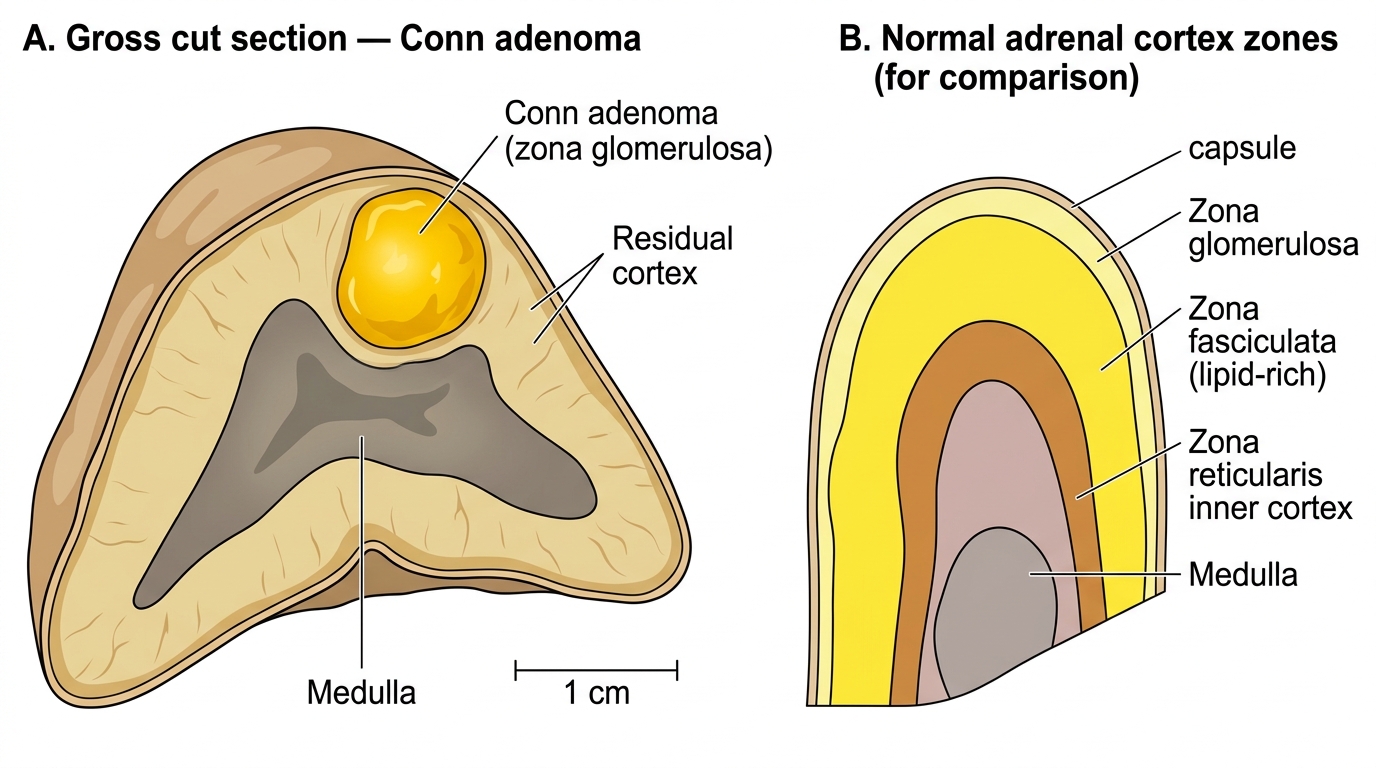
Conn Adenoma (Zona Glomerulosa Adenoma) — Gross Specimen and Normal Adrenal Cortex
Primary Adrenal Insufficiency — Addison Disease
Adrenal insufficiency is the failure to produce adequate cortisol and/or aldosterone. Primary adrenal insufficiency (Addison disease) involves destruction or dysfunction of the adrenal cortex itself.
Etiology (causes of Addison disease):
- Autoimmune adrenalitis — commonest cause in developed countries (~70–80%). Autoantibodies against 21-hydroxylase (key enzyme in steroid synthesis). Often part of autoimmune polyendocrine syndrome (APS) types 1 or 2.
- Tuberculosis — historically important; still commonest cause in developing countries including India. Haematogenous spread → bilateral caseating granulomas → adrenal destruction. Glands are enlarged initially, then fibrotic and calcified.
- Metastatic carcinoma — lung, breast, melanoma can destroy >90% of both glands; functional insufficiency usually requires >90% destruction.
- Histoplasmosis, CMV (HIV patients) — opportunistic infections.
- Waterhouse-Friderichsen syndrome (acute adrenal insufficiency) — bilateral adrenal haemorrhage in overwhelming sepsis, classically Neisseria meningitidis (also DIC, Pseudomonas). Endotoxin-driven vascular injury + DIC → haemorrhagic infarction of both glands → adrenal crisis.
Morphology:
• Autoimmune: bilateral adrenal atrophy; cortex replaced by lymphocytic infiltrate and fibrosis; medulla spared.
• TB: bilateral enlargement → caseating granulomas → eventual calcification.
• Waterhouse-Friderichsen: massively enlarged, haemorrhagic adrenals — cortex appears as a blood-soaked rim.
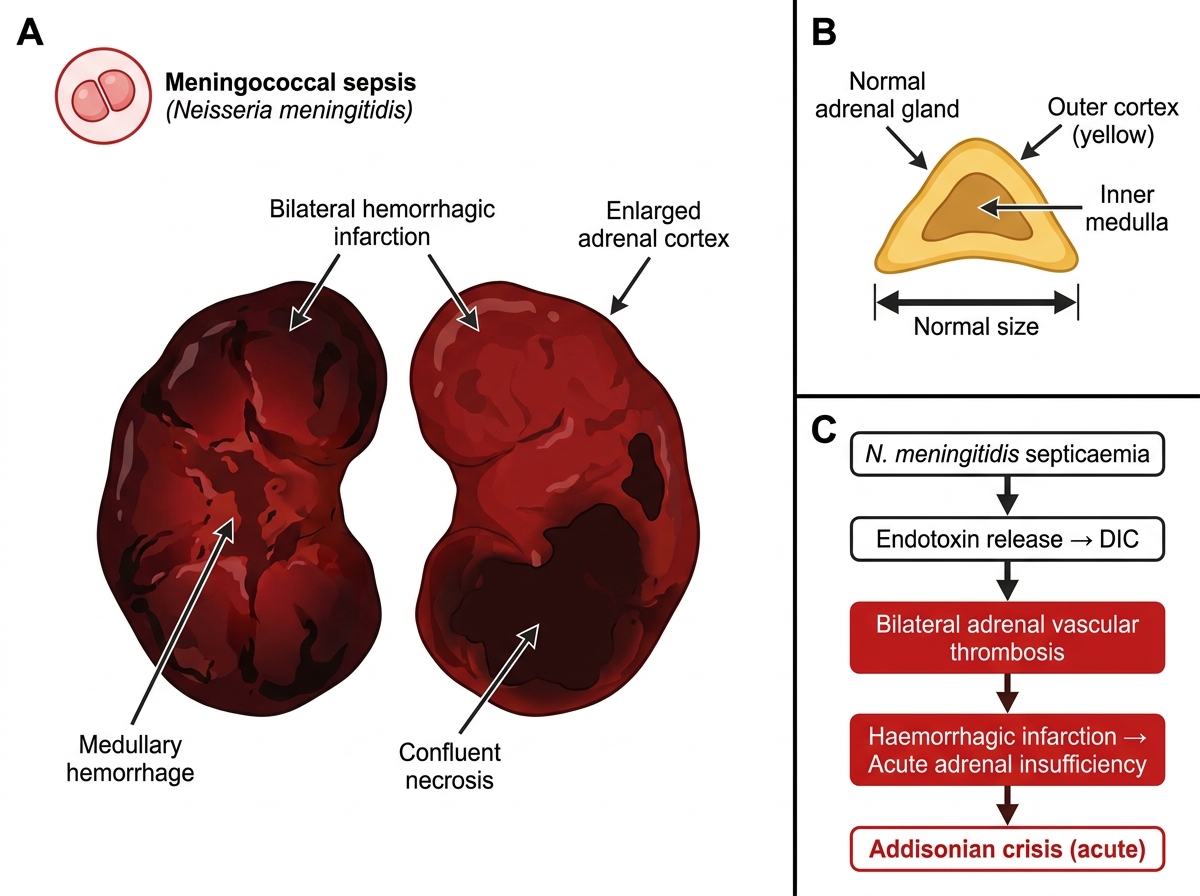
Waterhouse-Friderichsen Syndrome: Gross Pathology and Pathogenesis
Adrenal Insufficiency — Clinical Manifestations, Lab, and Mechanism of Hyperpigmentation
Manifestations of primary adrenal insufficiency (Addison disease):
| Feature | Mechanism |
|---|---|
| Weakness, fatigue | Reduced cortisol (impaired gluconeogenesis, metabolic effects) |
| Hypotension, postural dizziness | Aldosterone deficiency → Na⁺ loss, K⁺ retention, volume depletion |
| Hyponatraemia, hyperkalaemia | Aldosterone deficiency |
| Hypoglycaemia | Cortisol deficiency — reduced gluconeogenesis |
| Hyperpigmentation (skin + buccal mucosa) | See below |
| Nausea, vomiting, weight loss | Non-specific, cortisol deficiency |
| Salt craving | Aldosterone deficiency |
Mechanism of hyperpigmentation (frequently asked in exams):
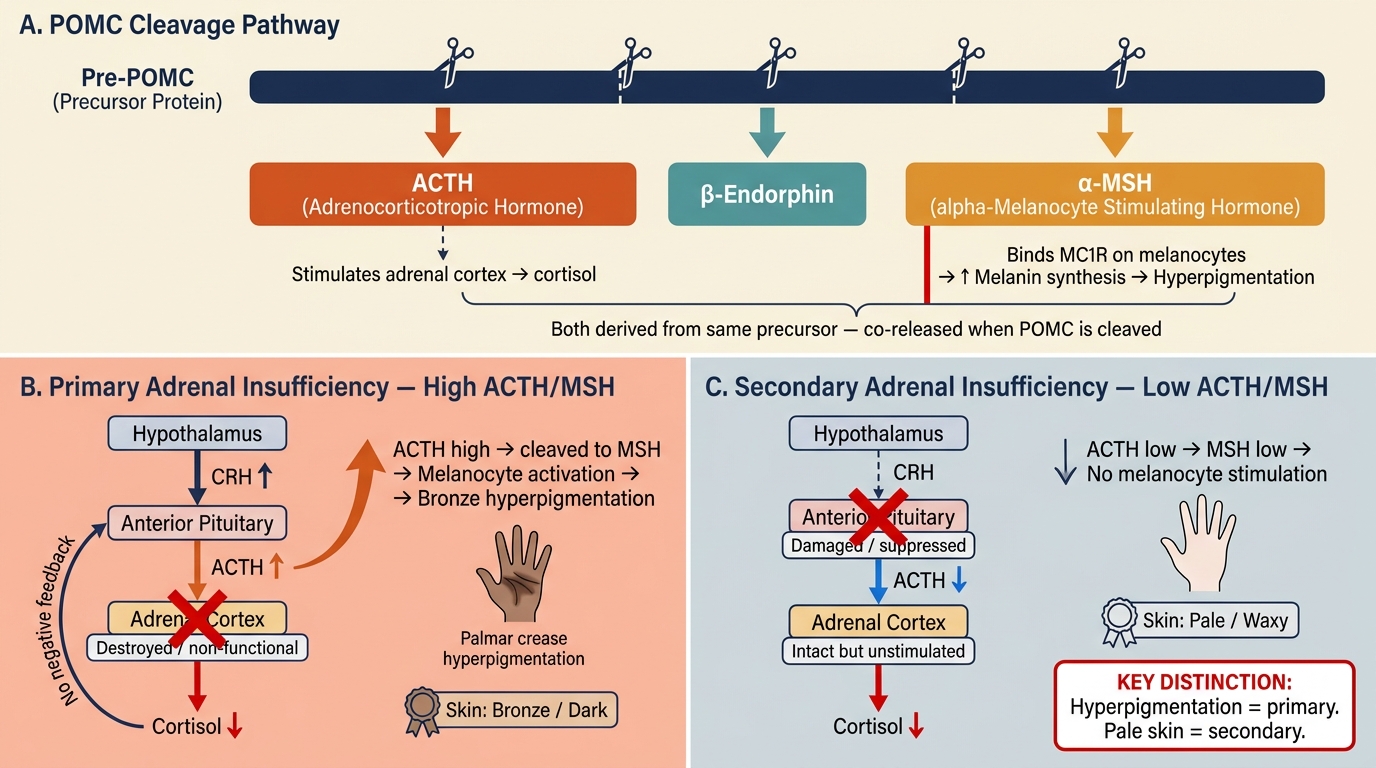
• Cortisol deficiency disinhibits the pituitary → ↑ ACTH secretion.
• ACTH is derived from pro-opiomelanocortin (POMC) by cleavage. The same POMC molecule also gives rise to melanocyte-stimulating hormone (α-MSH).
• Elevated POMC processing → elevated α-MSH → stimulates MC1R (melanocortin-1 receptor) on melanocytes → increased melanin synthesis.
• Hyperpigmentation is therefore a feature of primary insufficiency (elevated ACTH) and is ABSENT in secondary insufficiency (pituitary disease → ACTH is low).
Secondary adrenal insufficiency: Pituitary disease (tumor, infarction, Sheehan syndrome) → ↓ ACTH → ↓ cortisol. Aldosterone is preserved (RAAS intact). No hyperpigmentation. No hyperkalaemia. Hypoglycaemia and hyponatraemia (via SIADH) predominate.
Laboratory: Low serum cortisol (AM); Low 24-h urinary cortisol; ACTH stimulation test (Synacthen test) — in primary, adrenals fail to respond; in secondary, adrenals respond sluggishly (functional atrophy) but eventually respond with prolonged ACTH stimulation.
POMC Cleavage Pathway and Skin Pigmentation in Adrenal Insufficiency
CLINICAL PEARL
Hyperpigmentation distinguishes primary from secondary adrenal insufficiency at the bedside. In Addison disease (primary), look for bronze skin, hyperpigmented palmar creases, buccal mucosal patches, and pigmentation of surgical scars. In secondary insufficiency (hypopituitarism), the skin is pale and waxy — 'alabaster skin' — because ACTH and MSH are both low. This clinical sign alone determines whether to check ACTH levels or order an MRI pituitary.
SELF-CHECK
A 30-year-old man from rural India presents with weakness, weight loss, hyperpigmentation of the buccal mucosa, low blood pressure, hyponatraemia, and hyperkalaemia. Chest X-ray shows bilateral adrenal calcification. What is the MOST likely underlying cause?
A. Autoimmune adrenalitis (Addison disease)
B. Adrenocortical carcinoma with bilateral metastases
C. Tuberculous adrenalitis
D. Waterhouse-Friderichsen syndrome
Reveal Answer
Answer: C. Tuberculous adrenalitis
The combination of Addison disease features (hyperpigmentation, hypotension, hyponatraemia, hyperkalaemia) with bilateral adrenal calcification on imaging in a patient from rural India points strongly to tuberculous adrenalitis. TB causes haematogenous seeding of both adrenal glands with caseating granulomas; as the disease resolves, the glands fibrose and calcify. Autoimmune adrenalitis would not show calcification. Waterhouse-Friderichsen presents acutely with haemorrhage, not calcification.