Page 13 of 26
PA31.8-10 | Adrenal Gland Disorders — SDL Guide (Part 3)
Adrenocortical Neoplasms — Adenoma vs Carcinoma
Adrenal cortical neoplasms arise from any zone of the cortex. The central diagnostic challenge is distinguishing benign adenoma from malignant carcinoma.
Cortical Adenoma:
• Common (incidental finding — 'incidentaloma' in 1–5% of abdominal CTs).
• Usually small (<5 cm, <50 g), well-encapsulated, bright-yellow (lipid-rich), solitary.
• Most are non-functional. Functional adenomas produce cortisol (Cushing), aldosterone (Conn), or androgens.
• Histology: clear lipid-laden cells resembling zona fasciculata, with mild nuclear pleomorphism; no capsular/vascular invasion, low mitotic rate.
Adrenocortical Carcinoma (ACC):
• Rare but aggressive; bimodal peak (children <5 yr; adults 40–50 yr).
• Large tumours (>10 cm, >100 g) — weight >100 g is a useful threshold (though overlap exists with Weiss criteria).
• Cut section: haemorrhagic, necrotic, may invade adjacent organs.
• ~50% are functional — produce cortisol (±androgens → virilisation in women).
• Weiss criteria (histologic malignancy score, ≥3 of 9 = malignant):
- Nuclear grade 3 or 4 (Fuhrman)
- Mitotic rate >5/50 HPF
- Atypical mitoses
- Clear cells <25% of tumour cells
- Diffuse architecture >33%
- Necrosis present
- Venous invasion
- Sinusoidal invasion
- Capsular invasion
• Prognosis poor — 5-year survival ~35%.
| Feature | Adenoma | Carcinoma |
|---|---|---|
| Size | <5 cm, <50 g | >10 cm, >100 g |
| Capsule | Intact, well-encapsulated | Invasion common |
| Mitoses | Rare, typical | >5/50 HPF, atypical |
| Necrosis | Absent | Present |
| Prognosis | Excellent | Poor (5-yr ~35%) |
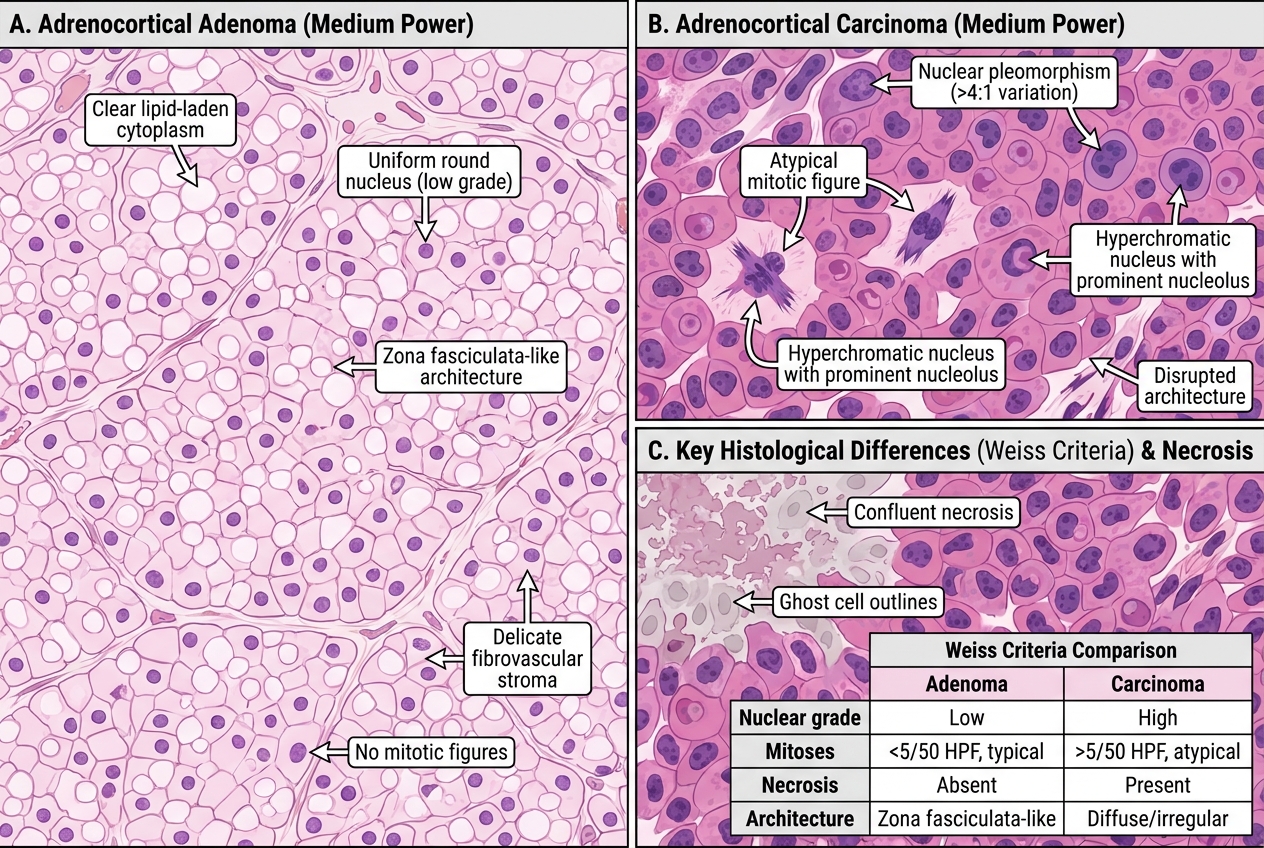
Adrenocortical Adenoma vs Carcinoma — Histology at Medium Power with Key Differentiating Features
Pheochromocytoma — Pathology and Rule of 10s
Pheochromocytoma is a catecholamine-secreting tumour arising from chromaffin cells of the adrenal medulla.
Pathogenesis: Tumour chromaffin cells secrete epinephrine and norepinephrine (and dopamine in extra-adrenal variants) → paroxysmal or sustained hypertension, headache, sweating, palpitations (the 'paroxysmal 4' — 5Ps: Pressure, Pain, Perspiration, Palpitations, Pallor).
Rule of 10s (must know for exams):
• ~10% are bilateral
• ~10% are extra-adrenal (paragangliomas; para-aortic, organ of Zuckerkandl)
• ~10% are familial (MEN2A, MEN2B, VHL, NF1, SDH mutations)
• ~10% are malignant (defined by metastasis, not histology alone)
• ~10% occur in children
MEN2 association: MEN2A = pheochromocytoma + medullary thyroid carcinoma (MTC) + hyperparathyroidism; MEN2B = pheo + MTC + mucosal neuromas + marfanoid habitus. Gene: RET proto-oncogene mutations.
Morphology:
• Gross: well-demarcated, tan-grey to haemorrhagic; average 5 cm, 100 g.
• Zellballen pattern (characteristic): nests of polygonal chromaffin cells separated by a delicate vascular network; 'zellballen' = German for 'cell balls'.
• Cells have abundant granular cytoplasm (catecholamine granules → brown with chromate fixative — 'chromaffin reaction').
• Cannot reliably distinguish benign from malignant histologically — malignancy defined only by metastasis.
Biochemical diagnosis: Elevated plasma metanephrines or 24-hour urinary VMA (vanillylmandelic acid) and fractionated metanephrines; urine catecholamines.
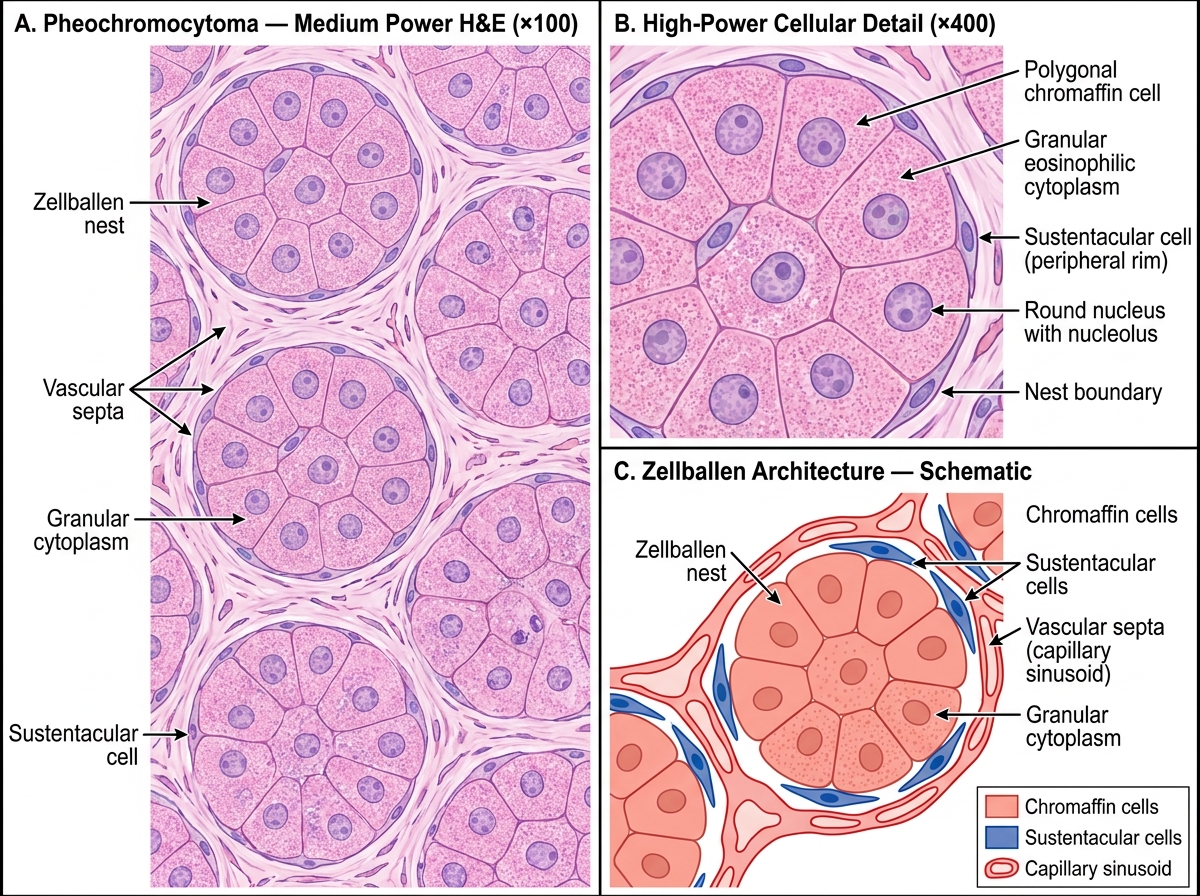
Histology of Pheochromocytoma — Zellballen Architecture (Medium & High Power)
CLINICAL PEARL
Pheochromocytoma is a 'great mimicker' of hypertensive crises. The classic presentation is paroxysmal hypertension precipitated by tumour manipulation, anaesthesia, certain drugs (beta-blockers without alpha-blockade first — causing paradoxical hypertension by blocking beta-2 vasodilation), or consumption of tyramine-rich foods. The sequence for surgical removal is alpha-blockade first (phenoxybenzamine) followed by beta-blockade — reversing this order can precipitate a fatal hypertensive crisis. For your exams, also remember: never give metoclopramide or glucagon to a known/suspected pheo patient.
Neuroblastoma — Paediatric Adrenal Medullary Tumour
Neuroblastoma is the commonest extracranial solid tumour of childhood, arising from primitive sympathoblasts (neural crest precursors of the adrenal medulla and sympathetic ganglia).
Epidemiology: Median age ~2 years; 90% present before age 5. Adrenal medulla is the primary site in ~40%; rest arise in paravertebral sympathetic ganglia (neck, chest, abdomen, pelvis).
Molecular biology (high-yield):
• N-myc (MYCN) amplification — most important adverse prognostic factor; >10 copies = poor prognosis.
• Deletion of chromosome 1p and 11q — additional poor prognostic markers.
• Trk-A (NTRK1) expression — favourable prognostic marker; tumours with TrkA undergo spontaneous differentiation (the basis of 'spontaneous regression' in Stage 4S).
Morphology:
• Small round blue cell tumour (along with Ewing sarcoma, Wilms tumour, rhabdomyosarcoma, PNET).
• Homer-Wright pseudorosettes (pathognomonic): tumour cells arranged in a circle around a central fibrillar core of neuropil (NOT around a vessel — this distinguishes them from true rosettes).
• Schwannian stroma absent (distinguishes from ganglioneuroblastoma/ganglioneuroma in the spectrum).
Clinical features: Abdominal mass; periorbital ecchymoses (Hutchinson sign — orbital metastasis); opsoclonus-myoclonus; bone pain from marrow metastasis; elevated urinary HVA (homovanillic acid) and VMA.
International Neuroblastoma Risk Classification (INRG): Very low, low, intermediate, high based on MYCN, stage, histology, age.
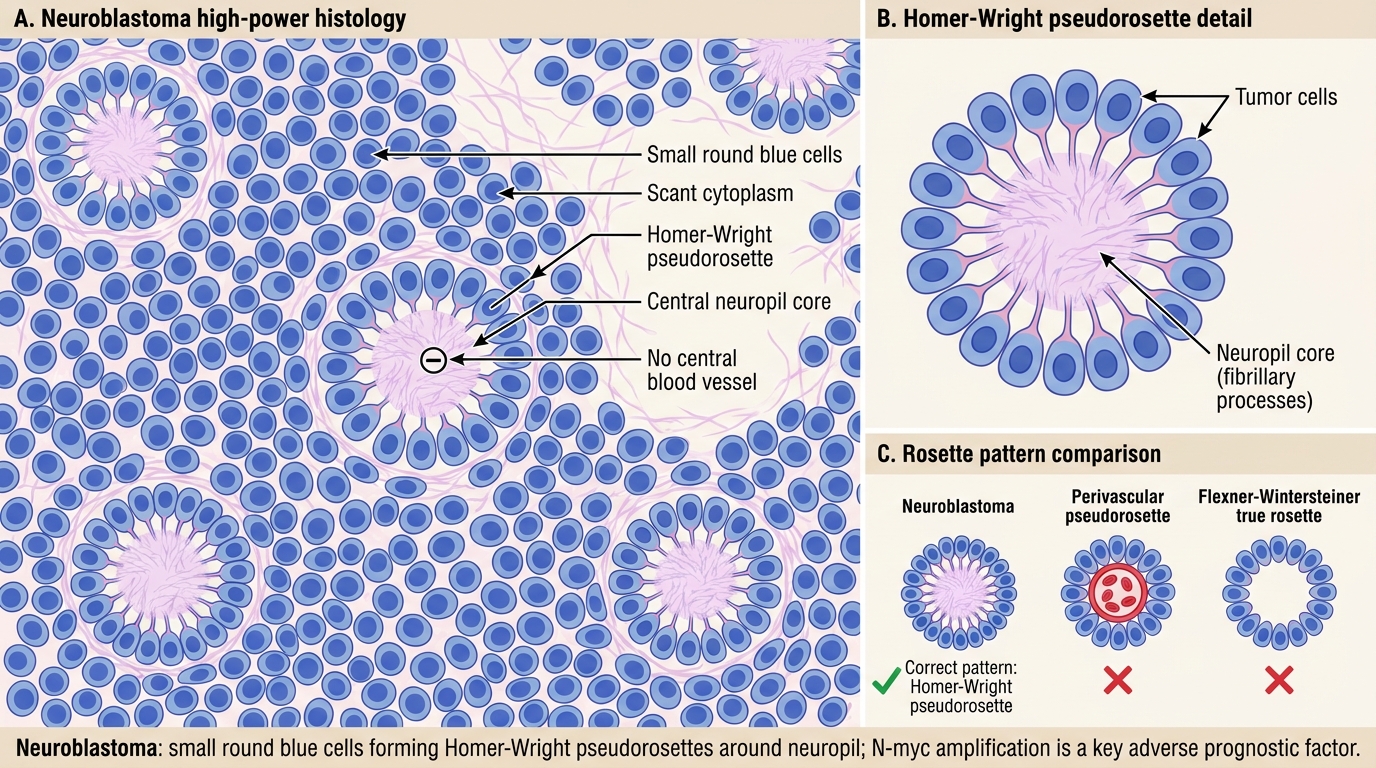
Neuroblastoma: Homer-Wright Pseudorosettes
SELF-CHECK
On histology of an adrenal medullary tumour in a 3-year-old child, you see small round blue cells arranged in circles around a central fibrillar core with no central vessel. Elevated urinary HVA confirms the diagnosis. What is this pathognomonic histologic pattern called?
A. Zellballen pattern
B. Homer-Wright pseudorosettes
C. Flexner-Wintersteiner rosettes
D. Perivascular pseudorosettes
Reveal Answer
Answer: B. Homer-Wright pseudorosettes
Homer-Wright pseudorosettes are the pathognomonic feature of neuroblastoma. The cells cluster around a central core of neuropil (fibrillar cytoplasmic processes) rather than around a vessel. Zellballen (cell balls) is the nesting pattern of pheochromocytoma. Flexner-Wintersteiner rosettes are seen in retinoblastoma (cells form a true rosette around a central lumen). Perivascular pseudorosettes are seen in ependymoma.