Page 19 of 26
PA31.{5,7} | Diabetes Mellitus & Pancreatic Cancer — SDL Guide (Part 5)
Clinical Manifestations, Lab Markers, Spread, and Prognosis
Clinical presentation — the 'silent assassin' pattern:
The pancreas is a retroperitoneal organ with no early warning system. Symptoms appear late, usually when the tumour is locally advanced or metastatic.
Head-of-pancreas tumours (60% of cases) — triad of:
1. Painless obstructive jaundice — the most common presenting symptom; caused by compression of the common bile duct; associated with acholic (clay-coloured) stools, dark urine, and pruritus
2. Courvoisier's sign — palpable, non-tender gallbladder in the presence of jaundice; law: "In obstructive jaundice with a palpable gallbladder, the cause is unlikely to be gallstones" (because gallstones → chronic inflammation → fibrotic, non-distensible gallbladder; cancer → gradual duct obstruction → distensible gallbladder)
3. Epigastric/back pain — radiation to the back in a boring quality; due to coeliac plexus invasion; often the sign of unresectability
Body/tail tumours: Present later with vague abdominal pain, weight loss, and jaundice only if metastases involve the liver — smaller tumours are often detected incidentally
Systemic and paraneoplastic features:
- Weight loss and cachexia — almost universal; due to anorexia, malabsorption (pancreatic duct obstruction → exocrine insufficiency → steatorrhoea), and tumour-derived catabolic cytokines
- New-onset DM in an elderly patient without obvious risk factors — 25% of PDAC patients develop DM within 1–3 years of diagnosis; may precede cancer diagnosis by years
- Trousseau's migratory thrombophlebitis — recurrent superficial thrombophlebitis affecting different veins; classic paraneoplastic sign of mucin-secreting adenocarcinomas (PDAC is the prototype); mechanism: tumour mucin activates tissue factor → hypercoagulable state; Trousseau coined this after noticing it in his own gastric cancer
- Depression and anxiety — disproportionate to stage; may precede diagnosis
Laboratory investigations:
- CA19-9 (carbohydrate antigen 19-9, also called sialyl Lewis Aᵃ antigen) — the most useful tumour marker:
- Sensitivity 80–85%, specificity 70–80% for PDAC
- Not diagnostic alone — elevated in biliary obstruction (benign or malignant), pancreatitis, cholangiocarcinoma
- Most useful for monitoring treatment response and recurrence in known PDAC
- Patients who are Lewis blood group negative (10–15% of population) cannot synthesise CA19-9 and will always have undetectable levels regardless of tumour status
- Liver function tests: Elevated bilirubin (conjugated), ALP, GGT, transaminases — obstructive pattern
- CT/MRI: Double duct sign (dilated CBD + main pancreatic duct); vascular encasement (superior mesenteric artery/vein → unresectability); liver metastases
Metastatic spread:
- Lymphatic: Peripancreatic, coeliac, and para-aortic lymph nodes — early, virtually universal
- Perineural: Along nerve sheaths (as above) — explains poor surgical margins
- Haematogenous: Liver (most common site, portal circulation), lungs, peritoneum
- Direct extension: Duodenum, stomach, spleen, superior mesenteric vessels
Prognosis:
- Overall 5-year survival: < 10% (one of the worst of any solid tumour)
- <20% of patients have resectable disease at diagnosis
- After potentially curative pancreatectomy (Whipple procedure): 5-year survival 20–25% (improved with adjuvant chemotherapy)
- Median survival with metastatic disease: 6–12 months
- The grim prognosis reflects: late presentation, early vascular and perineural invasion, desmoplastic stroma (drug-resistant), and lack of effective screening
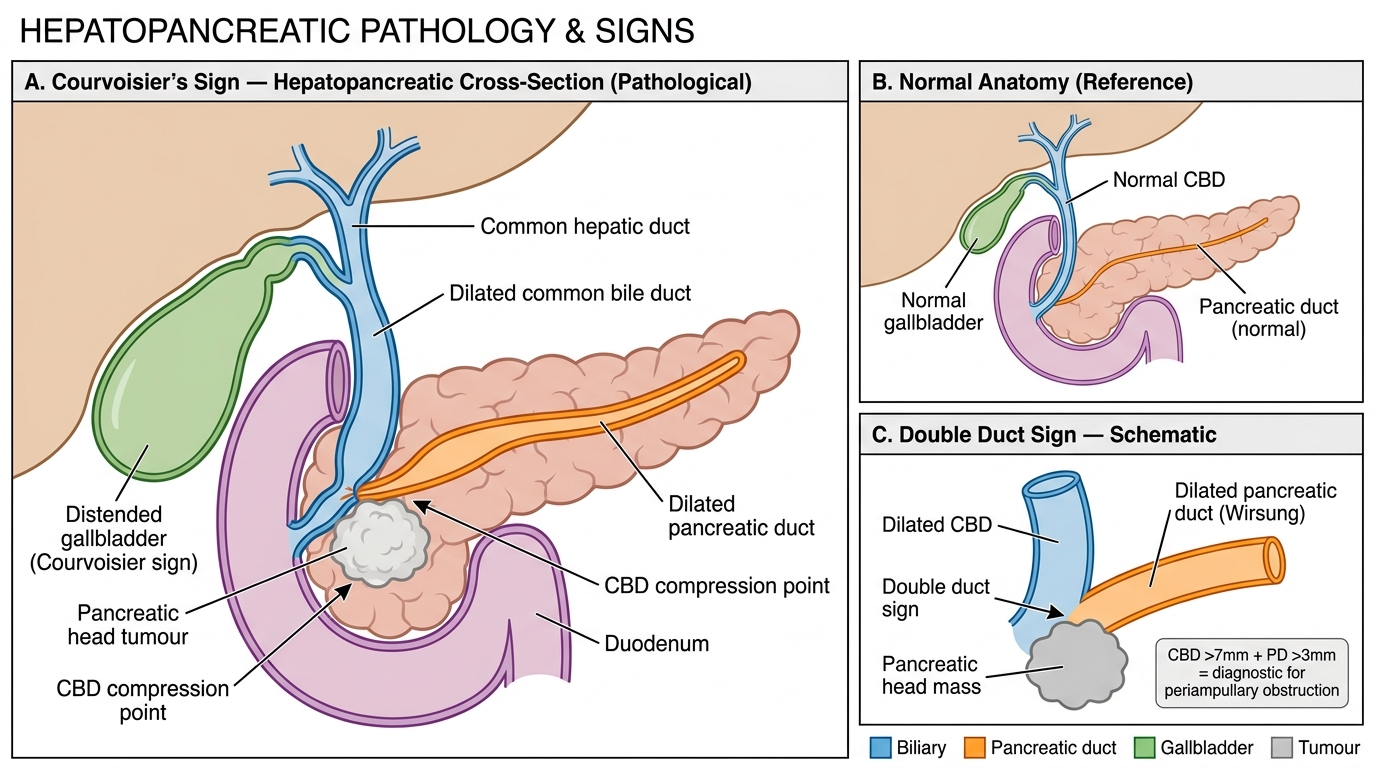
Courvoisier's Sign — Hepatopancreatic Anatomy, Pathology, and Double Duct Sign
CLINICAL PEARL
Trousseau's Tragic Self-Diagnosis: Armand Trousseau, the eminent 19th-century French physician, first described migratory thrombophlebitis as a sign of occult visceral malignancy in 1865. When he noticed the sign in his own arm shortly after, he reportedly said: 'I am lost — I have been seized with thrombosis.' He died of gastric cancer within months. The sign that bears his name — superficial migratory thrombophlebitis in a patient with unexplained weight loss, new DM, or obstructive jaundice — should prompt urgent investigation for a mucin-secreting carcinoma, most commonly PDAC.
SELF-CHECK
A 67-year-old man presents with a 6-week history of painless jaundice, 8 kg weight loss, and a palpable gallbladder. CT abdomen shows a 3.5 cm mass in the head of the pancreas with dilation of both the CBD and pancreatic duct. CA19-9 is 1,840 U/mL. Biopsy shows irregular glands in a desmoplastic stroma with perineural invasion. Which molecular alteration is MOST likely to predict extensive metastatic disease and a worse surgical outcome?
A. KRAS codon 12 mutation
B. SMAD4 (DPC4) deletion
C. p16/CDKN2A loss
D. TP53 point mutation
Reveal Answer
Answer: B. SMAD4 (DPC4) deletion
Loss of SMAD4 (DPC4) is the molecular alteration most strongly associated with widespread haematogenous metastasis and poor surgical outcome in PDAC. SMAD4 is a mediator of TGF-β tumour suppressor signalling; its loss correlates with the metastatic phenotype, and loss of SMAD4 immunostaining on IHC is used as a surrogate marker in some centres to distinguish locally advanced disease (SMAD4 intact) from widely metastatic disease (SMAD4 lost) — guiding surgery vs palliative intent. KRAS is mutated in >90% of PDAC (too ubiquitous to predict metastasis specifically); p16 loss and TP53 mutation are early/intermediate events that do not specifically predict the metastatic phenotype as reliably as SMAD4 deletion.