Page 1 of 26
PA31.1-3 | Thyroid: Goiter, Thyroiditis & Thyroid Function Disorders — SDL Guide
Learning Objectives
- Classify thyroid swellings (goiter) and explain the role of iodine deficiency in their pathogenesis
- Describe the morphological features of diffuse nontoxic goiter and multinodular goiter at gross and histological levels
- Explain the autoimmune pathogenesis of Hashimoto thyroiditis and correlate with its microscopic features and clinical outcome
- Distinguish subacute granulomatous (de Quervain) thyroiditis from Riedel thyroiditis and subacute lymphocytic thyroiditis
- Describe the pathogenesis of Graves disease, explain the role of TSI antibodies, and recognise its morphological hallmarks
- Compare and contrast thyrotoxicosis and hypothyroidism in terms of causes, clinical manifestations, and laboratory/imaging features
- Interpret TSH, free T4, and RAIU patterns to deduce the likely thyroid disorder in a given clinical scenario
INSTRUCTIONS
The thyroid is the most commonly diseased endocrine organ in clinical medicine — goiter affects ~800 million people worldwide and autoimmune thyroid disease is the leading cause of thyroid dysfunction in iodine-replete populations. Understanding thyroid pathology at the structural and molecular level will directly inform your interpretation of thyroid function tests, ultrasound reports, and FNAC findings in clinical postings. Work through each section actively — attempt every micro-quiz before reading the explanation. Estimated reading time: 38 minutes. Keep Robbins Ch. 24 open alongside for the gross photographs.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 24 — The Endocrine System (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old woman from rural Jharkhand presents with a 4-year history of gradually enlarging anterior neck swelling. She is euthyroid. Her 8-year-old daughter has been struggling in school — poor concentration, short stature, and cold intolerance. Iodine deficiency is suspected. Ten years later, the same woman re-presents — now with palpitations, weight loss despite a good appetite, heat intolerance, and protruding eyes. Her TSH is undetectable.
Two thyroid disorders, one family — yet their pathogenesis is completely different. This capsule explains how a single gland can fail in such opposite directions.
WHY THIS MATTERS
Thyroid disorders are the most common endocrine conditions you will encounter in OPD, wards, and community medicine postings. Goiter is endemic in the Himalayan belt and parts of peninsular India. Autoimmune thyroiditis (Hashimoto) is the most common cause of hypothyroidism in iodine-replete urban populations. Graves disease is the most common cause of hyperthyroidism.
As a future clinician, you will:
• Order and interpret TSH, free T4/T3, TPO antibodies, RAIU scans
• Recognise the cardinal signs of hyperthyroidism (sympathetic storm) vs. hypothyroidism (metabolic slowdown)
• Correlate an FNAC report with clinical presentation
• Understand why a euthyroid goiter can suddenly become toxic
The PA31 competency cluster maps directly to these clinical skills.
RECALL
Before reading further, recall the following from Physiology (PY — Endocrine System):
- TSH (thyroid-stimulating hormone) from the anterior pituitary binds TSHR on follicular cells → activates adenylyl cyclase → increased cAMP → synthesis and release of T3 and T4.
- T4 is the predominant secretory product; peripheral conversion of T4 → T3 by deiodinases. T3 is the biologically active form.
- Negative feedback: rising T3/T4 suppresses TRH (hypothalamus) and TSH (pituitary).
- Iodine is essential: one iodine atom is added to tyrosine residues on thyroglobulin to form monoiodotyrosine (MIT) and diiodotyrosine (DIT); coupling of DIT+DIT → T4, DIT+MIT → T3.
- The follicular cell synthesises thyroglobulin and secretes it into the follicular lumen (colloid); TSH stimulates endocytosis of colloid and proteolytic release of T3/T4.
If any of these steps are unclear, briefly review your Physiology notes — the pathology below will make much more sense with this foundation.
Normal Thyroid — Structure and Functional Unit
The normal adult thyroid weighs 20–30 g and has two lobes connected by an isthmus. Its functional unit is the follicle — a spherical structure lined by a single layer of follicular epithelial cells (principal cells) surrounding a central lumen filled with colloid (mostly thyroglobulin).
Follicular cell height is a direct readout of TSH stimulation:
• High TSH → tall columnar cells, scanty colloid ("active" follicle)
• Low TSH → flat squamous-like cells, abundant colloid ("resting" follicle)
Scattered between follicles are parafollicular C-cells (calcitonin-secreting) — important for thyroid cancer discussions but not central here.
Blood supply is rich (four thyroid arteries), which explains why bruits are audible over a hyperplastic gland in Graves disease.
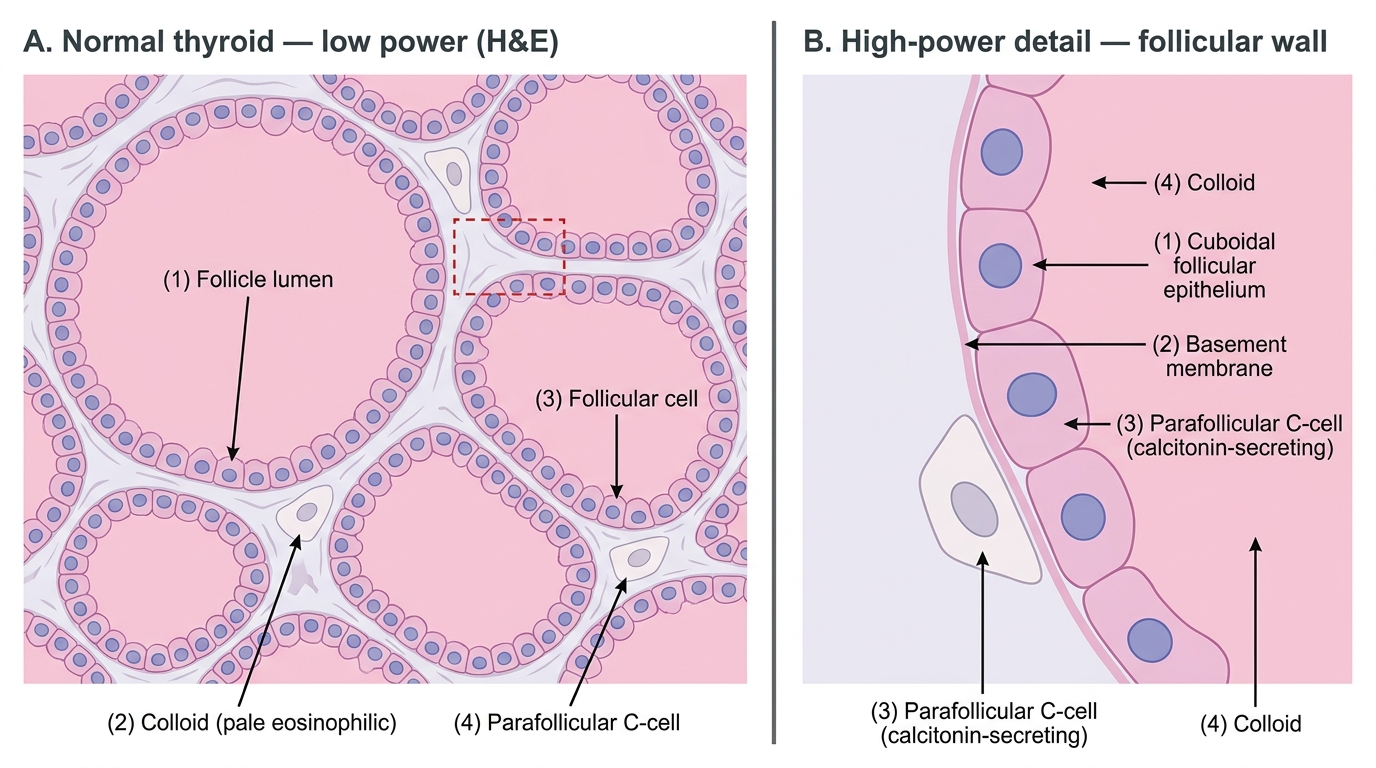
Normal Thyroid Histology (H&E) — Follicular Architecture and Cell Types
Classification of Thyroid Swellings (PA31.1)
A goiter (struma) is any enlargement of the thyroid gland. Classification is essential for NMC examinations and clinical practice:
By functional status:
| Type | TSH | T3/T4 | Clinical State |
|---|---|---|---|
| Nontoxic goiter | ↑ or normal | Normal | Euthyroid |
| Toxic goiter | ↓ (suppressed) | ↑↑ | Hyperthyroid |
| Hypothyroid goiter | ↑↑ | ↓↓ | Hypothyroid |
By morphology (Robbins classification):
1. Diffuse nontoxic (simple/colloid) goiter — uniform diffuse enlargement, iodine-deficient areas
2. Multinodular goiter (MNG) — irregular, nodular; the most common thyroid disease worldwide
3. Toxic diffuse goiter — Graves disease
4. Toxic multinodular goiter (Plummer disease) — autonomously functioning nodules
5. Toxic adenoma — solitary autonomous nodule
By geography: Endemic (community iodine deficiency ≥10% prevalence) vs. Sporadic (individual goitrogen exposure, dyshormonogenesis).
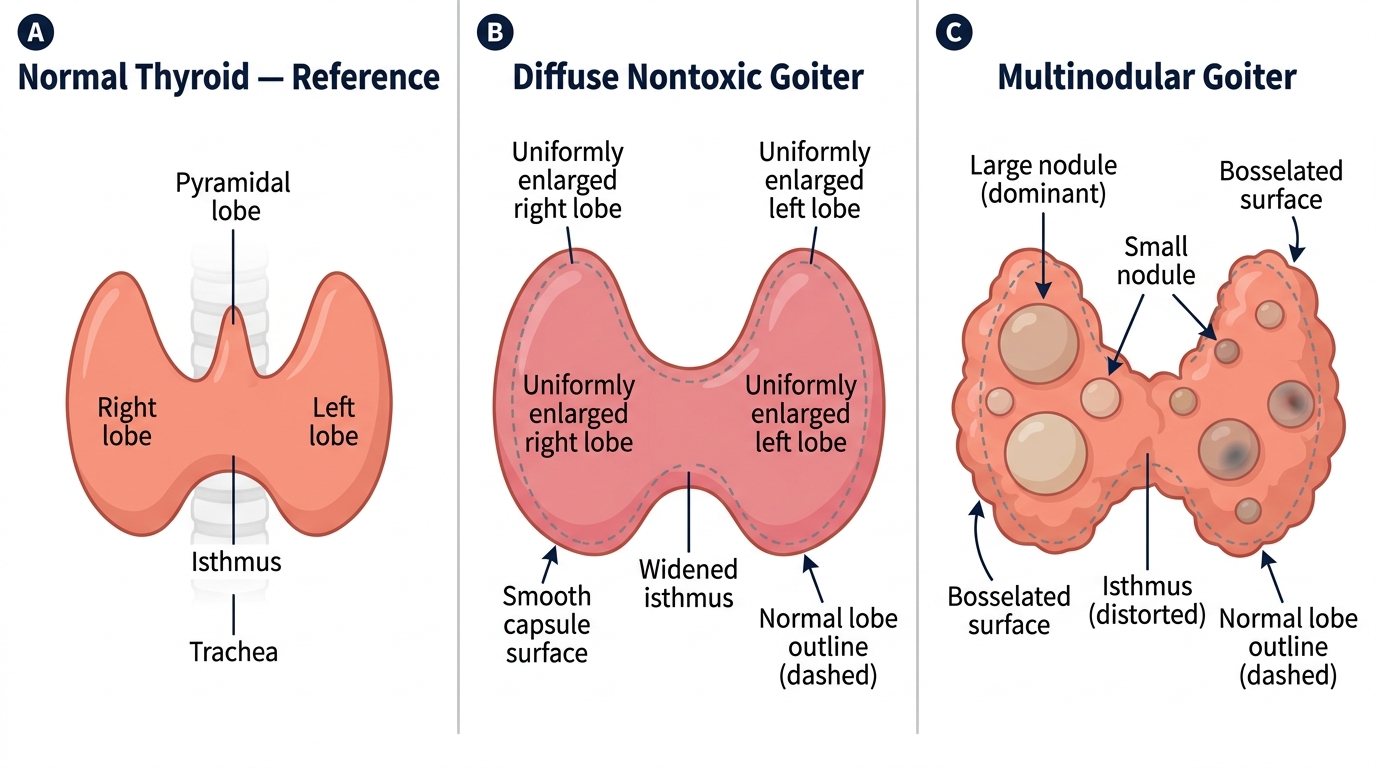
Gross Comparison: Normal Thyroid vs. Diffuse Nontoxic Goiter vs. Multinodular Goiter
Diffuse Nontoxic Goiter — Iodine Deficiency & Pathogenesis
Diffuse nontoxic (simple) goiter is the archetypical iodine-deficiency goiter and the most common cause of thyroid enlargement globally.
Iodine dependency: Dietary iodine <50 µg/day → impaired T3/T4 synthesis → compensatory ↑↑ TSH → follicular cell hyperplasia → diffuse enlargement. With iodine supplementation, hyperplastic cells involute → colloid accumulates → colloid goiter (pale, translucent, jelly-like cut surface).
Pathogenesis — two phases:
1. Hyperplastic phase: TSH-driven follicular proliferation; tall columnar cells, little colloid; gland soft and vascular
2. Colloid (involution) phase: Iodine restored (or demand decreases); follicles distend with colloid; cells flatten; gland rubbery and firm
Gross: Symmetric, smooth, weight 100–300 g, translucent amber-brown colloid on cut surface.
Micro:
• Hyperplastic phase: tall columnar epithelium, papillary infoldings, minimal colloid
• Colloid phase: distended follicles, flat epithelium, abundant dense colloid with peripheral "scalloping" (resorption vacuoles)
Clinical: Euthyroid; TSH may be at upper normal or mildly elevated; cosmetic concern; pressure symptoms (dysphagia, stridor) if large. Rarely, a colloid goiter can undergo focal hemorrhage, fibrosis, and calcification → multinodular goiter.
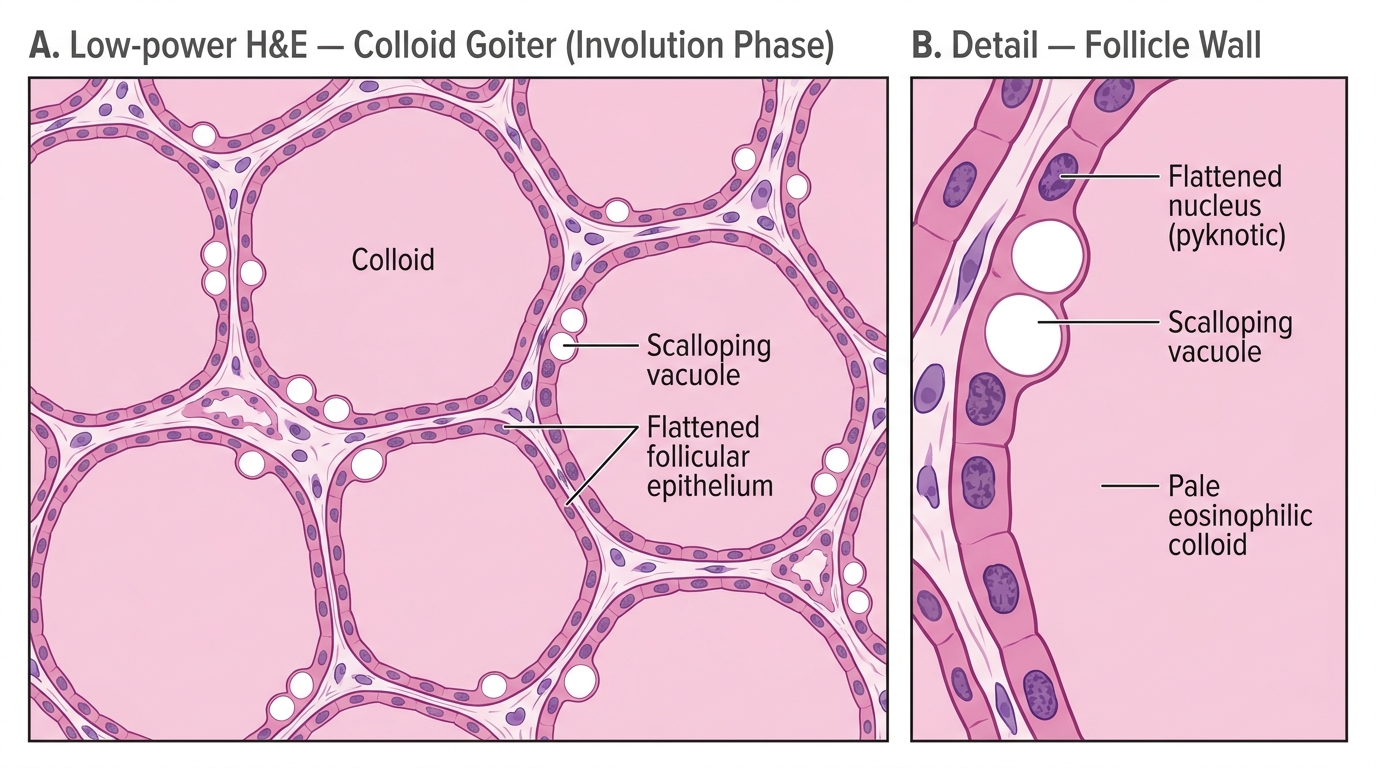
Colloid Goiter — Involution Phase: Low-Power H&E Histology