Page 2 of 26
PA31.1-3 | Thyroid: Goiter, Thyroiditis & Thyroid Function Disorders — SDL Guide (Part 2)
Multinodular Goiter — Pathogenesis and Morphology
Multinodular goiter (MNG) is the end-stage of repeated cycles of hyperplasia and involution in a gland with heterogeneous follicular cell responsiveness to TSH.
Pathogenesis:
• Over years, some follicular cells are more TSH-responsive than their neighbours → clonal expansion → nodule formation
• Nodules develop secondary changes: hemorrhage → cystic degeneration → fibrosis → calcification → ossification
• Autonomously functioning clones may eventually lose TSH dependence → toxic MNG (Plummer disease)
Gross morphology:
• Gland markedly asymmetric and bosselated (500–2,000 g in severe cases)
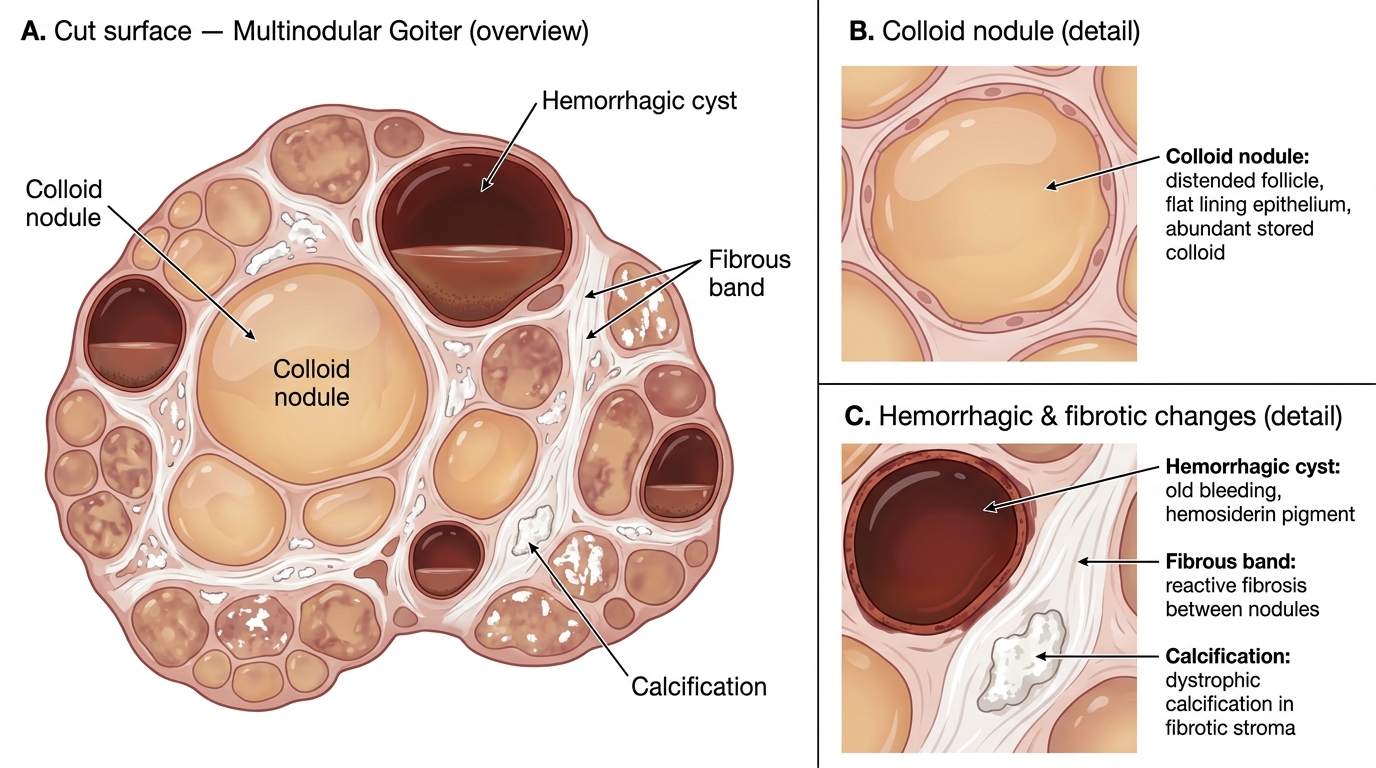
• Cut surface shows nodules of varied size with:
- Gelatinous amber colloid-filled areas
- Brown/red hemorrhagic foci
- Cystic areas (liquefied old hemorrhage)
- White fibrotic bands
- Gritty calcified speckles ("eggshell" calcification on X-ray)
Micro:
• Follicles of widely varying size — hyperplastic (tall cells, papillary infoldings) alongside involuted (flat cells, full of colloid)
• Thick fibrous capsule may surround individual nodules ("encapsulated nodule")
• Degenerative changes: cholesterol crystals, hemosiderin-laden macrophages, dystrophic calcification
Key distinction from adenoma: MNG nodules lack a complete uniform fibrous capsule, are multiple, and show varied internal architecture. A solitary encapsulated nodule with uniform architecture = follicular adenoma.
Gross Pathology of Multinodular Goiter — Cut Surface Features
CLINICAL PEARL
The Plummer–Vinson connection and iodine supplementation paradox: In severe iodine-deficient MNG, sudden iodine supplementation (e.g., after iodinized salt introduction) can precipitate hyperthyroidism in autonomously functioning nodules — the Jod-Basedow phenomenon. This is because the previously substrate-starved autonomous clones now have excess iodine to synthesise T3/T4 uninhibited by TSH. Clinical implication: introduce iodine supplementation gradually in endemic goiter populations.
SELF-CHECK
A 45-year-old farmer from a hilly district presents with a 15-year-old large neck swelling. On FNAC, smears show follicles of varying sizes — some distended with abundant colloid and flat epithelium, others lined by tall columnar cells with papillary infoldings. There are hemosiderin-laden macrophages and cholesterol crystals. The most likely diagnosis is:
A. Follicular adenoma — encapsulated, uniform follicular architecture
B. Multinodular goiter — mixed hyperplastic and involuted follicles with degenerative changes
C. Hashimoto thyroiditis — lymphocytic infiltrate and Hürthle cells expected
D. Papillary thyroid carcinoma — nuclear grooves and pseudoinclusions expected
Reveal Answer
Answer: B. Multinodular goiter — mixed hyperplastic and involuted follicles with degenerative changes
The key findings — mixed hyperplastic and involuted follicles, hemosiderin macrophages, cholesterol crystals — point to multinodular goiter. The diversity of follicle sizes reflects repeated cycles of hyperplasia and involution. A follicular adenoma has uniform architecture and a complete fibrous capsule. Hashimoto requires lymphoid follicles with germinal centres and Hürthle cell metaplasia. PTC needs nuclear features (grooves, inclusions, ground-glass nuclei). Long duration in an iodine-deficient area seals the diagnosis.
Hashimoto Thyroiditis — Autoimmune Hypothyroidism (PA31.1, PA31.3)
Hashimoto thyroiditis (chronic lymphocytic thyroiditis) is the most common thyroid disease in iodine-replete populations and the most common cause of hypothyroidism in adults.
Epidemiology: Female:male = 10–20:1; peak in middle age; HLA-DR3 and HLA-DR5 associations.
Pathogenesis — autoimmune:
Both T-cell and B-cell mediated:
• CD8+ cytotoxic T cells directly kill follicular cells
• CD4+ Th1 cells recruit macrophages; IFN-γ and TNF-α amplify damage
• Autoantibodies: anti-TPO (anti-microsomal, >95% positive) and anti-thyroglobulin (60–70% positive) — useful diagnostic markers; exact pathogenic role debated (complement activation, ADCC)
• Net result: progressive follicular destruction → fibrosis → hypothyroidism
Gross: Diffusely enlarged, firm, pale yellow-tan, lobulated gland; weight 200–300 g.
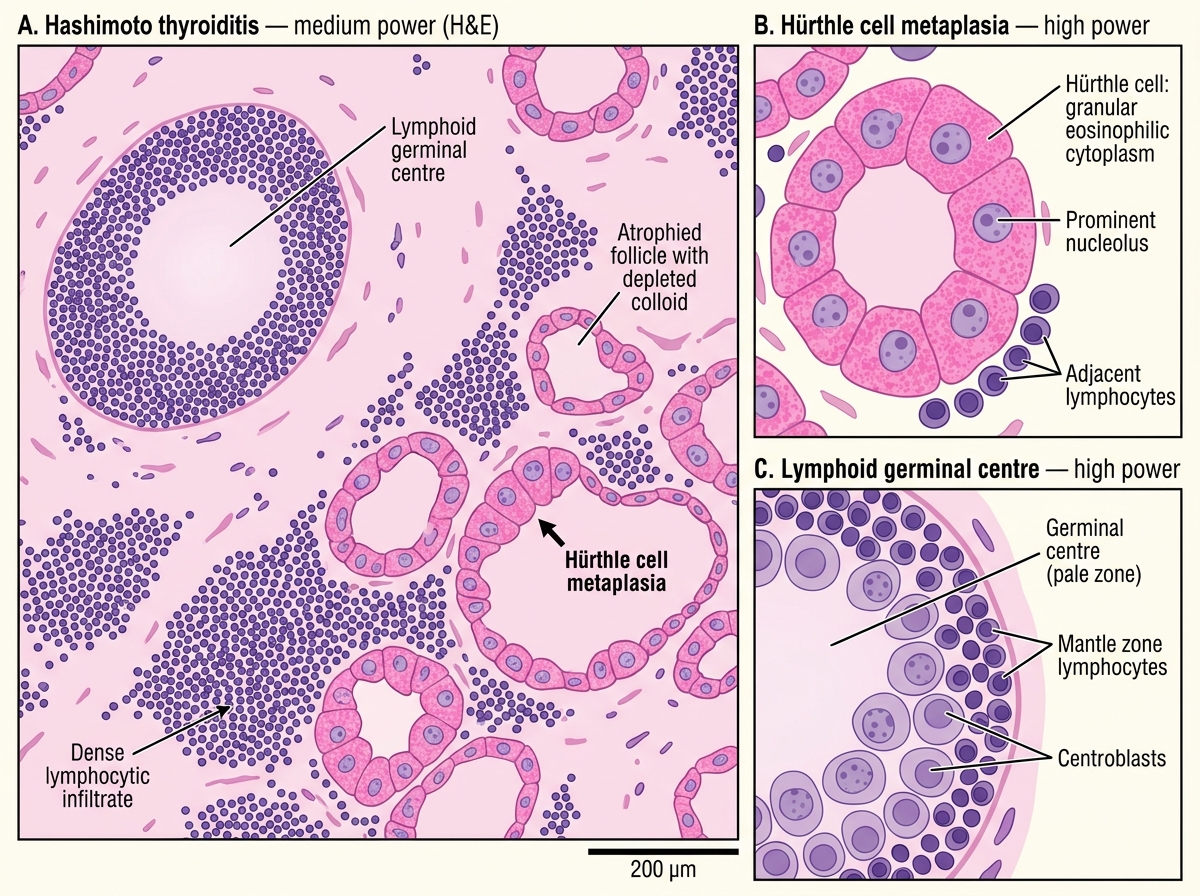
Microscopic hallmarks (learn these for OSCE):
1. Diffuse lymphocytic infiltrate with prominent germinal centres (lymphoid follicles within thyroid parenchyma)
2. Hürthle cell (oxyphilic/Askanazy cell) metaplasia of follicular epithelium — large cells with abundant granular eosinophilic cytoplasm (mitochondria-packed); nuclei may be enlarged and irregular
3. Atrophied thyroid follicles — depleted colloid, reduced size
4. Interstitial fibrosis (variable)
Lab: High TSH, low free T4, markedly elevated anti-TPO antibodies.
Course: Hypothyroidism is the natural endpoint. Small but real risk of primary thyroid lymphoma (MALToma) arising from the chronic lymphoid infiltrate — presents as rapidly enlarging thyroid in a patient with known Hashimoto.
Hashimoto Thyroiditis — H&E Histology (Medium Power with High-Power Insets)
Other Forms of Thyroiditis
Subacute granulomatous thyroiditis (de Quervain thyroiditis)
Etiology: Viral infection (Coxsackievirus, mumps, adenovirus) — follows an URTI by 2–4 weeks.
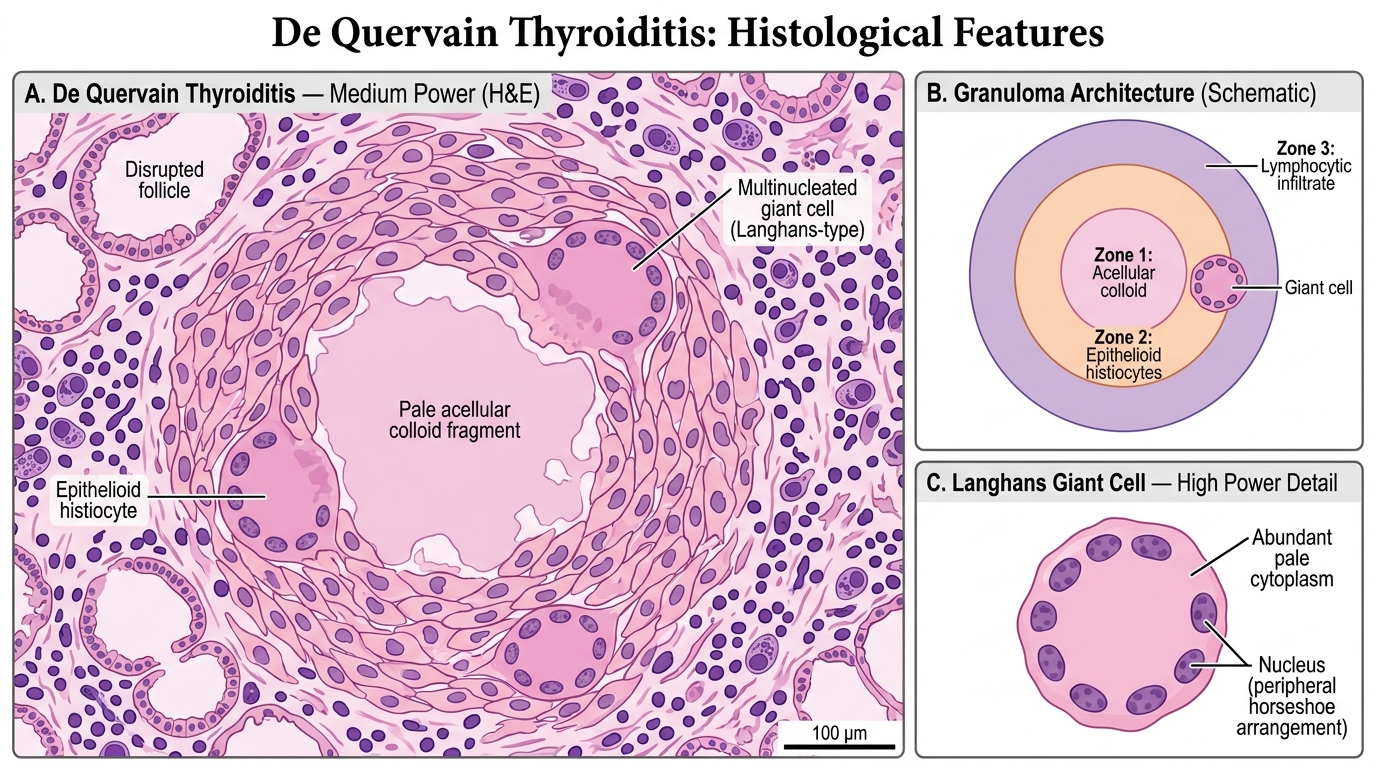
Pathogenesis: Viral damage → follicular rupture → extravasation of colloid → foreign-body giant-cell reaction around colloid.
Micro: Granulomas with central colloid fragments surrounded by epithelioid histiocytes and multinucleated giant cells; adjacent follicular disruption; neutrophilic infiltration early.
Clinical course: Classic 4-phase thyroid function evolution:
1. Toxic phase (4–8 wk): follicular damage → colloid release → T3/T4 surge → hyperthyroidism; RAIU suppressed
2. Euthyroid phase (2–4 wk)
3. Hypothyroid phase (4–8 wk): depleted stores → transient hypothyroidism
4. Recovery phase: complete restoration in >90%
Key distinction: Painful thyroid + raised ESR + post-viral onset + transient hyperthyroid → de Quervain.
Subacute lymphocytic (painless/silent) thyroiditis
• Autoimmune; associated with postpartum thyroiditis (within 1 year of delivery)
• Micro: lymphocytic infiltrate WITHOUT germinal centres, WITHOUT Hürthle cell change (unlike Hashimoto)
• Course: same 4-phase evolution as de Quervain but painless and self-limiting
• Anti-TPO may be mildly positive
Riedel thyroiditis (fibrous thyroiditis)
• Rare; dense hyaline fibrosis replaces thyroid parenchyma and extends into perithyroidal soft tissue (muscles, vessels, trachea)
• "Rock-hard" thyroid — clinically mimics carcinoma or lymphoma
• Part of IgG4-related systemic disease spectrum (fibroinflammatory disease)
• Micro: paucicellular sclerosis with abundant dense collagen, scattered lymphocytes, obliterative phlebitis
Histology of Subacute Granulomatous (de Quervain) Thyroiditis — Medium Power H&E
CLINICAL PEARL
The "thyroiditis hyperthyroidism" trap: Medical students frequently confuse thyroiditis-associated hyperthyroidism with Graves disease. The key distinguishing feature is RAIU (radioactive iodine uptake):
• Thyroiditis (de Quervain, postpartum): low/suppressed RAIU — gland is inflamed and not actively trapping iodine; T3/T4 is from passive leakage
• Graves disease: high RAIU — gland is actively stimulated by TSI antibodies to trap iodine and synthesise hormone
Anti-thyroid drugs (carbimazole, PTU) have no role in thyroiditis-associated hyperthyroidism because synthesis is NOT increased — only β-blockers for symptom relief.
SELF-CHECK
A 28-year-old woman presents 3 months after delivery with fatigue, constipation, and weight gain. Thyroid is non-tender and slightly enlarged. TSH is 12 mU/L, free T4 is low, anti-TPO is weakly positive. RAIU is 1.2% at 24 hours (normal: 15–35%). Six months later, her thyroid function tests normalize without treatment. The most likely diagnosis is:
A. Hashimoto thyroiditis — permanent hypothyroidism expected
B. Postpartum (subacute lymphocytic) thyroiditis — transient hypothyroid phase
C. Subacute granulomatous thyroiditis — painful thyroid expected
D. Riedel thyroiditis — rock-hard thyroid with compression symptoms expected
Reveal Answer
Answer: B. Postpartum (subacute lymphocytic) thyroiditis — transient hypothyroid phase
Postpartum subacute lymphocytic thyroiditis is the correct answer. The classic clues are: postpartum onset (within 1 year), painless thyroid, low RAIU despite hypothyroidism (gland not actively trapping iodine — damaged follicles leaking stored hormone earlier, now depleted), mild anti-TPO positivity, and spontaneous recovery. Hashimoto causes permanent hypothyroidism and has markedly elevated anti-TPO. De Quervain is painful with raised ESR. Riedel presents as a hard fixed mass, not soft and diffuse.