Page 3 of 26
PA31.1-3 | Thyroid: Goiter, Thyroiditis & Thyroid Function Disorders — SDL Guide (Part 3)
Graves Disease — Pathogenesis and Morphology (PA31.2)
Graves disease (diffuse toxic goiter) is the most common cause of hyperthyroidism and a prototypical organ-specific autoimmune disease.
Epidemiology: F:M = 7–10:1; peak 20–40 years; HLA-DR3, HLA-B8 association.
Autoimmune pathogenesis — the TSI antibody:
• CD4+ Th2 cells stimulate autoreactive B cells to produce thyroid-stimulating immunoglobulins (TSI) — IgG antibodies that bind the TSH receptor (TSHR) on follicular cells
• TSI mimics TSH → persistent receptor activation → cAMP pathway → unregulated T3/T4 synthesis and secretion
• Unlike TSH, TSI is NOT subject to negative feedback → sustained hyperthyroidism
• Also: TSH-receptor blocking antibodies (in some patients, same antigen, different epitope → hypothyroidism)
Gross morphology:
• Diffusely enlarged, symmetric, firm, red-brown (hyperemic) gland — 35–60 g
• Markedly increased vascularity → bruit on auscultation (thyroid bruit = clinical sign of Graves)
Microscopic hallmarks:
1. Tall, crowded columnar follicular cells — marked cellular hypertrophy
2. Papillary infoldings into follicular lumen (without fibrovascular cores — NOT true papillae of carcinoma)
3. Scalloped/pale colloid — peripheral resorption vacuoles at cell-colloid interface (colloid being actively endocytosed)
4. Lymphocytic infiltrate in interstitium (autoimmune component)
5. May have germinal centres (overlap with Hashimoto in long-standing cases)
Pre-treatment hallmark: After antithyroid drug treatment (PTU/carbimazole), colloid reaccumulates and cells flatten — gland "involutes" before surgery.
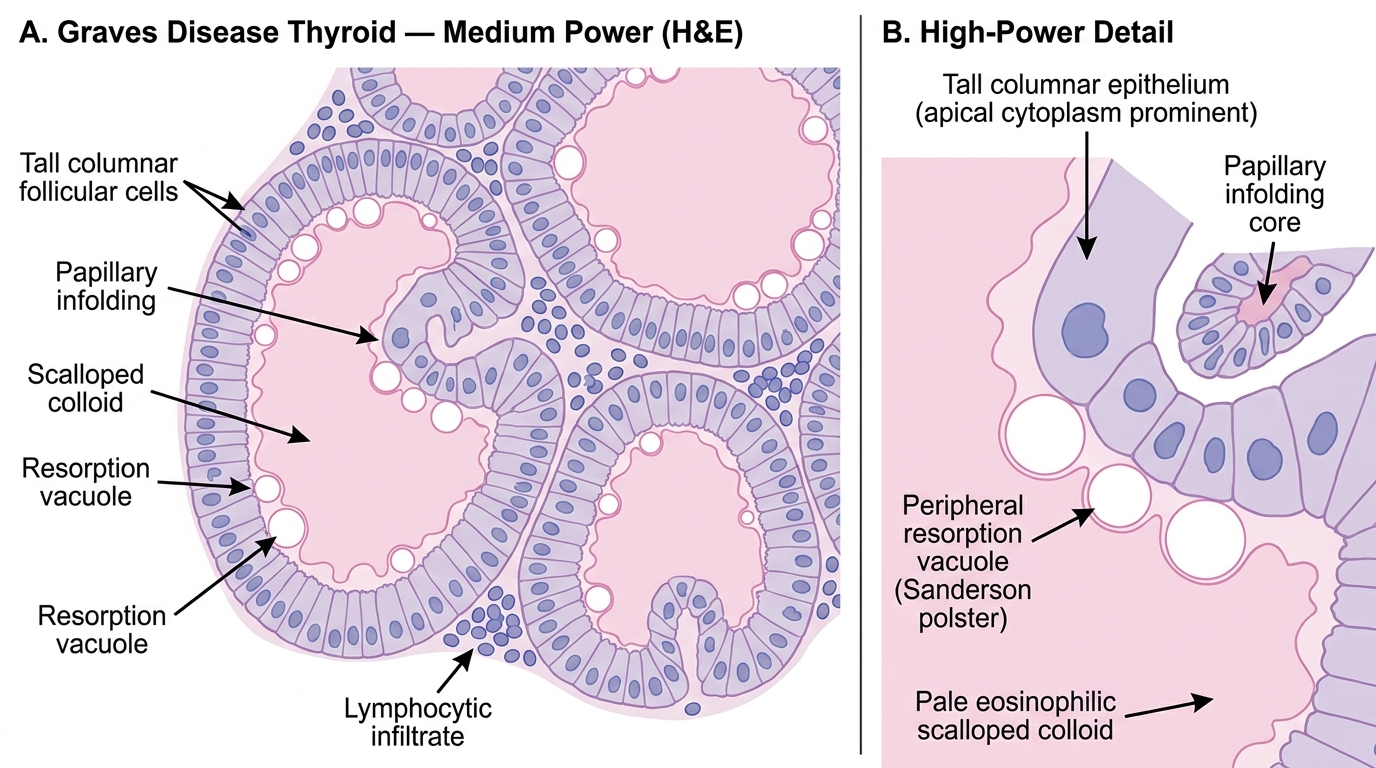
Histology of Graves Disease Thyroid (H&E, Medium Power)
Graves Disease — Extrathyroidal Manifestations
Graves disease is a systemic autoimmune condition with three classic extrathyroidal features:
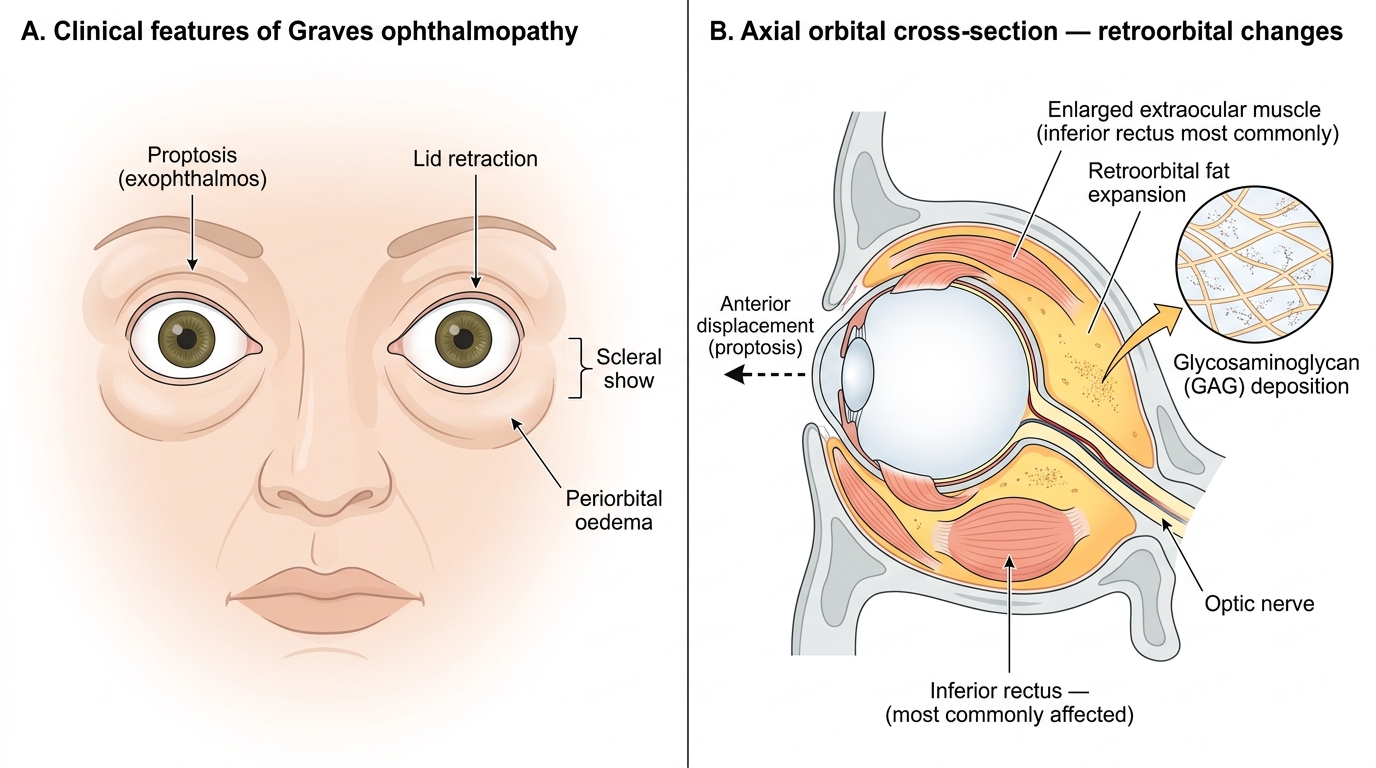
1. Graves ophthalmopathy (thyroid eye disease):
• Autoantibodies cross-react with TSHR on orbital fibroblasts → fibroblast activation → glycosaminoglycan (hyaluronate) deposition in retroorbital fat and extraocular muscles → proptosis (exophthalmos), periorbital oedema, diplopia
• Occurs in ~50% of Graves patients; can worsen AFTER thyroid treatment (immune rebound)
• May persist/progress even when thyrotoxicosis is controlled
• Corneal exposure → keratitis if severe
2. Graves dermopathy (pretibial myxedema):
• TSI stimulates dermal fibroblasts → mucin (glycosaminoglycan) deposition in dermis
• Thickened, indurated orange-peel texture skin over pretibial area
• Present in <5%; associated with severe ophthalmopathy
3. Thyroid acropachy:
• Rare; clubbing of fingers + soft tissue swelling of hands/feet + periosteal new bone formation
• Triplet of acropachy + dermopathy + ophthalmopathy = highly specific for Graves
TSI detection: Detected as TRAb (TSH receptor antibodies) by competition assay or as TSI by bioassay. Positive in >95% of untreated Graves.
Graves Ophthalmopathy: Clinical Features and Orbital Pathology
Thyrotoxicosis — Causes, Clinical Features & Pathophysiology (PA31.2)
Thyrotoxicosis is the clinical state caused by excess thyroid hormones in tissues, regardless of source.
Causes (memorise the RAIU pattern — it's the diagnostic key):
| Cause | TSH | Free T4 | RAIU | Mechanism |
|---|---|---|---|---|
| Graves disease | ↓↓ | ↑↑ | ↑↑ diffuse | TSI-driven overproduction |
| Toxic MNG | ↓↓ | ↑↑ | ↑ patchy | Autonomous nodules |
| Toxic adenoma | ↓↓ | ↑↑ | ↑ focal "hot" nodule | Autonomous adenoma |
| De Quervain thyroiditis | ↓↓ | ↑↑ | ↓↓ suppressed | Passive leakage from damaged follicles |
| Factitious thyrotoxicosis | ↓↓ | ↑↑ | ↓↓ suppressed | Exogenous T4 (thyroglobulin ↓) |
| TSH-secreting pituitary adenoma | ↑ | ↑↑ | ↑ | Secondary (very rare) |
Clinical manifestations — "sympathetic storm" + hypermetabolism:
• Cardiovascular: tachycardia, wide pulse pressure, high-output cardiac failure, atrial fibrillation (T3 directly shortens action potential in atrial myocytes)
• Neurological/psychiatric: anxiety, tremor, emotional lability, hyperreflexia, insomnia
• Metabolic: weight loss despite increased appetite (↑ basal metabolic rate), heat intolerance, excessive sweating
• Musculoskeletal: proximal myopathy, thyrotoxic periodic paralysis (hypokalemia, more common in Asian males)
• Skin/hair: fine hair, moist skin, onycholysis (Plummer nails)
• Reproductive: oligomenorrhea, reduced fertility; gynaecomastia in males
• Ocular (Graves-specific): proptosis, lid lag, lid retraction, Stellwag sign (infrequent blinking)
Thyroid storm (thyrotoxic crisis): Acute exacerbation — hyperpyrexia, delirium, cardiovascular collapse; mortality ~20% with treatment, >90% untreated.
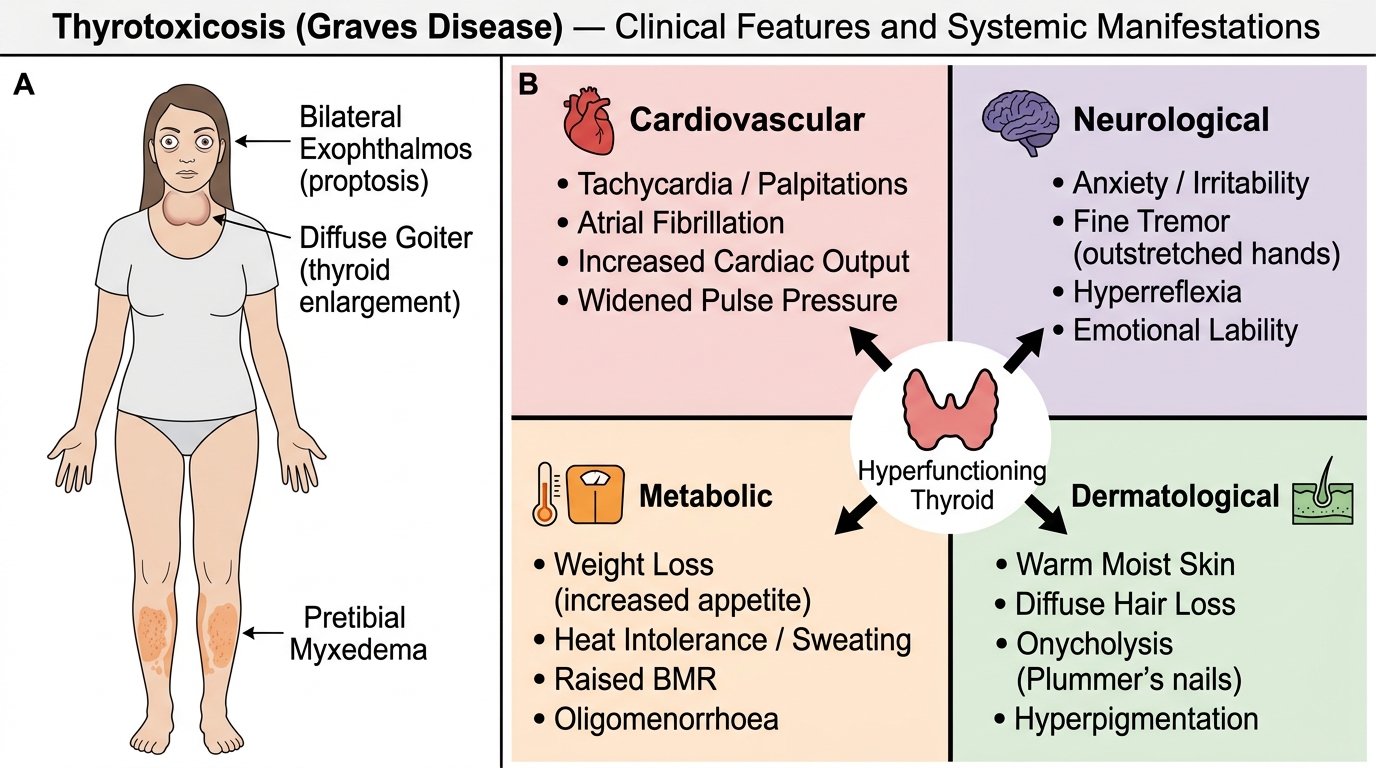
Thyrotoxicosis (Graves Disease): Clinical Triad and Organ-System Manifestations