Page 4 of 26
PA31.1-3 | Thyroid: Goiter, Thyroiditis & Thyroid Function Disorders — SDL Guide (Part 4)
Hypothyroidism — Causes, Clinical Features & Laboratory Findings (PA31.3)
Hypothyroidism is deficient thyroid hormone action on tissues. It is classified by level of axis failure:
Primary hypothyroidism (>99% of cases — thyroid itself is deficient):
1. Hashimoto thyroiditis — most common in iodine-replete regions (autoimmune destruction)
2. Iodine deficiency — most common worldwide (impaired synthesis)
3. Post-radioiodine/post-surgical — iatrogenic ablation
4. Dyshormonogenesis — congenital enzyme defects (e.g., thyroid peroxidase mutations)
5. Goitrogens — dietary (cassava, cabbage — thiocyanates), drugs (lithium, amiodarone, PTU overdose)
Secondary hypothyroidism (pituitary failure → ↓TSH → thyroid underactivation)
Tertiary hypothyroidism (hypothalamic failure → ↓TRH)
Clinical manifestations — "metabolic slowdown":
• Cardiovascular: bradycardia, low-voltage ECG, pericardial effusion
• Neurological: lethargy, cognitive slowing, depression, cerebellar ataxia
• Metabolic: weight gain (not due to true obesity — mainly myxoedema fluid), cold intolerance, ↑ LDL cholesterol
• Skin/hair: dry coarse skin, hair loss, non-pitting myxoedema (mucin deposition in dermis), puffy face, macroglossia, hoarse voice
• Reproductive: menorrhagia, infertility, elevated prolactin (TRH also stimulates PRL)
• Neuromuscular: delayed relaxation of deep tendon reflexes ("hung-up" reflexes), carpal tunnel syndrome
Special form — Congenital hypothyroidism (cretinism): Iodine deficiency or thyroid agenesis in utero → irreversible intellectual disability + stunted growth. Neonatal TSH screening (Guthrie card) enables early thyroxine replacement and prevents neurological damage.
Laboratory findings:
• Primary: ↑TSH (most sensitive early marker), ↓ free T4
• Secondary/tertiary: ↓TSH, ↓ free T4
• Dyslipidaemia: ↑ LDL-C, ↑ triglycerides
• ↑ CK (muscle myopathy), ↑ serum prolactin
Myxoedema coma: End-stage severe hypothyroidism — hypothermia, bradycardia, CO2 retention, altered consciousness; medical emergency.
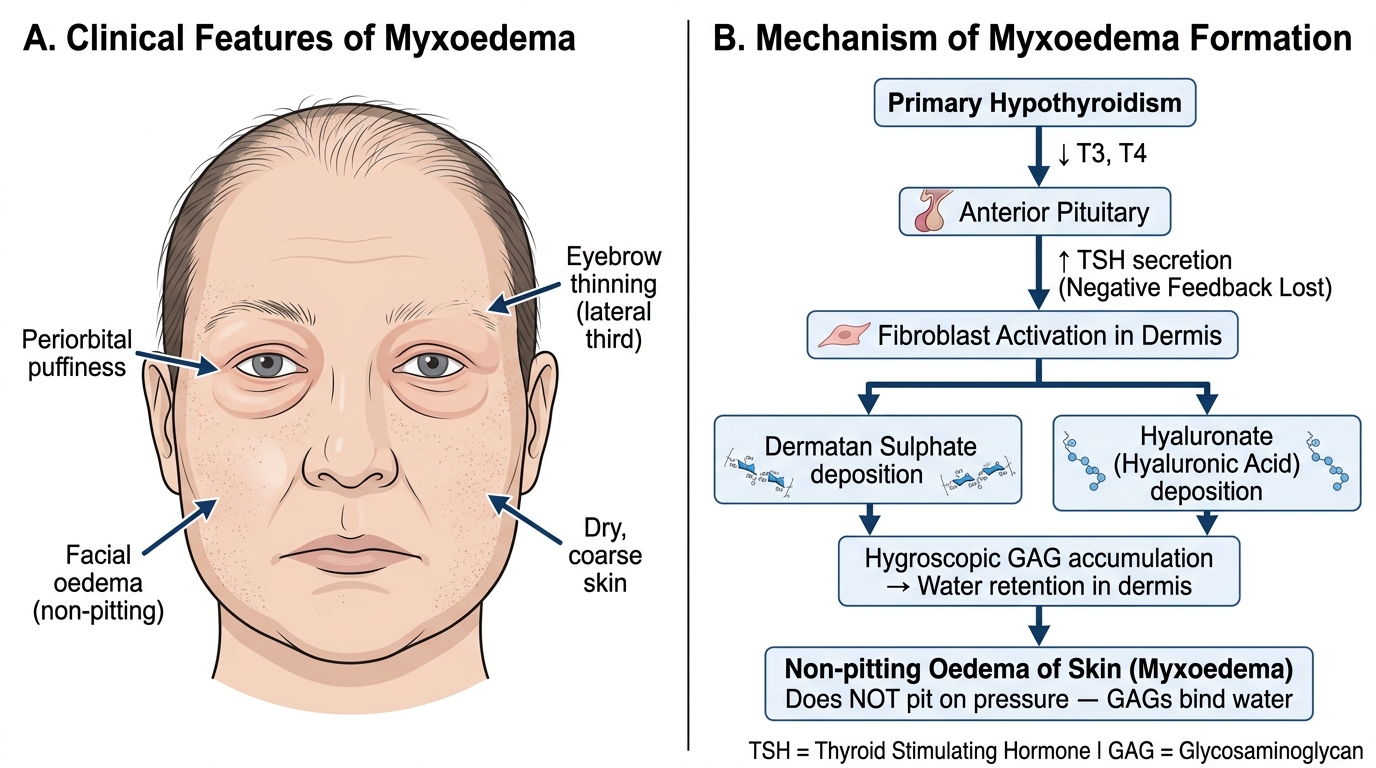
Myxoedema: Clinical Features and Pathophysiological Mechanism
Thyrotoxicosis vs. Hypothyroidism — Integrated Comparison
This comparison table is your rapid-revision anchor. Examiners love asking you to distinguish the two:
| Feature | Thyrotoxicosis | Hypothyroidism |
|---|---|---|
| Heart rate | Tachycardia, AF | Bradycardia |
| Weight | Loss (↑ appetite) | Gain (↓ appetite) |
| Temperature tolerance | Heat intolerance, sweating | Cold intolerance, dry skin |
| Skin | Warm, moist, fine | Dry, coarse, myxoedematous |
| Hair | Fine, brittle, diffuse loss | Coarse, brittle, outer third eyebrow loss |
| Deep tendon reflexes | Hyperreflexia, fast relaxation | Hyporeflexia, delayed relaxation |
| Bowel | Diarrhoea, hyperdefecation | Constipation |
| Menstruation | Oligomenorrhoea | Menorrhagia |
| TSH | ↓↓ (primary) or ↑ (TSH-oma) | ↑↑ (primary) or ↓ (secondary) |
| Free T4 | ↑↑ | ↓↓ |
| RAIU | ↑ (Graves) or ↓ (thyroiditis) | ↓ (not used diagnostically) |
| Cholesterol | ↓ LDL | ↑ LDL |
| Most common cause | Graves disease | Hashimoto thyroiditis (iodine-replete) / iodine deficiency (worldwide) |
Memory hook for reflexes: In hyperthyroidism, everything is fast — fast heart, fast gut, fast reflexes. In hypothyroidism, everything is slow — but the reflex relaxation phase is disproportionately slow (hallmark sign on physical examination).
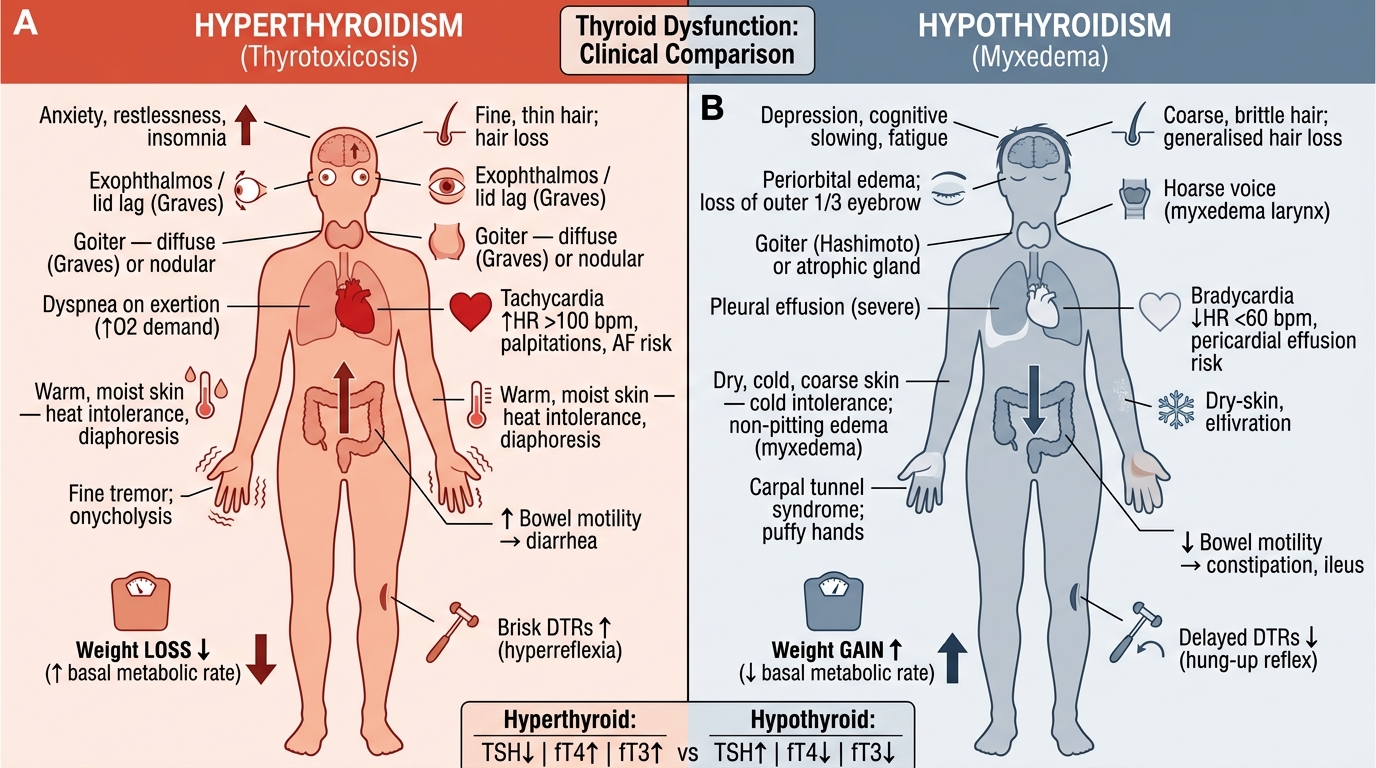
Hyperthyroidism vs. Hypothyroidism — Systemic Clinical Features
Laboratory & Imaging Interpretation in Thyroid Disorders
Thyroid Function Tests — interpretation framework:
Step 1: TSH — the most sensitive screening test for primary thyroid dysfunction
• TSH ↑ → primary hypothyroidism (or recovery phase of thyroiditis)
• TSH ↓ → hyperthyroidism (or central hypothyroidism — rare)
• TSH normal → euthyroid in most circumstances
Step 2: Free T4 (and free T3 if indicated)
• Confirms and quantifies the degree of dysfunction
• Free T3 is useful in T3-toxicosis (autonomous nodules may preferentially secrete T3)
Step 3: Antibodies
• Anti-TPO ↑↑ → Hashimoto (or Graves overlap)
• TRAb/TSI positive → Graves disease (>95% sensitivity)
• Anti-thyroglobulin → less specific
RAIU (Radioactive Iodine Uptake):
• Measures gland's iodine-trapping capacity (reflects TSH stimulation or autonomous activity)
• Technique: administer 123I tracer; measure uptake at 6 h and 24 h
• High RAIU + homogeneous scan → Graves
• High RAIU + focal "hot" nodule → toxic adenoma
• High RAIU + patchy, nodular → toxic MNG
• Low/suppressed RAIU → thyroiditis, factitious, iodine excess (Wolff-Chaikoff effect)
Thyroid Ultrasound:
• Graves: diffusely enlarged, hypoechoic gland, markedly ↑ vascularity on Doppler ("thyroid inferno")
• MNG: multiple nodules of varying echogenicity ± cystic change ± calcification
• Hashimoto: heterogeneous, hypoechoic parenchyma with echogenic fibrous septa, ↓ vascularity
FNAC (Fine Needle Aspiration Cytology):
• Standard for evaluating thyroid nodules (Bethesda classification)
• Hashimoto: lymphocytes, Hürthle cells, sparse follicular cells
• Graves: hyperplastic follicular cells with scant colloid (may raise concern for follicular neoplasm — clinical correlation crucial)
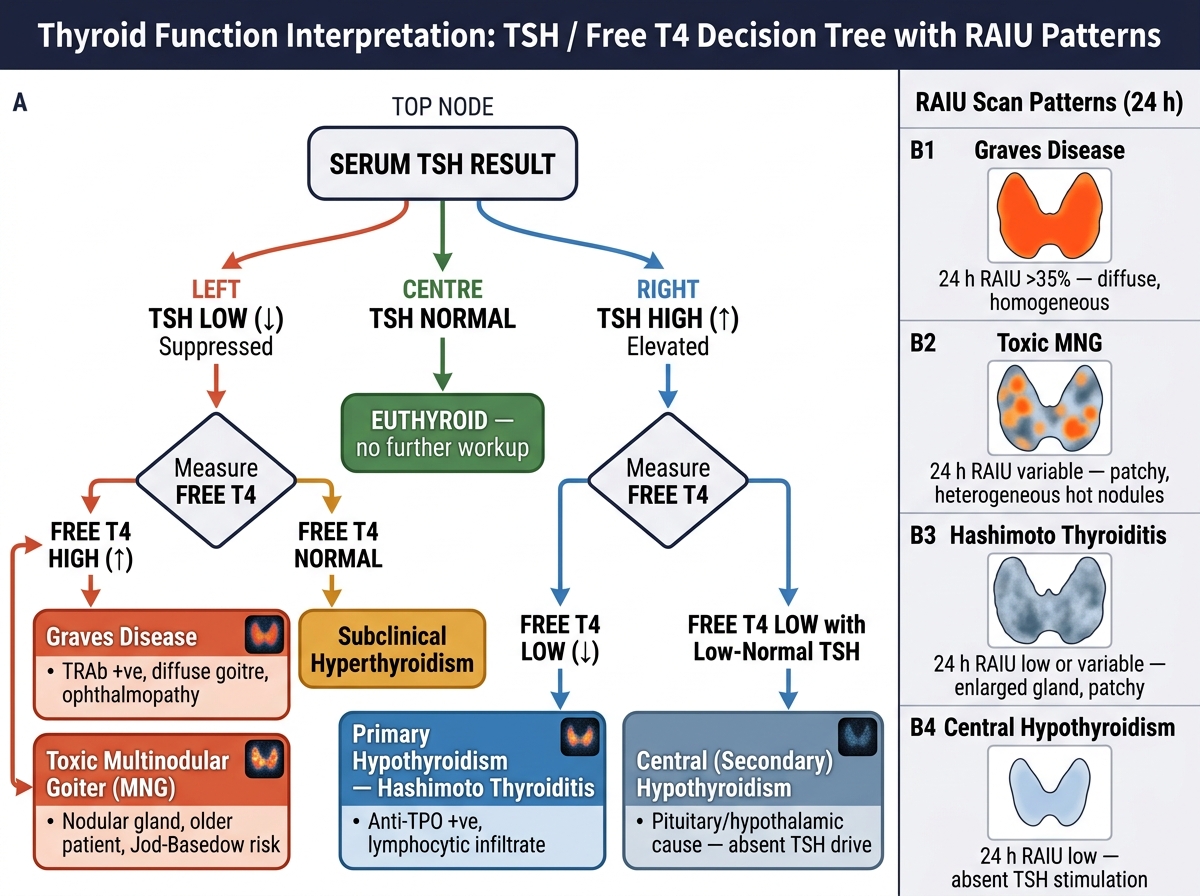
TSH / Free T4 Decision Tree with RAIU Scan Patterns
CLINICAL PEARL
Amiodarone and thyroid dysfunction — the CBME clinical link: Amiodarone (anti-arrhythmic) contains 37% iodine by weight. It causes thyroid dysfunction in up to 30% of patients via two mechanisms:
• Amiodarone-induced hypothyroidism (AIH): Wolff-Chaikoff effect — excess iodine acutely inhibits thyroid peroxidase → blocks T3/T4 synthesis; more common in Hashimoto patients (impaired escape mechanism)
• Amiodarone-induced thyrotoxicosis Type 1 (AIT-1): Iodine load drives excess hormone synthesis in underlying MNG or Graves (Jod-Basedow)
• AIT-2: Direct toxic destructive thyroiditis from amiodarone → colloid leakage → RAIU suppressed
Distinguishing AIT-1 vs AIT-2 guides treatment (antithyroid drugs vs. steroids). This is a real exam favourite in combined pharmacology–pathology questions.
SELF-CHECK
A 32-year-old woman presents with 6 months of palpitations, 5 kg weight loss, heat intolerance, and protrusion of both eyes. Examination reveals a diffusely enlarged smooth thyroid with a bruit, lid lag, and tremor. Labs: TSH undetectable, free T4 markedly elevated, TRAb strongly positive. RAIU at 24 hours = 68% (normal 15–35%). Which finding on thyroid histology would you expect?
A. Dense lymphocytic infiltrate with germinal centres and Hürthle cell metaplasia
B. Granulomas with central colloid and multinucleated giant cells
C. Tall crowded columnar follicular cells with papillary infoldings and scalloped pale colloid
D. Paucicellular dense hyaline fibrosis extending into perithyroidal tissues
Reveal Answer
Answer: C. Tall crowded columnar follicular cells with papillary infoldings and scalloped pale colloid
This is classic Graves disease: diffuse goiter + bruit (high vascularity) + bilateral proptosis + undetectable TSH + high free T4 + strongly positive TRAb + high RAIU (TSI drives active iodine trapping). The hallmark histology is option C — tall crowded columnar cells with papillary infoldings (pseudopapillae, not true papillae) and scalloped pale colloid from active endocytosis. Option A is Hashimoto (lymphocytes, germinal centres, Hürthle cells). Option B is de Quervain (granulomas). Option D is Riedel (paucicellular fibrosis).