Page 6 of 26
PA31.{4,6} | Thyroid Tumors & Parathyroid Disease — SDL Guide
Learning Objectives
- Classify thyroid neoplasms (adenoma vs. carcinoma) and distinguish major carcinoma subtypes by pathogenesis, histology, spread pattern, and prognosis
- Describe the classic nuclear features of papillary thyroid carcinoma (Orphan-Annie-eye nuclei, nuclear grooves, pseudoinclusions) and recognize psammoma bodies
- Explain how capsular and vascular invasion distinguish follicular carcinoma from follicular adenoma
- Describe the cell of origin, molecular marker, amyloid stroma, and hereditary associations of medullary thyroid carcinoma
- Outline the approach to a thyroid nodule (FNAC, Bethesda System)
- Classify hyperparathyroidism (primary, secondary, tertiary) with causes, lab findings, and clinical manifestations
- Describe the skeletal manifestations of hyperparathyroidism including osteitis fibrosa cystica and brown tumor
- Identify the morphologic features of chief cell adenoma and chief cell hyperplasia
INSTRUCTIONS
Thyroid nodules are extraordinarily common — about 5% of adults have a palpable thyroid nodule, and up to 50% of adults have nodules detectable on ultrasound. The pathologist's report on the fine needle aspirate of that nodule shapes the entire surgical decision. Meanwhile, hypercalcemia is one of the most frequently encountered biochemical abnormalities in clinical medicine, and 90% of cases trace back to primary hyperparathyroidism or malignancy. Master the morphology in this module, and you will understand both the microscope slide and the patient's story.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 24 (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch. 28 (textbook)
- Bethesda System for Reporting Thyroid Cytopathology, 2nd ed. (2017) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 2022, a 32-year-old schoolteacher in Puducherry visited her physician for an unrelated throat infection. The doctor noticed a firm, non-tender swelling in the lower neck — a thyroid nodule she had never felt herself. An ultrasound showed it was 2.2 cm, solid, hypoechoic, with irregular margins. A fine needle aspiration cytology (FNAC) was performed and reported Bethesda Category V: suspicious for malignancy. She underwent a total thyroidectomy.
The histology: papillary columns lined by cells with strikingly clear, empty-looking nuclei and finely grooved nuclear membranes. A small, laminated, concentric calcification sat at the center of one papilla. The pathologist's report confirmed papillary thyroid carcinoma — the same tumor that Napoleon's surgeon may have missed in 1821.
At 32, with appropriate surgery and TSH suppression, her 20-year survival exceeds 95%. The key to that outcome was a pathologist who knew what those nuclei meant.
WHY THIS MATTERS
Thyroid and parathyroid pathology are high-yield areas for undergraduate pathology and appear regularly in professional examinations. More importantly, they have direct clinical impact:
- Thyroid nodules are extremely common in India — iodine sufficiency campaigns have reduced goiter but not nodule prevalence.
- Fine needle aspiration cytology (FNAC) of thyroid is a core clinical skill you will learn in surgery postings; understanding the pathology helps you counsel patients.
- Hypercalcemia is a common surgical emergency (renal stones, bony pains, confusion) — primary hyperparathyroidism is the outpatient cause, malignancy is the inpatient cause.
- The mnemonic 'stones, bones, groans, and psychic moans' is not just a memory aid — it is a complete symptom cluster that will alert you to a diagnosis before the blood test result arrives.
- NMC competencies PA31.4 and PA31.6 require you to classify, describe pathogenesis, and interpret laboratory features — this module addresses all three.
RECALL
Before we begin, let us activate what you already know from earlier in this course:
From Normal Histology: The thyroid follicle is lined by follicular (principal) cells that synthesize T3/T4, and parafollicular C cells (scattered between follicles) that secrete calcitonin. Keep this distinction in mind — each cell type gives rise to a different tumor.
From Physiology: TSH from the pituitary drives follicular cell proliferation and thyroid hormone synthesis. Prolonged TSH stimulation (as in iodine deficiency) is a growth stimulus that can initiate neoplasia.
From Biochemistry: PTH (parathyroid hormone) raises serum calcium by (a) activating osteoclasts to resorb bone, (b) increasing renal calcium reabsorption and phosphate excretion, and (c) activating vitamin D → intestinal calcium absorption. This three-pronged action explains all the lab findings in hyperparathyroidism.
From Gross Pathology (previous topics): You know that a tumor with an intact capsule behaves differently from one that has broken through its capsule. This concept is the single most important distinguishing feature between follicular adenoma and follicular carcinoma.
Thyroid Neoplasms: Overview and Classification
Thyroid neoplasms arise from one of two cell populations:
| Cell of Origin | Tumor Type |
|---|---|
| Follicular cells | Follicular adenoma, Papillary carcinoma, Follicular carcinoma, Anaplastic (undifferentiated) carcinoma |
| Parafollicular C cells | Medullary carcinoma |
The clinical starting point is always the thyroid nodule. Key epidemiology:
- ~5% of adults have a palpable thyroid nodule; ultrasound detects nodules in up to 50%
- Only 5% of thyroid nodules are malignant — the pathologist's job is to find them
- Women are affected 3–4× more than men for most thyroid cancers (except anaplastic)
- Papillary thyroid carcinoma (PTC) is the most common thyroid malignancy (~80–85% of cases)
Approach to a Thyroid Nodule:
1. Ultrasound — assess size, echogenicity, margins, calcification, vascularity (TIRADS scoring)
2. FNAC (Fine Needle Aspiration Cytology) — the diagnostic cornerstone, minimally invasive
3. Bethesda System categorizes cytology into 6 classes (I = non-diagnostic → VI = malignant) with associated malignancy risk and management guidance
4. Thyroid function tests — most thyroid carcinomas are euthyroid; a "hot" (hyperfunctioning) nodule on radionuclide scan is almost never malignant
Risk factors for malignancy in a nodule: history of head/neck irradiation, rapidly growing nodule, firmness/fixation, lymphadenopathy, age <20 or >70, male sex, family history of thyroid carcinoma or MEN2.
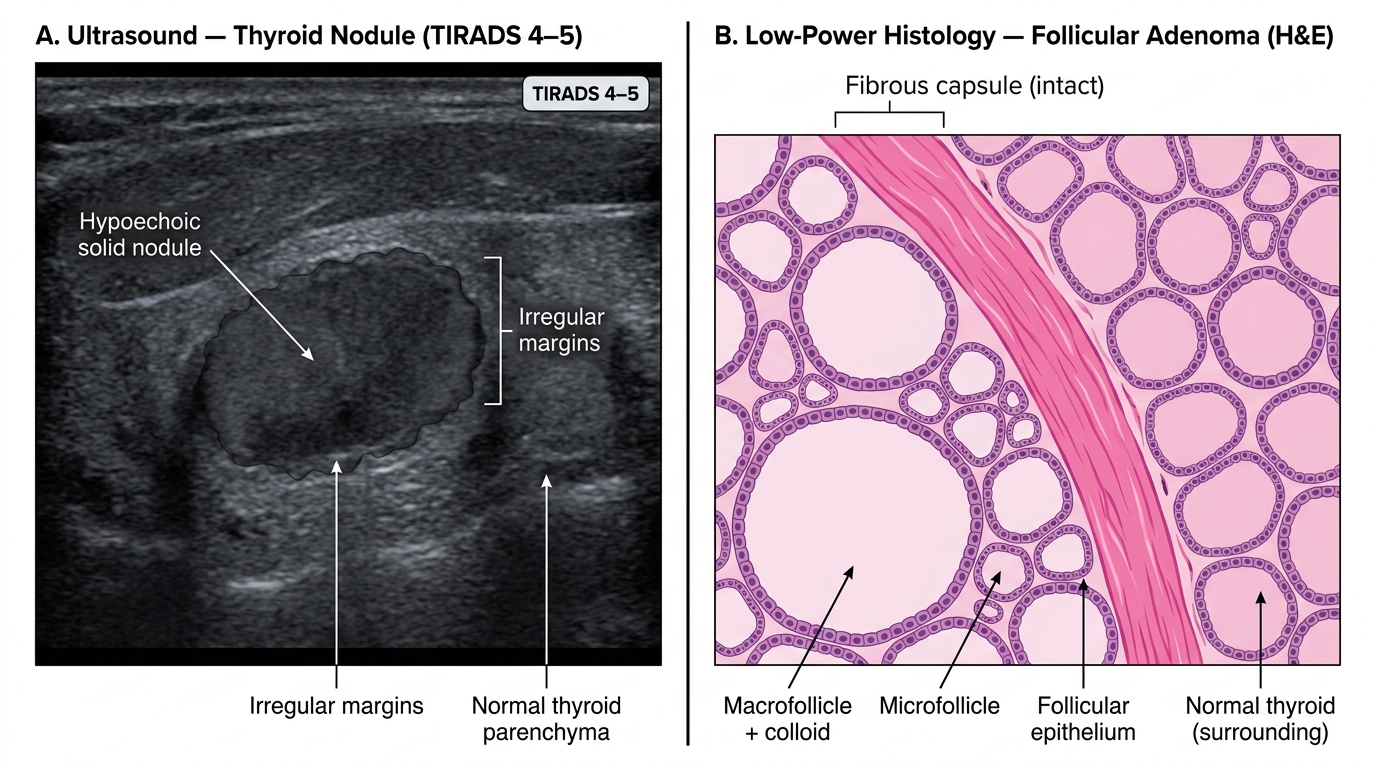
Thyroid Nodule — Ultrasound Appearance and Histological Architecture
Follicular Adenoma: The Benign Thyroid Nodule
Follicular adenoma is the most common thyroid neoplasm overall. It is a benign, solitary encapsulated tumor arising from follicular cells.
Gross pathology:
• Solitary, well-circumscribed nodule, typically 1–3 cm
• Completely surrounded by a thin, intact fibrous capsule — this is the critical gross feature
• Cut surface: pale tan, soft, sometimes with hemorrhage or cystic change
Microscopic features:
• Follicles of varying size — normal, macro-, or microfollicular pattern
• Follicular cells that may show mild nuclear atypia
• No capsular invasion, no vascular invasion — this is the defining feature that separates adenoma from carcinoma
• Colloid may be abundant (macrofollicular/simple adenoma) or scant (microfollicular/fetal adenoma)
Molecular: Some follicular adenomas have mutations in RAS oncogenes, but unlike follicular carcinomas, do not carry PAX8-PPARG translocations.
Clinical significance:
• Most patients are euthyroid
• Rarely, a toxic (hyperfunctioning) adenoma can produce excess thyroid hormone (TSH-independent autonomous nodule, driven by TSH receptor mutations)
• Adenomas do not transform into carcinomas; they are dead-end lesions
• FNAC: "follicular neoplasm" (Bethesda III/IV) — cannot distinguish adenoma from well-differentiated follicular carcinoma on cytology alone; excision is often required
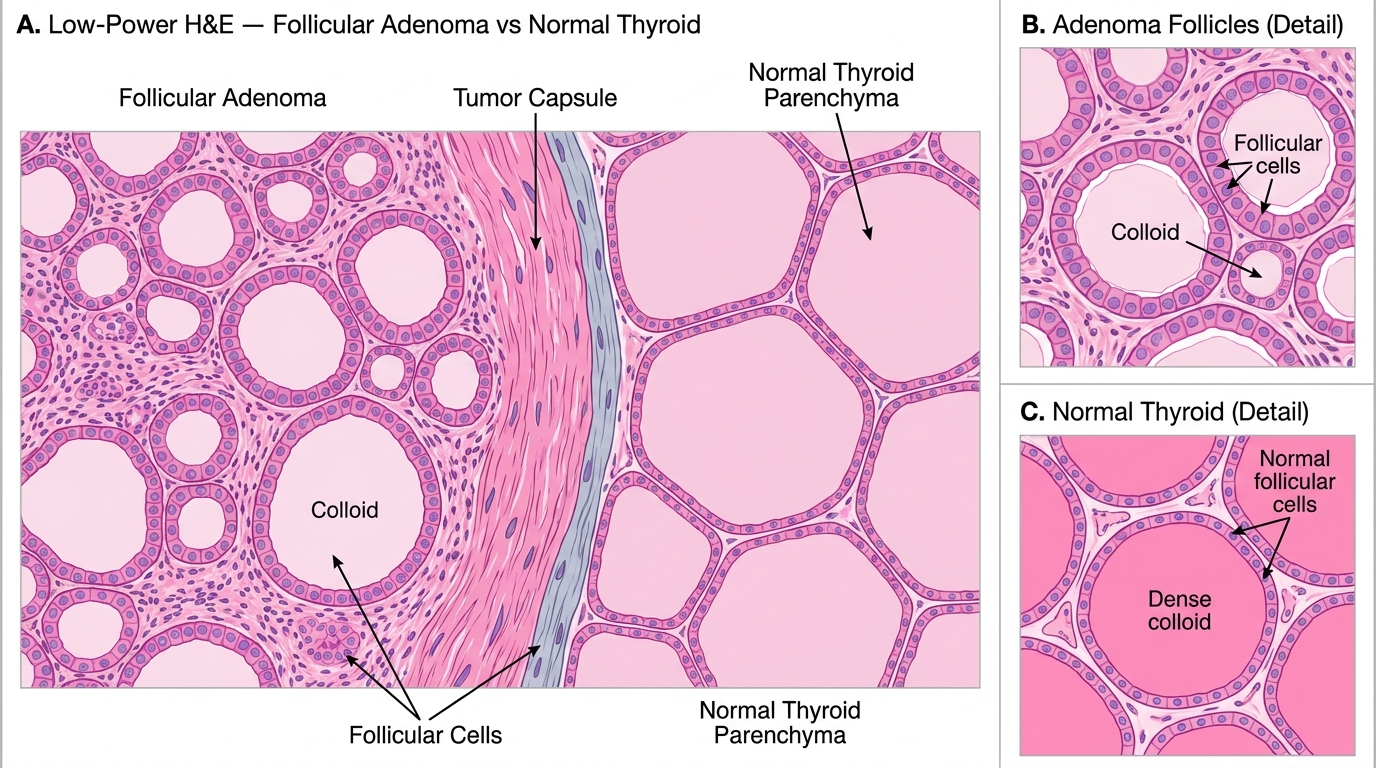
Follicular Adenoma: Low-Power Histology Showing Intact Capsule and Comparison with Normal Thyroid
Papillary Thyroid Carcinoma: The Most Common Thyroid Cancer
Papillary thyroid carcinoma (PTC) accounts for 80–85% of all thyroid carcinomas. Despite being a carcinoma, it carries an excellent prognosis (20-year survival >95% for localized disease).
Epidemiology & Etiology:
• Most common in women aged 20–50
• Ionizing radiation to the head/neck is the best established risk factor (e.g., post-Chernobyl pediatric PTC surge, historical neck irradiation for thymic enlargement)
• Mutations: BRAF V600E (most common, ~60% of PTCs) and RET/PTC rearrangements (especially in radiation-associated and pediatric PTCs)
Gross pathology:
• Poorly demarcated, infiltrative mass — no true capsule
• Firm, white–grey, gritty (due to calcifications)
• Multifocal in ~20% of cases
Microscopic features — MEMORIZE THESE:
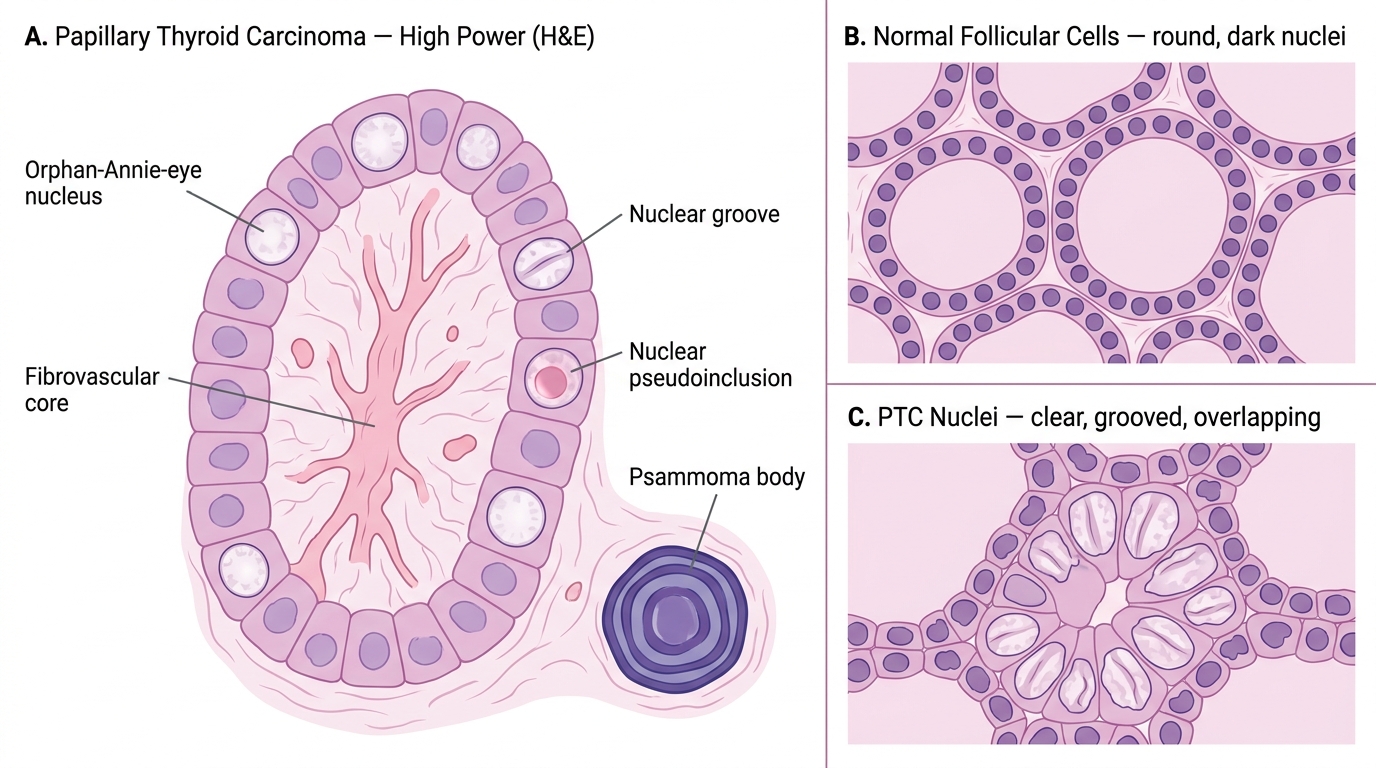
- Papillary architecture — branching papillae with fibrovascular cores lined by tumor cells. (Note: some PTCs are follicular variant and lack papillae; the nuclear features still make the diagnosis.)
- Orphan-Annie-eye nuclei (optically clear nuclei) — large, pale, empty-appearing nuclei due to dispersion of fine chromatin to the nuclear periphery. Named after the blank white eyes in the comic strip character. Pathognomonic of PTC.
- Nuclear grooves — linear infoldings of the nuclear membrane, seen as grooves on cross-section
- Nuclear pseudoinclusions — cytoplasmic invaginations into the nucleus, appearing as eosinophilic round inclusions within the nucleus
- Psammoma bodies — concentrically laminated, basophilic calcifications within papillae, formed by calcification of necrotic tumor cells. Seen in ~40–50% of PTCs. Highly specific for PTC when found in a thyroid FNAC.
Spread: Predominantly lymphatic — cervical lymph node metastases are common at presentation. Lymph node metastasis does NOT worsen prognosis significantly in well-differentiated PTC.
Variants of clinical importance:
• Follicular variant — entirely follicular architecture but with classic PTC nuclear features; same prognosis
• Tall cell variant — aggressive; cells are twice as tall as wide; more common in elderly
• Microcarcinoma — ≤1 cm; often incidental finding; excellent prognosis
Prognosis: Excellent in young patients with localized disease. Risk stratification by AGES score or TNM stage guides radioiodine ablation decisions.
Histological Features of Papillary Thyroid Carcinoma
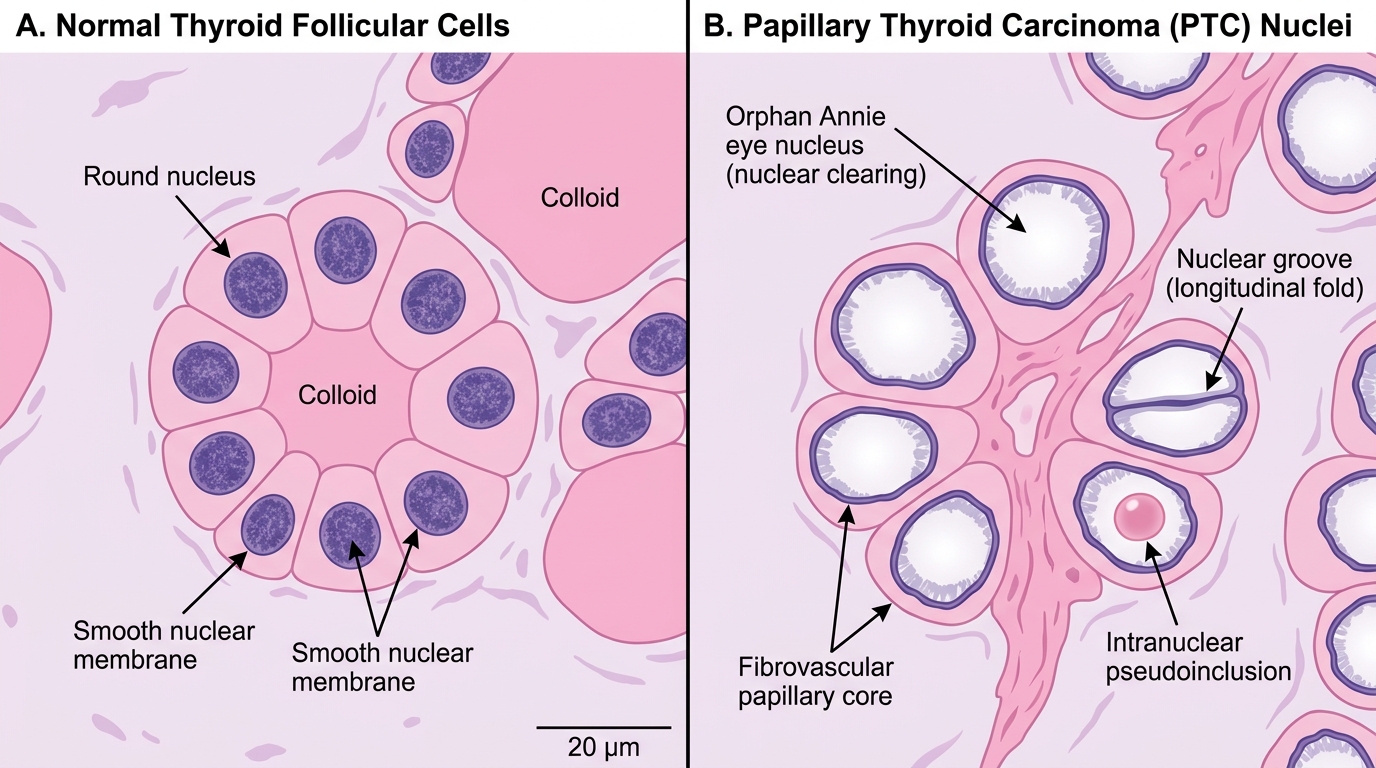
Nuclear Features of Papillary Thyroid Carcinoma — Normal vs. PTC (H&E, ×400)
CLINICAL PEARL
The nuclear features of PTC trump architecture. The follicular variant of papillary carcinoma has entirely follicular architecture — it looks like a follicular neoplasm at first glance. But on high power, the nuclei are classic: optically clear, grooved, with pseudoinclusions. A pathologist who looks only at the architecture will miss the diagnosis. Always screen the nucleus carefully before calling a thyroid lesion a follicular neoplasm.
Practical tip: Psammoma bodies in a thyroid FNAC are almost pathognomonic for papillary carcinoma — they are not a feature of benign nodular goiter or follicular neoplasms. If you see concentric, laminated calcifications in cytology, escalate urgency immediately.
SELF-CHECK
A 28-year-old woman undergoes FNAC of a 1.8 cm thyroid nodule. Smears show cells with large, pale, empty-looking nuclei with nuclear grooves and a concentric laminated calcific body. What is the most likely diagnosis?
A. Follicular adenoma
B. Papillary thyroid carcinoma
C. Medullary thyroid carcinoma
D. Hashimoto thyroiditis
Reveal Answer
Answer: B. Papillary thyroid carcinoma
The cytological triad of optically clear (Orphan-Annie-eye) nuclei, nuclear grooves, and psammoma bodies is pathognomonic for papillary thyroid carcinoma. Follicular adenoma lacks these nuclear features. Medullary carcinoma shows plasmacytoid/spindle cells with amyloid. Hashimoto thyroiditis shows Hürthle cells and lymphocytes.