Page 7 of 26
PA31.{4,6} | Thyroid Tumors & Parathyroid Disease — SDL Guide (Part 2)
Follicular Thyroid Carcinoma: When Invasion Defines Malignancy
Follicular thyroid carcinoma (FTC) accounts for 10–15% of thyroid carcinomas. The critical teaching point: you cannot diagnose follicular carcinoma on cytology alone — the diagnosis requires histologic demonstration of invasion.
Why? Follicular carcinoma and follicular adenoma look identical on cytology (both show follicular cells, may show microfollicular pattern). The only features that prove malignancy are:
- Capsular invasion — tumor cells penetrating through the fibrous capsule (must be full-thickness breach, not just pushing up against it)
- Vascular invasion — tumor thrombi within capsular blood vessels lined by endothelium
Classification by invasion extent:
| Type | Invasive Features | Metastatic Risk |
|---|---|---|
| Minimally invasive | Limited capsular ± vascular invasion | Low (<5% metastasis) |
| Widely invasive | Broad fronts of capsular breach, extensive vascular invasion | High (30–50% distant metastasis) |
Gross pathology:
• Solitary, encapsulated mass — indistinguishable from adenoma grossly unless invasion is evident
• Widely invasive forms may infiltrate thyroid parenchyma extensively
Molecular: RAS mutations (30–45%) and PAX8-PPARG translocation (30–35%) are characteristic. BRAF mutations are absent (helps distinguish from PTC follicular variant).
Spread: Hematogenous — metastases to lungs and bones are characteristic ("cannon ball" lung mets, lytic/sclerotic bone mets). Lymph node metastasis is much less common than in PTC.
Prognosis: Worse than PTC for widely invasive forms. Minimally invasive FTC has an excellent prognosis similar to adenoma after resection.
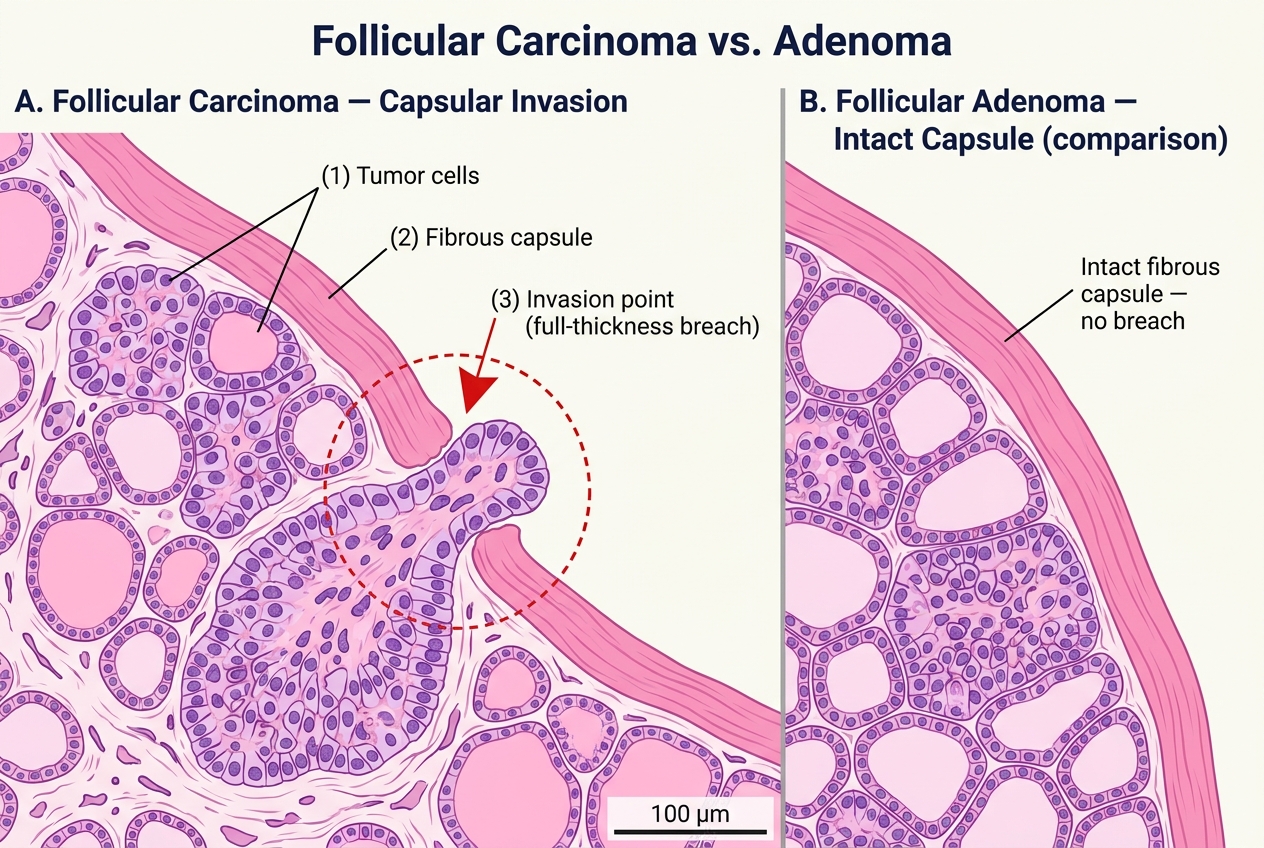
Capsular Invasion in Follicular Thyroid Carcinoma vs. Intact Capsule in Follicular Adenoma (H&E, Medium Power)
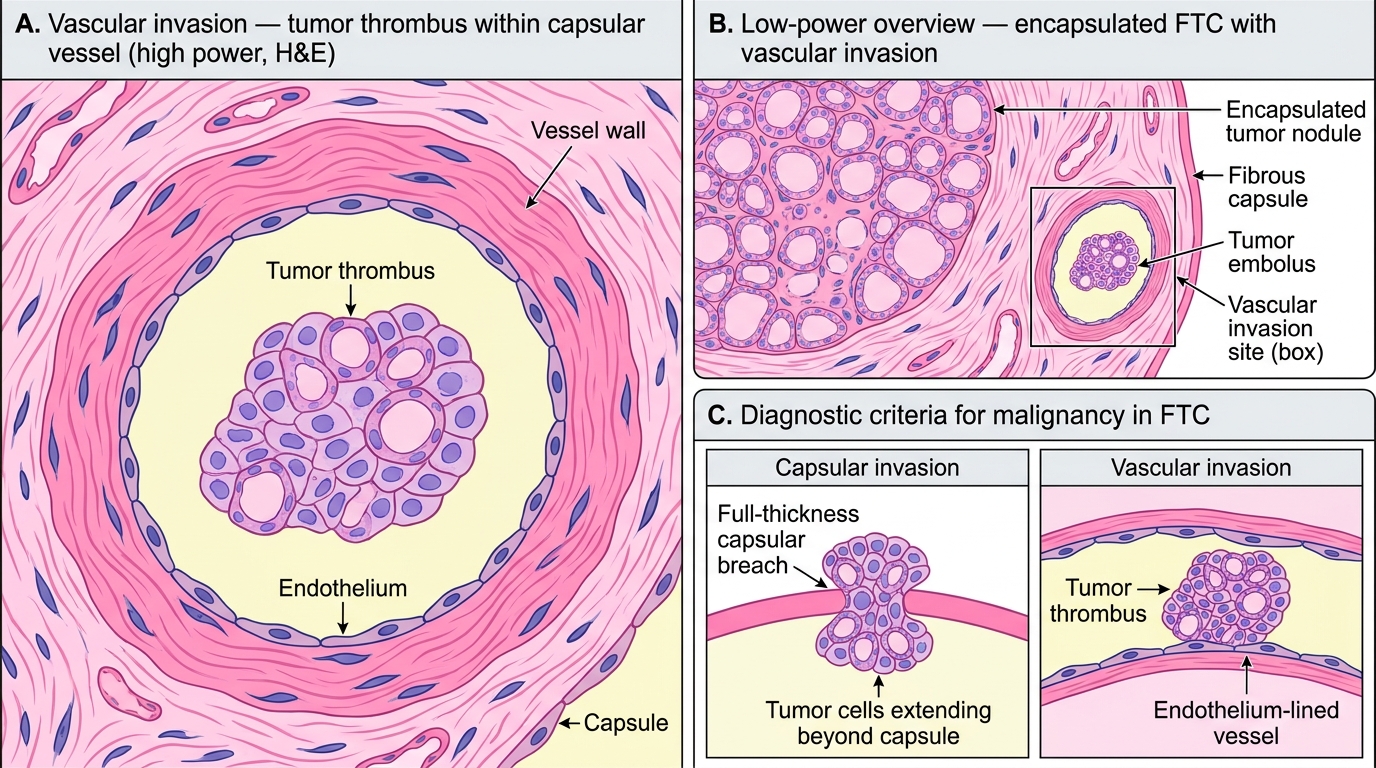
Vascular Invasion in Follicular Thyroid Carcinoma: Diagnostic Histology
Medullary Thyroid Carcinoma: The Calcitonin-Secreting Tumor
Medullary thyroid carcinoma (MTC) arises from parafollicular C cells — the calcitonin-secreting cells scattered between thyroid follicles. It accounts for 5–10% of thyroid carcinomas but is clinically distinct and critically important because of its hereditary associations.
Two forms:
| Feature | Sporadic MTC | Hereditary MTC |
|---|---|---|
| Frequency | ~75% | ~25% |
| Age | 40–60s | Younger (childhood–30s) |
| Laterality | Usually unilateral | Often bilateral and multifocal |
| Precursor | — | C-cell hyperplasia → MTC |
| Mutation | Somatic RET | Germline RET point mutation |
Hereditary MTC occurs in three settings:
1. MEN2A (Sipple syndrome) — MTC + bilateral pheochromocytoma + parathyroid hyperplasia
2. MEN2B — MTC + pheochromocytoma + mucosal neuromas + marfanoid habitus
3. Familial MTC — MTC alone, no other endocrine tumors
All hereditary MTC is caused by germline RET proto-oncogene point mutations. Genetic testing of family members is mandatory.
Gross pathology:
• Firm, gray-white mass; often bilateral in hereditary forms
Microscopic features:
1. Sheets, nests, or trabeculae of uniform polygonal to spindle cells (no follicle formation — remember, C cells don't make thyroid hormone)
2. Amyloid stroma — the hallmark. Amyloid here consists of polymerized calcitonin precursor peptides (calcitonin amyloid, stained with Congo red, shows apple-green birefringence under polarized light)
3. Fine stippled ("salt-and-pepper") chromatin — a neuroendocrine pattern
4. May show carcinoid-like architecture
Biochemical marker: Serum calcitonin — elevated in virtually all cases; used for diagnosis, staging, and post-operative follow-up. Carcinoembryonic antigen (CEA) is also elevated and correlates with prognosis.
Prognosis: Intermediate — better than anaplastic, worse than PTC. 10-year survival ~60–80% for localized disease, but poor with distant metastases.
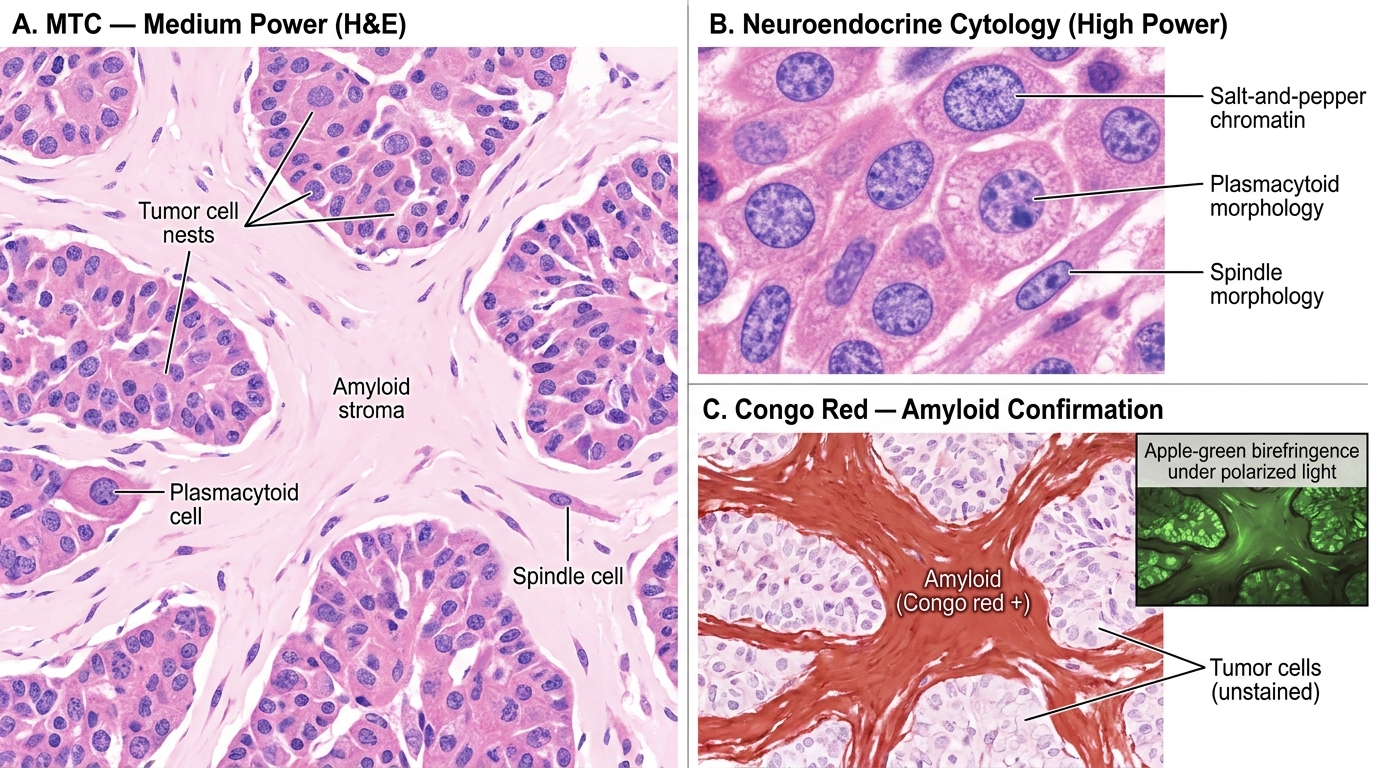
Medullary Thyroid Carcinoma — H&E Histology and Amyloid Confirmation
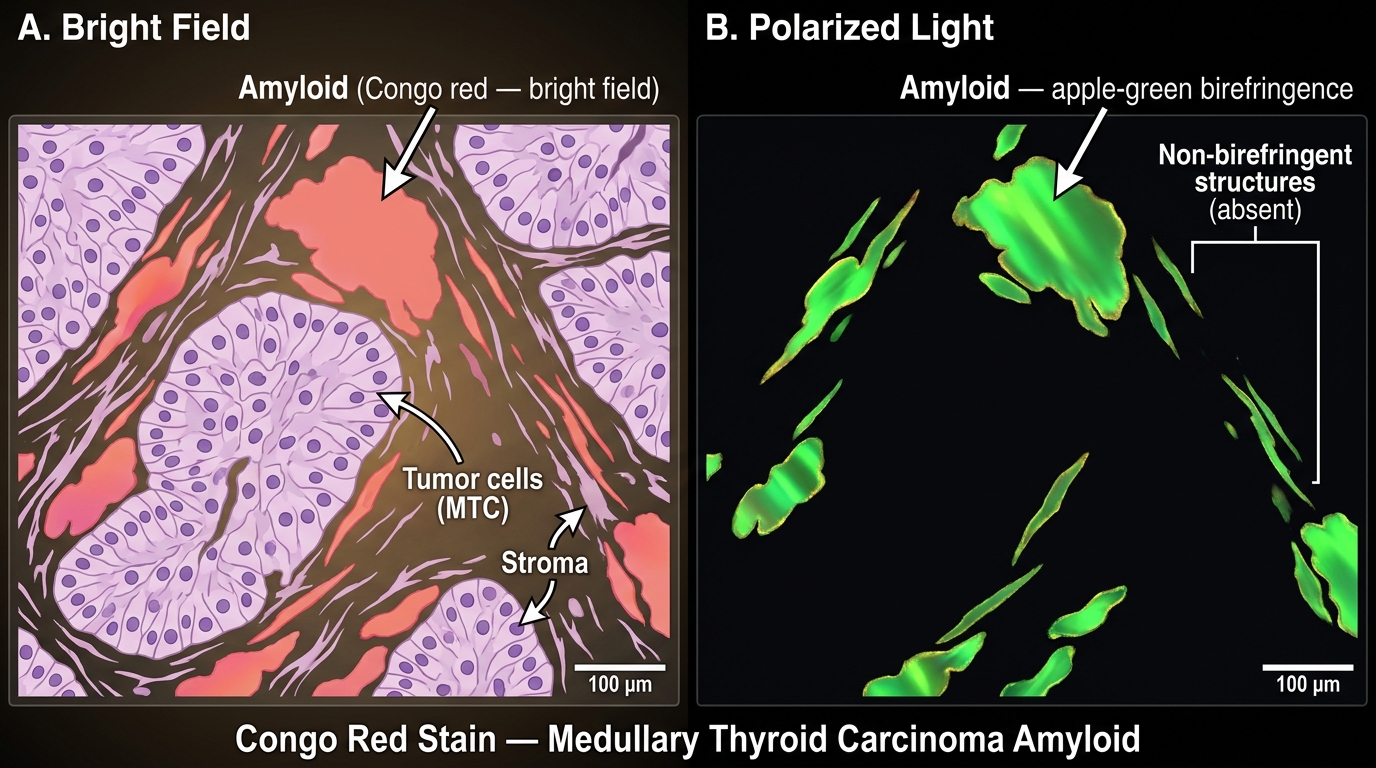
Congo Red Stain: Amyloid in Medullary Thyroid Carcinoma — Bright Field vs. Polarized Light
CLINICAL PEARL
MEN2A family screening saves lives. When a patient is diagnosed with MTC, the pathologist's report triggers a cascade: genetic testing for RET mutation, screening all first-degree relatives, and prophylactic thyroidectomy in mutation-positive family members — ideally before age 5 years for high-risk mutations. A young person's "routine" thyroid carcinoma may be the sentinel event that saves multiple family members.
Calcitonin paradox: MTC secretes large amounts of calcitonin, yet patients rarely develop hypocalcemia. Why? Because calcitonin's bone-resorption inhibition is far outweighed by PTH and other calcium regulatory mechanisms in the long term. Serum calcitonin is useful as a tumor marker, not a calcium regulator in this context.
Anaplastic Thyroid Carcinoma: The Most Aggressive Thyroid Tumor
Anaplastic (undifferentiated) thyroid carcinoma is rare (~1–2% of thyroid carcinomas) but constitutes one of the most lethal human malignancies. It does not respond to radioiodine or TSH suppression.
Key features:
- Age: Almost exclusively in patients >65 years of age — a thyroid carcinoma in an elderly patient that is rapidly enlarging must raise this diagnosis
- Pathogenesis: Often arises by dedifferentiation from pre-existing well-differentiated thyroid carcinoma (PTC or FTC), with acquisition of additional mutations (TP53, BRAF, CTNNB1)
- Presentation: Rapidly enlarging neck mass, dysphagia, dyspnea, stridor from tracheal compression, and hoarseness (recurrent laryngeal nerve invasion)
Gross: Large, infiltrative mass replacing much of the thyroid; frequently extends into adjacent soft tissues, trachea, esophagus
Microscopic features:
• Markedly pleomorphic, high-grade cells in three possible patterns:
1. Giant cell — bizarre, multinucleated giant cells with atypical mitoses
2. Spindle cell — sarcomatoid appearance
3. Squamoid — focal squamous differentiation
• Abundant mitoses and necrosis
• Complete loss of thyroid follicular differentiation (negative for thyroglobulin on IHC)
Prognosis: Uniformly fatal. Median survival is 3–6 months from diagnosis. No effective systemic therapy exists, though BRAF-targeted therapy (dabrafenib + trametinib) shows modest benefit in BRAF V600E-mutant cases.
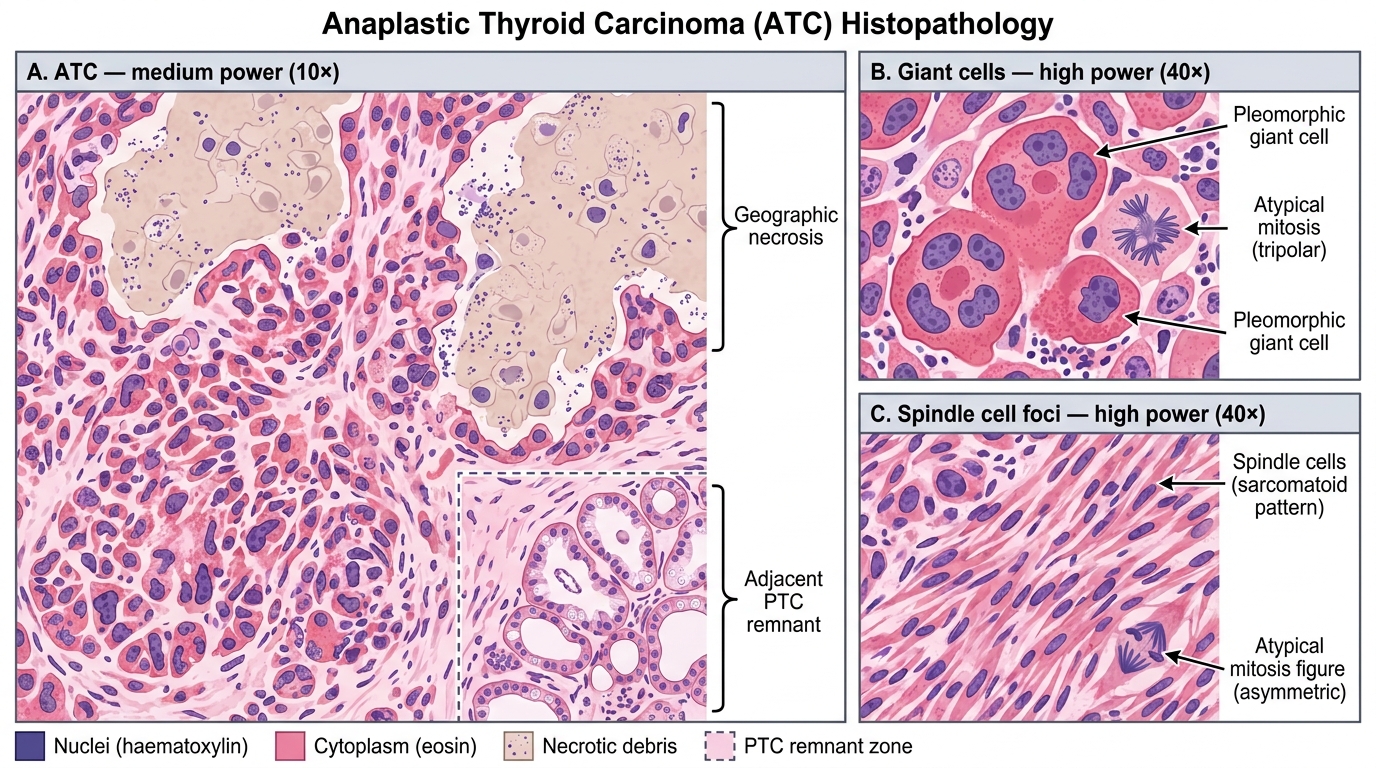
Anaplastic Thyroid Carcinoma — H&E Histology (Medium and High Power)
SELF-CHECK
A 70-year-old man presents with a rapidly enlarging neck mass causing stridor and dysphagia over 4 weeks. FNAC shows markedly pleomorphic cells with bizarre giant cells and abundant mitoses. Immunohistochemistry is negative for thyroglobulin. What is the diagnosis and expected prognosis?
A. Papillary thyroid carcinoma — 20-year survival >95%
B. Anaplastic thyroid carcinoma — median survival 3–6 months
C. Medullary thyroid carcinoma — 10-year survival ~70%
D. Non-Hodgkin lymphoma of thyroid — good response to chemotherapy
Reveal Answer
Answer: B. Anaplastic thyroid carcinoma — median survival 3–6 months
The clinical picture (elderly, rapidly enlarging mass, stridor/dysphagia) combined with the histologic findings (marked pleomorphism, giant cells, necrosis, thyroglobulin-negative IHC) is classic for anaplastic thyroid carcinoma. This is the most aggressive thyroid malignancy with a uniformly poor prognosis, median survival 3–6 months. PTC is thyroglobulin-positive and has excellent prognosis. Lymphoma can look similar but responds well to treatment and stains B-cell markers positive.