Page 8 of 26
PA31.{4,6} | Thyroid Tumors & Parathyroid Disease — SDL Guide (Part 3)
Thyroid Carcinoma Comparison: At a Glance
This table consolidates the four major thyroid carcinomas for examination revision:
| Feature | Papillary (PTC) | Follicular (FTC) | Medullary (MTC) | Anaplastic |
|---|---|---|---|---|
| Frequency | 80–85% | 10–15% | 5–10% | 1–2% |
| Cell of origin | Follicular | Follicular | C cell (parafollicular) | Follicular (dedifferentiated) |
| Age | 20–50 | 40–60 | Variable | >65 |
| Key molecular | BRAF V600E, RET/PTC | RAS, PAX8-PPARG | Germline/somatic RET | TP53, BRAF |
| Histologic hallmark | Orphan-Annie nuclei, psammoma bodies | Capsular/vascular invasion | Amyloid stroma | Pleomorphic giant cells |
| Spread | Lymphatic (cervical nodes) | Hematogenous (lung, bone) | Both | Direct invasion + hematogenous |
| Serum marker | Thyroglobulin (post-op) | Thyroglobulin (post-op) | Calcitonin, CEA | None useful |
| Radioiodine response | Yes (especially differentiated) | Yes | No | No |
| Prognosis | Excellent | Good (minimally invasive) to moderate (widely invasive) | Intermediate | Uniformly fatal |
Memory anchor for spread patterns: "Papillary goes to Lymph nodes; Follicular goes to the Far field (bones/lungs)"
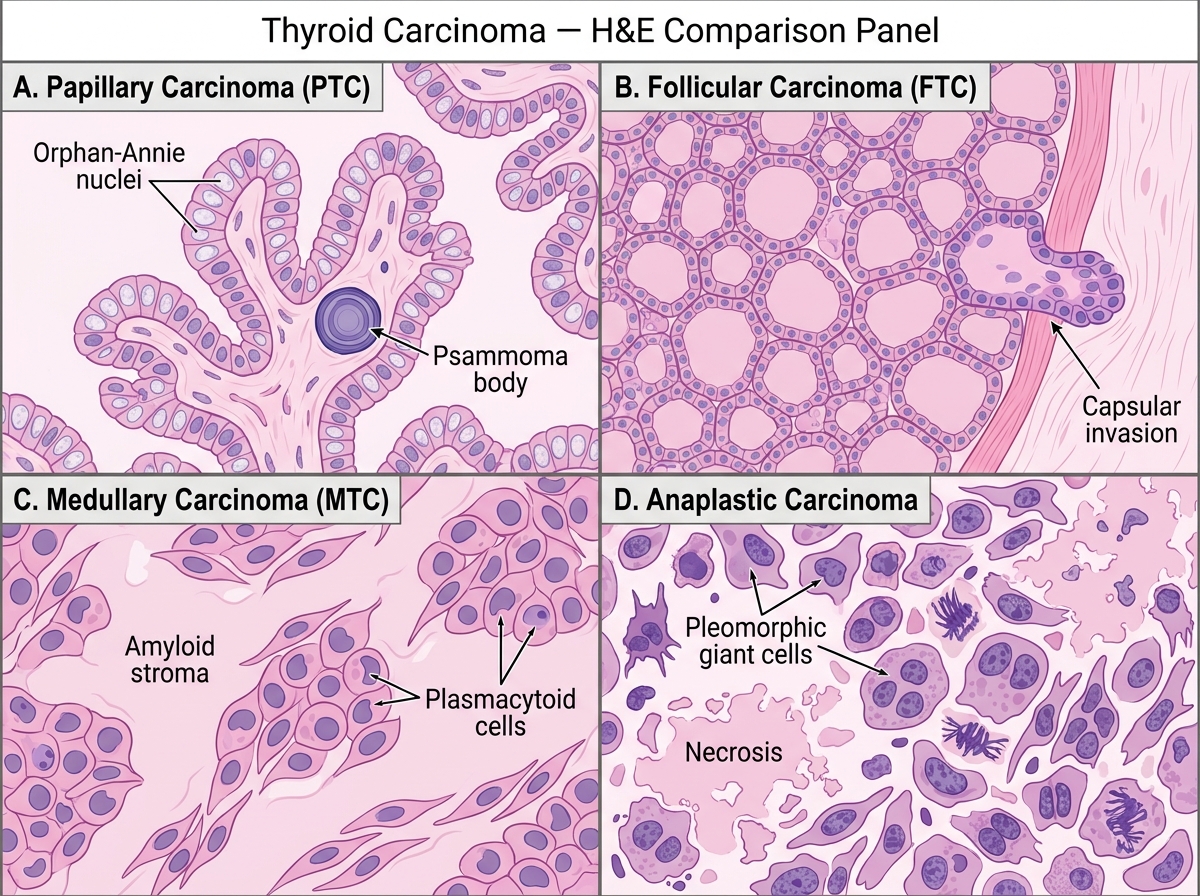
Thyroid Carcinoma — Comparative H&E Histology Panel
Primary Hyperparathyroidism: Pathogenesis and Causes
Hyperparathyroidism is defined as excess secretion of parathyroid hormone (PTH), leading to hypercalcemia and hypophosphatemia.
Classification:
| Type | Mechanism | PTH | Calcium | Cause |
|---|---|---|---|---|
| Primary | Autonomous PTH secretion | ↑↑ | ↑↑ | Parathyroid adenoma (85%), hyperplasia (14%), carcinoma (1%) |
| Secondary | Appropriate PTH ↑ in response to chronic hypocalcemia | ↑↑ | Low or normal | CKD (most common), malabsorption, vitamin D deficiency |
| Tertiary | Secondary → autonomous hyperfunction despite resolved stimulus | ↑↑↑ | ↑↑ | Long-standing secondary hyperparathyroidism (CKD, post-transplant) |
Primary Hyperparathyroidism — Causes in Detail:
- Parathyroid adenoma (85%) — benign neoplasm of a single gland (usually inferior parathyroid). Characteristic rim of normal parathyroid tissue at the periphery (compressed normal gland). Composed predominantly of chief cells (principal cells). No evidence of multiple gland involvement.
- Primary chief cell hyperplasia (14%) — involves all four glands (multiglandular). Associated with MEN1 (MENIN gene, chromosome 11q13) and MEN2A (RET mutation). Asymmetric enlargement of all four glands.
- Parathyroid carcinoma (<1%) — rare, but should be suspected with very high PTH, palpable neck mass, and severe hypercalcemia. Fibrous bands, perineural invasion, and vascular invasion on histology.
Genetics:
- MEN1 (Werner syndrome): Parathyroid hyperplasia + anterior pituitary tumor + pancreatic islet tumor (MENIN tumor suppressor gene)
- MEN2A (Sipple syndrome): MTC + pheochromocytoma + parathyroid hyperplasia (RET proto-oncogene)
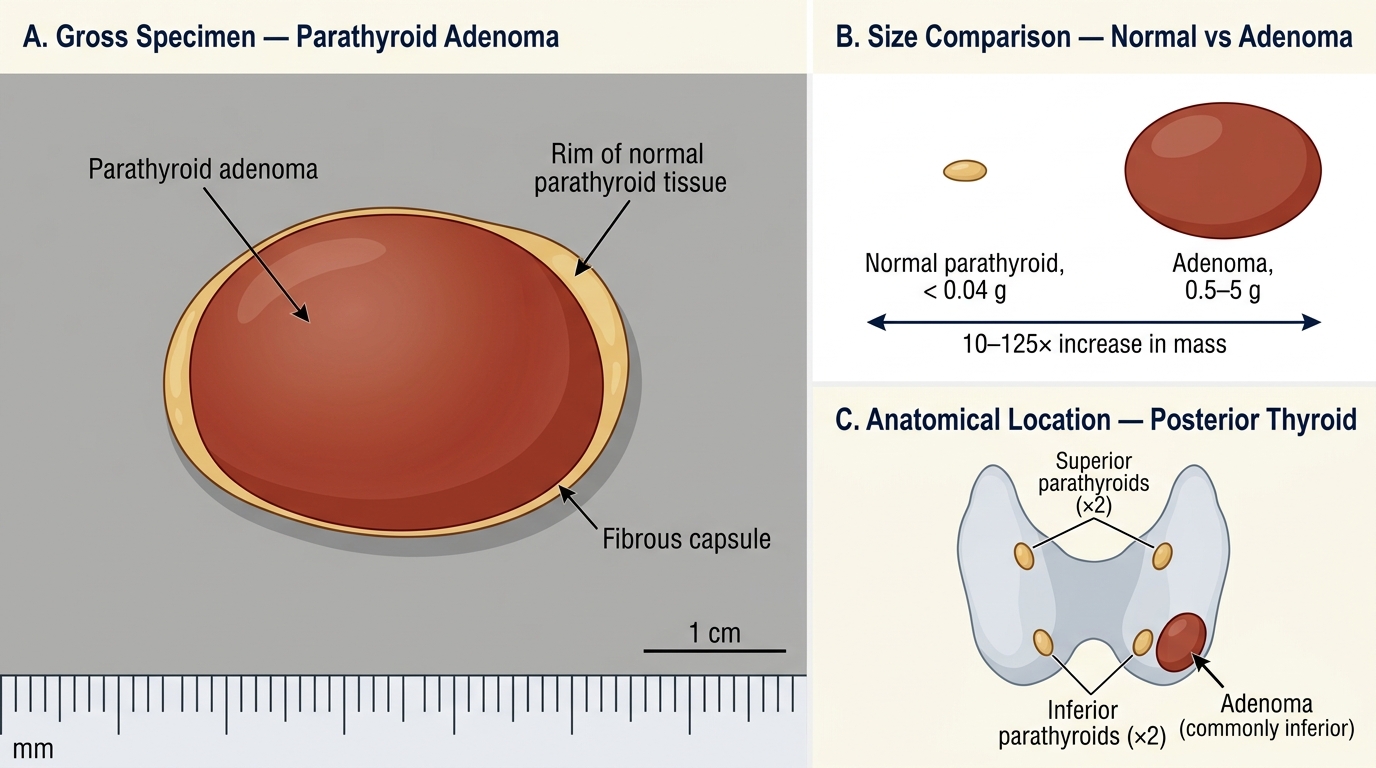
Parathyroid Adenoma — Gross Pathology, Size Comparison, and Anatomical Context
Hyperparathyroidism: Clinical Manifestations and Lab Findings
The clinical manifestations of hyperparathyroidism are best remembered by the classic mnemonic:
"Stones, Bones, Groans, and Psychic Moans"
| Component | Manifestation | Mechanism |
|---|---|---|
| Stones | Renal stones (nephrolithiasis), nephrocalcinosis | Hypercalciuria → calcium oxalate/phosphate stones |
| Bones | Bone pain, pathological fractures, osteitis fibrosa cystica | PTH → osteoclast activation → bone resorption |
| Groans | Nausea, vomiting, constipation, peptic ulcer (via gastrin) | Hypercalcemia → smooth muscle relaxation, gastrin secretion |
| Psychic moans | Depression, anxiety, cognitive impairment, confusion | Hypercalcemia → CNS depression, fatigue |
Additional manifestations:
• Band keratopathy — calcium deposits at lateral corneal margins (slit-lamp finding)
• Hypertension — in ~50% of patients
• Shortened QT interval on ECG — classic electrocardiographic sign of hypercalcemia
• Polyuria/polydipsia — nephrogenic diabetes insipidus (hypercalcemia inhibits ADH action on renal tubule)
Laboratory findings — Primary Hyperparathyroidism:
| Test | Finding | Reasoning |
|---|---|---|
| Serum calcium | ↑↑ | PTH releases bone calcium, increases renal reabsorption |
| Serum phosphate | ↓ | PTH promotes renal phosphate wasting |
| Serum PTH (intact) | ↑ or inappropriately normal | Autonomous secretion (normal PTH in hypercalcemia = inappropriate = abnormal) |
| Urine calcium | ↑ | Overwhelms renal reabsorption |
| Alkaline phosphatase | ↑ | Osteoblastic activity secondary to bone turnover |
| 1,25-(OH)₂ vitamin D | ↑ | PTH activates 1-α-hydroxylase in kidney |
Key distinction: In malignancy-associated hypercalcemia, PTH-related protein (PTHrP) is elevated but intact PTH is suppressed (because the pituitary-parathyroid feedback axis is intact and responds to hypercalcemia).
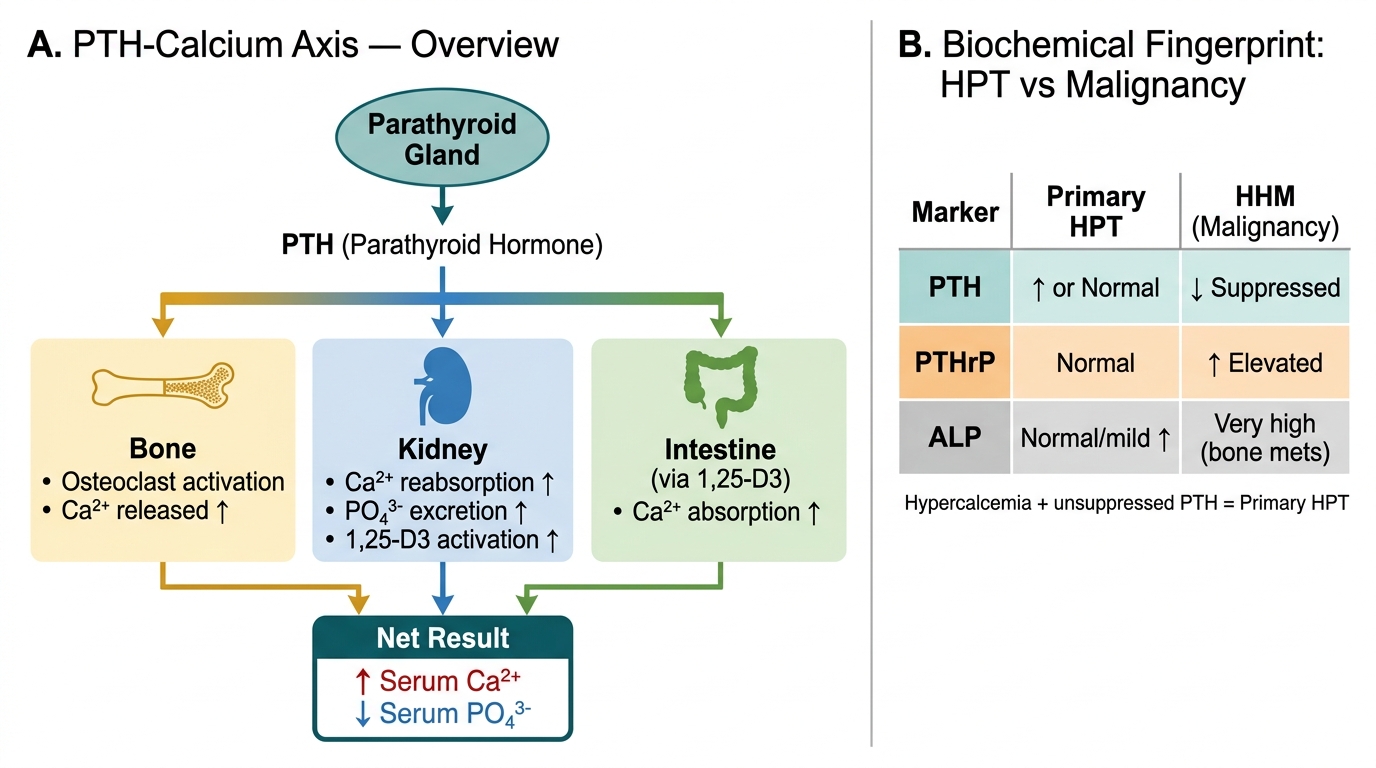
PTH-Calcium Axis and Biochemical Distinction of Hypercalcemia
CLINICAL PEARL
"Asymptomatic" primary hyperparathyroidism is common — and often missed. Today, >80% of primary HPT patients in developed countries are diagnosed incidentally on routine biochemistry before developing stones or bone disease. The finding of hypercalcemia with an unsuppressed (or elevated) PTH is sufficient to diagnose primary hyperparathyroidism — no other test is needed for the biochemical diagnosis.
Urgent distinction — PTH vs. PTHrP:
In an inpatient with hypercalcemia, the first question is: primary HPT or malignancy?
- Primary HPT: PTH ↑, PTHrP normal
- Malignancy (solid tumor): PTH suppressed ↓, PTHrP ↑ (humoral hypercalcemia of malignancy)
- Bone mets: PTH suppressed, PTHrP variable, alkaline phosphatase often very high
This single biochemical distinction guides the entire workup.