Page 9 of 26
PA31.{4,6} | Thyroid Tumors & Parathyroid Disease — SDL Guide (Part 4)
Morphologic Features: Parathyroid Adenoma, Hyperplasia, and Skeletal Changes
Parathyroid Adenoma — Morphology:
- Gross: Solitary, oval, reddish-brown gland, typically 0.5–5 g (normal gland: 35–40 mg). Other glands are normal or atrophic (suppressed by hypercalcemia).
- Microscopic:
- Predominantly chief cells (principal cells) — small polygonal cells with round nuclei, pale eosinophilic cytoplasm; the workhorse PTH-secreting cell
- Rim of compressed normal parathyroid tissue at edge (key feature — absent in carcinoma and hyperplasia)
- Absent fat cells within the adenoma (intracellular fat is lost in hyperfunctioning chief cells)
- May contain water-clear cells or oxyphil cells (non-functional large eosinophilic cells)
Primary Chief Cell Hyperplasia — Morphology:
• All four glands enlarged — asymmetrically
• Diffuse or nodular proliferation of chief cells
• No rim of normal tissue at periphery (distinguishes from adenoma)
• Requires intraoperative assessment of all four glands at surgery
Skeletal changes of hyperparathyroidism:
Osteitis fibrosa cystica (von Recklinghausen disease of bone) — severe, prolonged hyperparathyroidism:
1. Osteoclastic bone resorption — peritrabecular fibrosis, "dissecting osteitis"
2. Brown tumor — localized collections of osteoclasts and reactive giant cells with hemosiderin deposition (hemorrhage → hemosiderin → brown color). Not a true neoplasm — these resolve after parathyroidectomy. May be mistaken for giant cell tumor of bone on X-ray.
3. "Salt and pepper" skull on X-ray — diffuse subperiosteal bone resorption
4. Subperiosteal resorption of radial aspect of middle phalanx — pathognomonic radiologic sign of hyperparathyroidism
5. Rugger jersey spine — alternating dense/lucent bands on vertebrae (in secondary HPT)
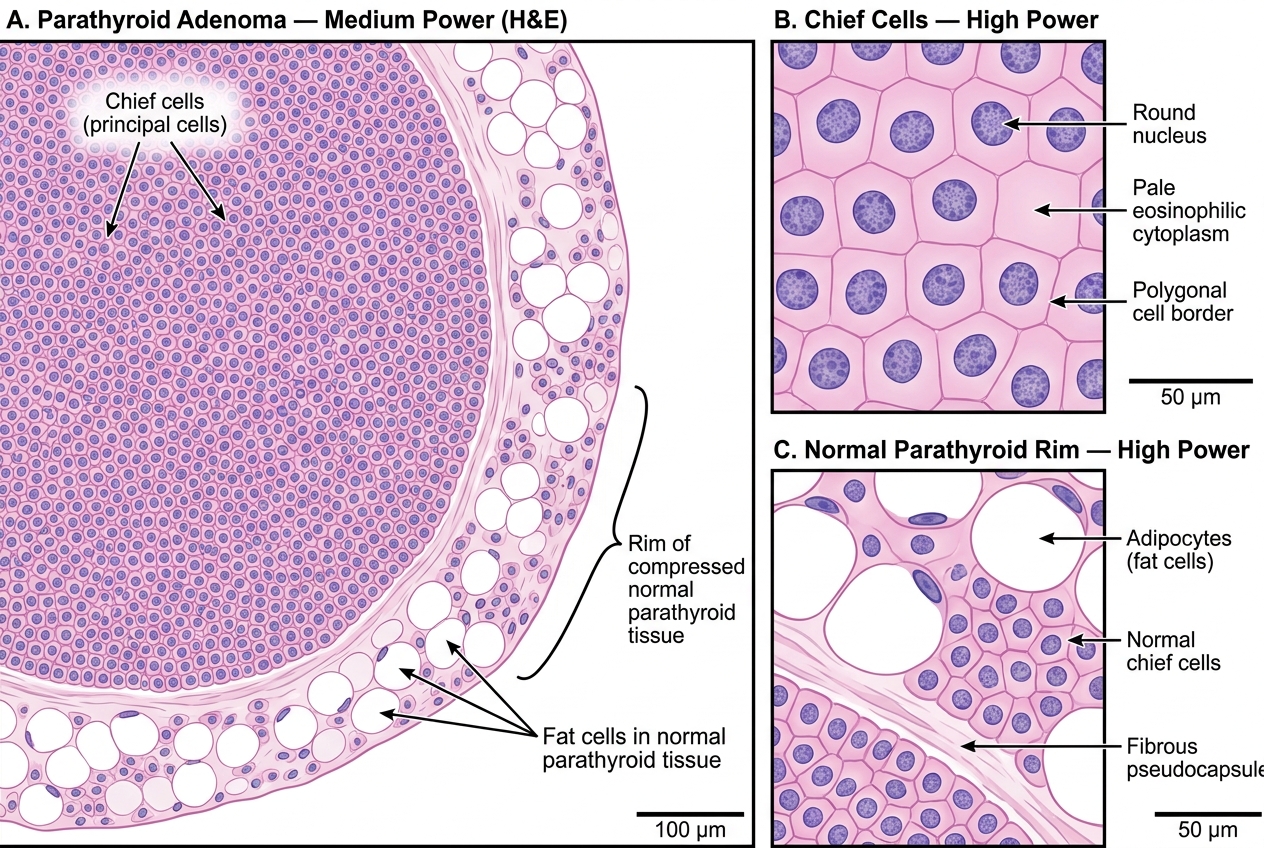
Parathyroid Adenoma: H&E Histology — Chief Cells and Rim of Normal Parathyroid Tissue
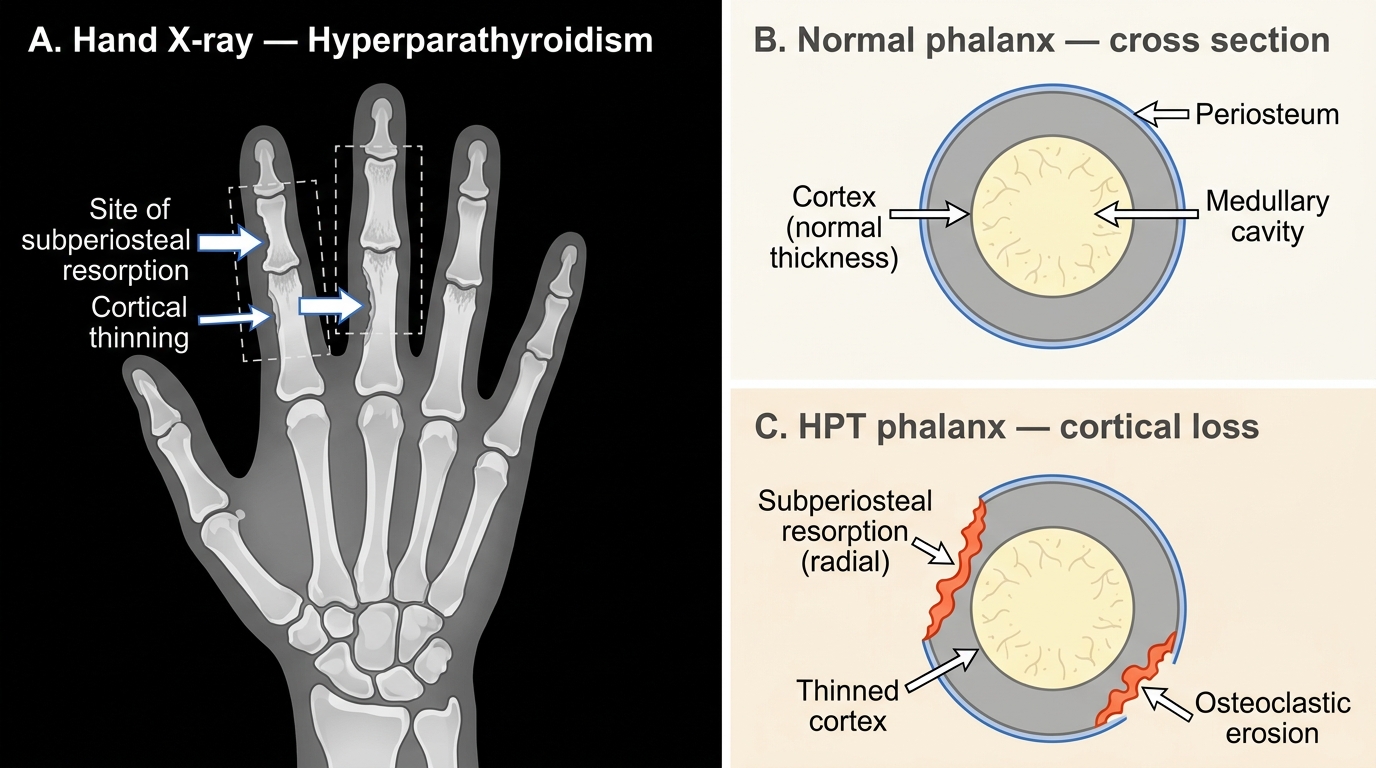
Subperiosteal Bone Resorption in Hyperparathyroidism — Hand X-ray and Phalanx Cross-sections
Secondary and Tertiary Hyperparathyroidism
Secondary Hyperparathyroidism:
• Cause: Chronic kidney disease (CKD) is by far the most common cause in clinical practice
• Mechanism in CKD:
1. ↓ GFR → phosphate retention → ↑ serum phosphate
2. ↑ Phosphate → directly suppresses serum calcium
3. ↓ GFR → ↓ 1-α-hydroxylase → ↓ calcitriol (1,25-D₃) → ↓ intestinal calcium absorption
4. Low calcium + low calcitriol → parathyroid gland stimulation → appropriate ↑ PTH
5. Chronic stimulation → all four glands enlarge (chief cell hyperplasia)
- Lab: Ca²⁺ low or normal, PO₄³⁻ elevated, PTH elevated, calcitriol low — the opposite of primary HPT phosphate pattern
- Treatment: Dietary phosphate restriction, oral calcium + vitamin D supplements, phosphate binders, cinacalcet (calcimimetic that mimics calcium at the parathyroid calcium-sensing receptor)
Tertiary Hyperparathyroidism:
- Mechanism: After prolonged secondary HPT (especially in CKD or post-renal transplant), the hyperplastic parathyroid glands develop autonomous function — they no longer respond to feedback from corrected calcium levels
- Result: Hypercalcemia despite correction of the original stimulus (e.g., after successful renal transplant)
- Histology: Nodular hyperplasia of all four glands → some nodules become clonal (adenoma-like autonomous secretion)
- Treatment: Surgical parathyroidectomy (3.5-gland removal or total with autotransplantation)
Memory scaffold:
- Primary: Problem is in the parathyroid → PTH ↑, Ca ↑, PO₄ ↓
- Secondary: Problem is outside (kidney/gut) → PTH ↑ as compensatory response, Ca low/normal, PO₄ ↑ (in CKD)
- Tertiary: Secondary that escaped feedback → now acts like primary
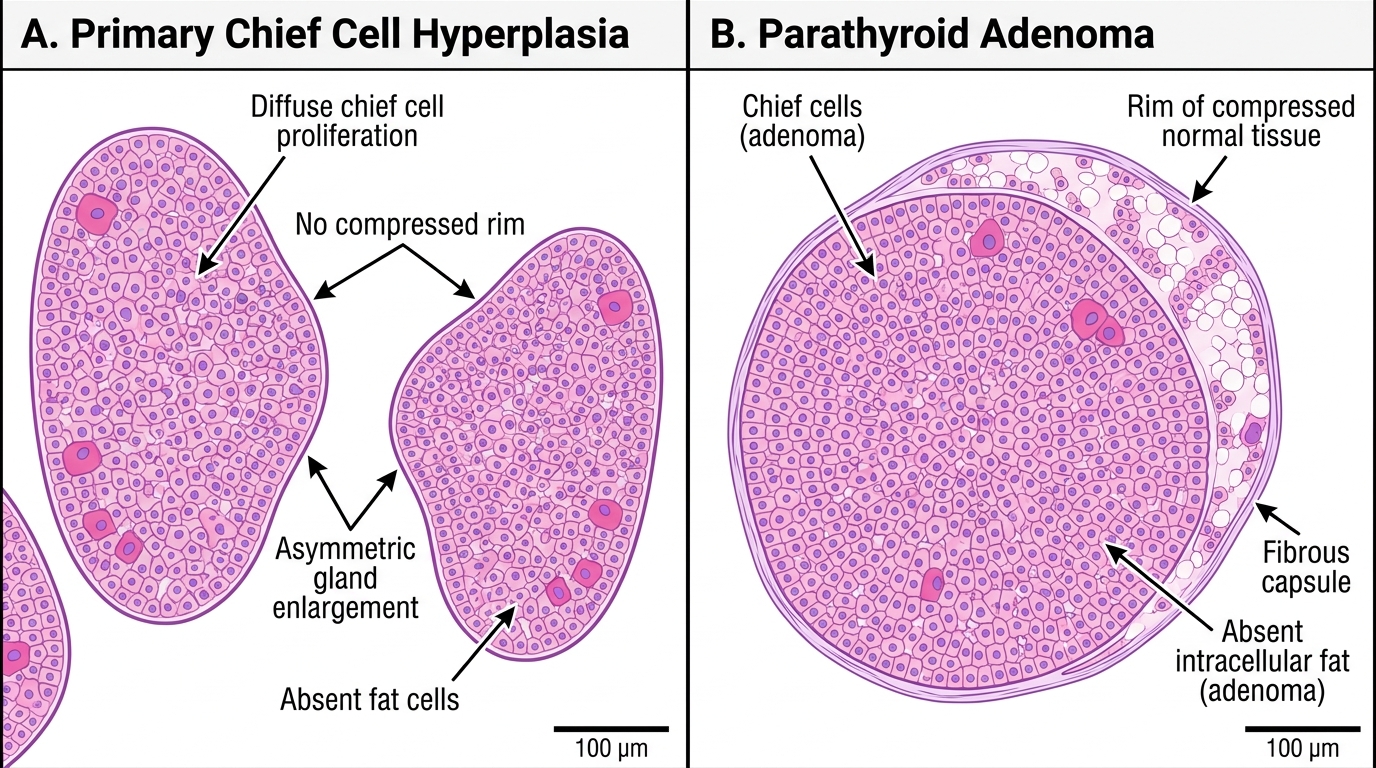
H&E Histology: Parathyroid Chief Cell Hyperplasia vs. Adenoma
SELF-CHECK
A 55-year-old patient with long-standing CKD on hemodialysis is found to have very high PTH, elevated serum phosphate, and normal serum calcium. After receiving a successful renal transplant 6 months ago, she now has hypercalcemia with still-elevated PTH. What is the most likely explanation?
A. Primary hyperparathyroidism due to a new parathyroid adenoma
B. Tertiary hyperparathyroidism — autonomous PTH secretion after prolonged CKD
C. Secondary hyperparathyroidism persisting due to ongoing CKD
D. Malignancy-associated hypercalcemia from PTHrP secretion
Reveal Answer
Answer: B. Tertiary hyperparathyroidism — autonomous PTH secretion after prolonged CKD
This is the classic scenario for tertiary hyperparathyroidism. Long-standing CKD caused secondary HPT (all four glands hyperplastic, appropriately elevated PTH). After successful transplant correcting the original stimulus, the chronically stimulated parathyroid glands have developed autonomous function and continue to secrete PTH despite restored calcium homeostasis — resulting in hypercalcemia. Primary HPT would not have been preceded by CKD-driven secondary disease. Secondary HPT would not produce hypercalcemia. PTHrP would suppress intact PTH.