Page 1 of 23
PA29.6-8 | Cervicitis, Endometriosis & Adenomyosis — SDL Guide
Learning Objectives
- Describe the etiology and morphologic features of acute and chronic cervicitis, including the role of the transformation zone and follicular cervicitis (PA29.6)
- Explain the etiology, hormonal dependence, sites, microscopic features, clinical manifestations, and complications of endometriosis (PA29.7)
- Describe the etiology, morphologic features, and clinical distinctions of adenomyosis, differentiating it from endometriosis and leiomyoma (PA29.8)
INSTRUCTIONS
These three conditions account for a large share of gynecological morbidity in women of reproductive age — from discharge and cervical dysplasia risk to the most common cause of secondary dysmenorrhea and infertility in India. Pathologists report these diagnoses on cervical biopsies, laparoscopic specimens, and hysterectomy slides every day. Understanding the morphology and underlying biology here is not academic box-ticking: it directly shapes how you will interpret histopathology reports, counsel patients, and recognize when a 'simple period pain' needs urgent investigation. Work through each section actively — the micro-quizzes are calibrated to exam and clinical viva level.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 22 — Female Genital Tract (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old married woman presents to the OPD with a 3-year history of progressively worsening lower abdominal pain that peaks 2 days before each period and a failure to conceive despite regular unprotected intercourse for 18 months. On examination, her uterus is retroverted and fixed; movement of the cervix elicits sharp pain (cervical excitation tenderness). Pelvic ultrasound shows a 4 cm left ovarian cyst with low-level internal echoes. Her Pap smear two years ago was reported as 'chronic cervicitis'.
Three separate pathological processes — cervicitis, endometriosis, and adenomyosis — can all announce themselves in a young woman's pelvic pain story, and they can co-exist. By the time you finish this module you will be able to explain exactly what the pathologist sees under the microscope that underpins each diagnosis, and why each condition behaves the way it does.
WHY THIS MATTERS
Why does this matter to you as a second-year MBBS student?
- Prevalence: Chronic cervicitis is the single most common gynecological diagnosis in Pap smear reports. Endometriosis affects ~10% of women of reproductive age worldwide and is the leading surgically-confirmed cause of infertility and chronic pelvic pain in India.
- NMC exam weightage: PA29.6–PA29.8 are consistently asked in university theory and practical exams; endometriosis microscopy is a classic histopathology slide question.
- Clinical bridge: Cervicitis underlies STI management, cervical cancer risk stratification, and the concept of the transformation zone — which you will revisit in the cervical carcinoma module. Endometriosis and adenomyosis are central to the gynecology ward case presentations you will encounter in Year 3.
- Conceptual anchor: All three conditions are governed by a core principle — normal tissue in the wrong context, whether that is inflammation in a sterile site (cervix), ectopic endometrium outside the uterus (endometriosis), or endometrium buried within the muscle wall (adenomyosis).
RECALL
Before we begin, activate your Year-1 knowledge:
The cervix and transformation zone — Recall that the ectocervix is lined by stratified squamous epithelium, while the endocervical canal is lined by columnar (mucus-secreting) epithelium. The transformation zone (T-zone) or squamo-columnar junction is the dynamic interface between these two epithelia. During puberty and pregnancy, eversion of columnar cells (ectropion) exposes them to the acidic vaginal environment, driving squamous metaplasia. This metaplastic zone is biologically active and both inflammation-prone and carcinogen-susceptible.
The endometrium — Recall the two layers: the functionalis (shed during menstruation, hormone-responsive) and the basalis (permanent, regenerative source). The functionalis contains endometrial glands (simple tubular, lined by columnar epithelium) embedded in a vascular stroma of spindle-shaped cells.
The myometrium — The thick smooth muscle wall of the uterus. Under normal circumstances the endomyometrial junction is sharp; glands do not penetrate into the muscle.
Acute Cervicitis: Etiology and Pathogenesis
Cervicitis is inflammation of the cervix. Acute cervicitis is less common in practice but important to recognise because its causes overlap with sexually transmitted infections (STIs).
Etiology of acute cervicitis:
- Neisseria gonorrhoeae — Gram-negative diplococcus; causes purulent endocervicitis; the columnar epithelium of the endocervical canal is the primary target (squamous epithelium is relatively resistant).
- Chlamydia trachomatis (serovars D–K) — Most common STI-related cause of cervicitis globally and in India. Obligate intracellular bacterium; produces a mucopurulent discharge and, characteristically, follicular cervicitis (lymphoid follicles in the subepithelial stroma).
- Herpes simplex virus type 2 (HSV-2) — causes vesicles and ulceration; Tzanck smear shows multinucleated giant cells.
- Trichomonas vaginalis — protozoon; produces a frothy, malodorous discharge; strawberry cervix on colposcopy.
- Non-infectious causes: Chemical irritants (douches, contraceptive creams, pessaries), foreign bodies (IUDs, forgotten tampons), post-partum lacerations.
Morphology — acute cervicitis:
• Grossly: congested, edematous cervix with mucopurulent discharge from the os.
• Microscopically: neutrophilic infiltrate in the cervical epithelium and stroma; epithelial erosion may be seen; goblet-cell mucus production disrupted.
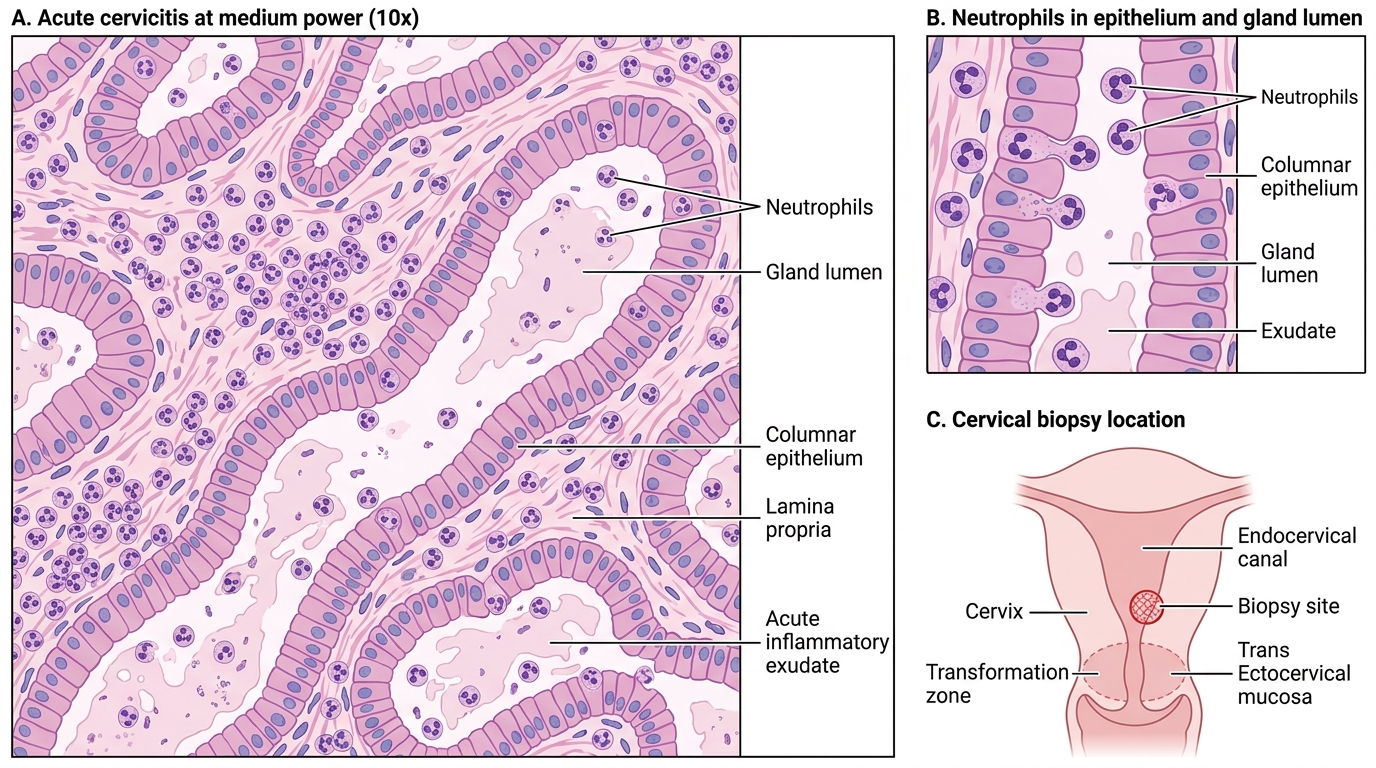
Acute Cervicitis: Cervical Biopsy at 10x
Chronic Cervicitis and Follicular Cervicitis
Chronic cervicitis is by far the more common clinical and histopathological entity. It is almost universal in parous women and in women of reproductive age attending gynecology clinics.
Etiology:
• Normal vaginal flora (lactobacilli, anaerobes) in the context of cervical lacerations, ectropion, or IUD use.
• Persistent low-grade STI (Chlamydia is the classic cause of the follicular variant).
• Post-partum, post-abortion trauma.
• In many women no specific organism is identified — the inflammation is a response to the microbiologically normal but mechanically traumatized transformation zone.
Morphology — chronic cervicitis:
Grossly: Cervix may appear erythematous, granular, or show a mucopurulent or mucoid discharge. Nabothian cysts (retention cysts of obstructed endocervical glands) may be seen as yellowish domes on the ectocervix.
Microscopically:
• Lymphoplasmacytic infiltrate dominates (lymphocytes, plasma cells, occasional macrophages).
• Glandular hyperplasia and mucus retention (Nabothian cysts).
• Reactive squamous metaplasia in the transformation zone.
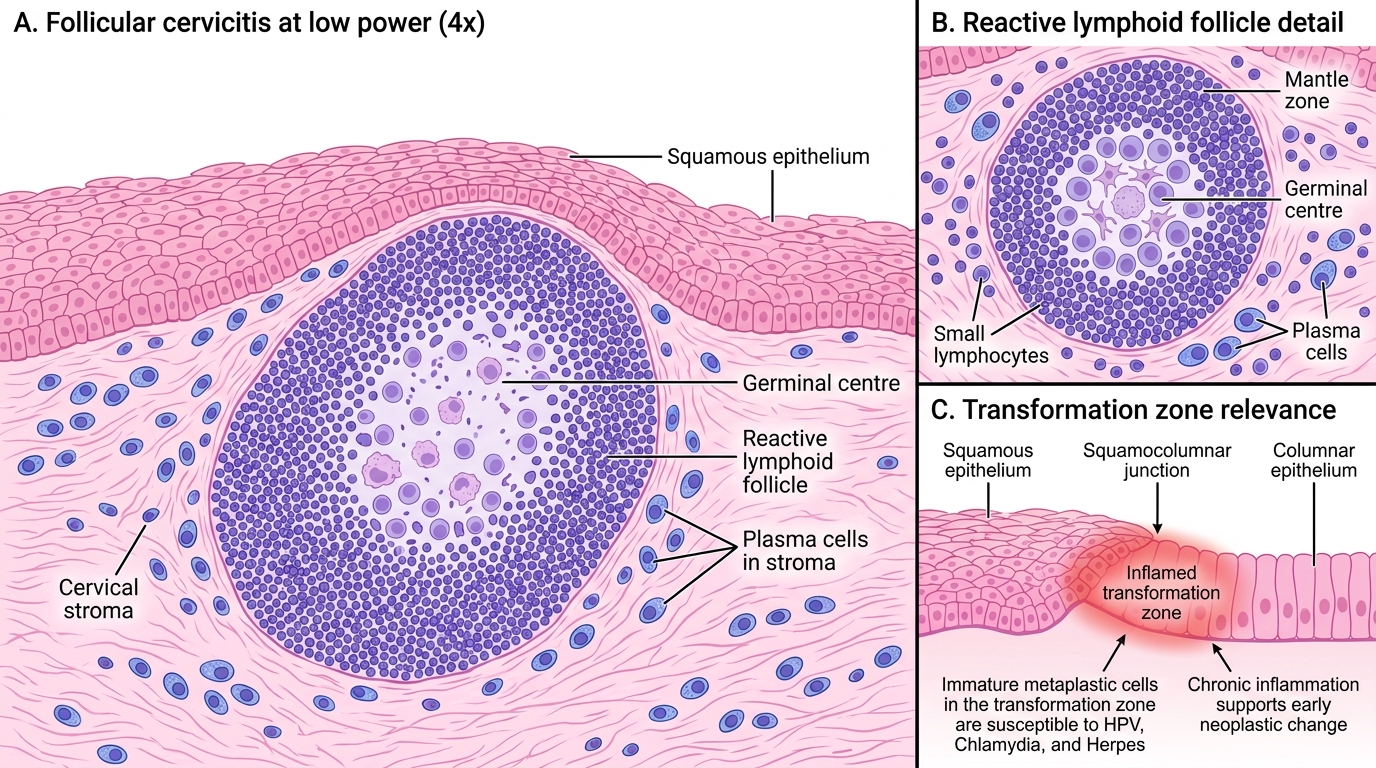
Follicular cervicitis — a distinctive subtype:
• Lymphoid follicles with germinal centers are present in the cervical stroma (reactive lymphoid aggregates — resembling tonsil-like tissue).
• Strongly associated with Chlamydia trachomatis infection.
• The follicles can disrupt the overlying epithelium and create a cobblestone appearance on colposcopy.
Follicular Cervicitis and the Transformation Zone
Cervicitis and the Transformation Zone
Understanding why the transformation zone matters is essential for linking cervicitis to the cervical dysplasia and carcinoma you will study in the next module.
The T-zone and susceptibility:
• Squamous metaplasia in the T-zone produces cells that are biologically immature and transiently lack the full protective glycogen coat of mature squamous cells.
• These immature metaplastic cells are preferentially infected by HPV, Chlamydia, and Herpes — explaining why the T-zone is the site of origin for cervical intraepithelial neoplasia (CIN) and invasive squamous carcinoma.
• Chronic cervicitis in the T-zone sustains a pro-inflammatory microenvironment (cytokines, reactive oxygen species, NF-κB signaling) that is permissive to viral integration and early neoplastic change.
Clinical–pathological correlation:
| Feature | Acute Cervicitis | Chronic Cervicitis |
|---|---|---|
| Dominant infiltrate | Neutrophils | Lymphocytes, plasma cells |
| Discharge | Purulent, mucopurulent | Mucoid or mucopurulent |
| Common cause | N. gonorrhoeae, HSV | Chlamydia, normal flora, IUD |
| Nabothian cysts | Absent | Often present |
| Follicular variant | No | Yes (Chlamydia) |
| Cancer risk link | Indirect (HPV co-infection) | Yes — via T-zone inflammation |
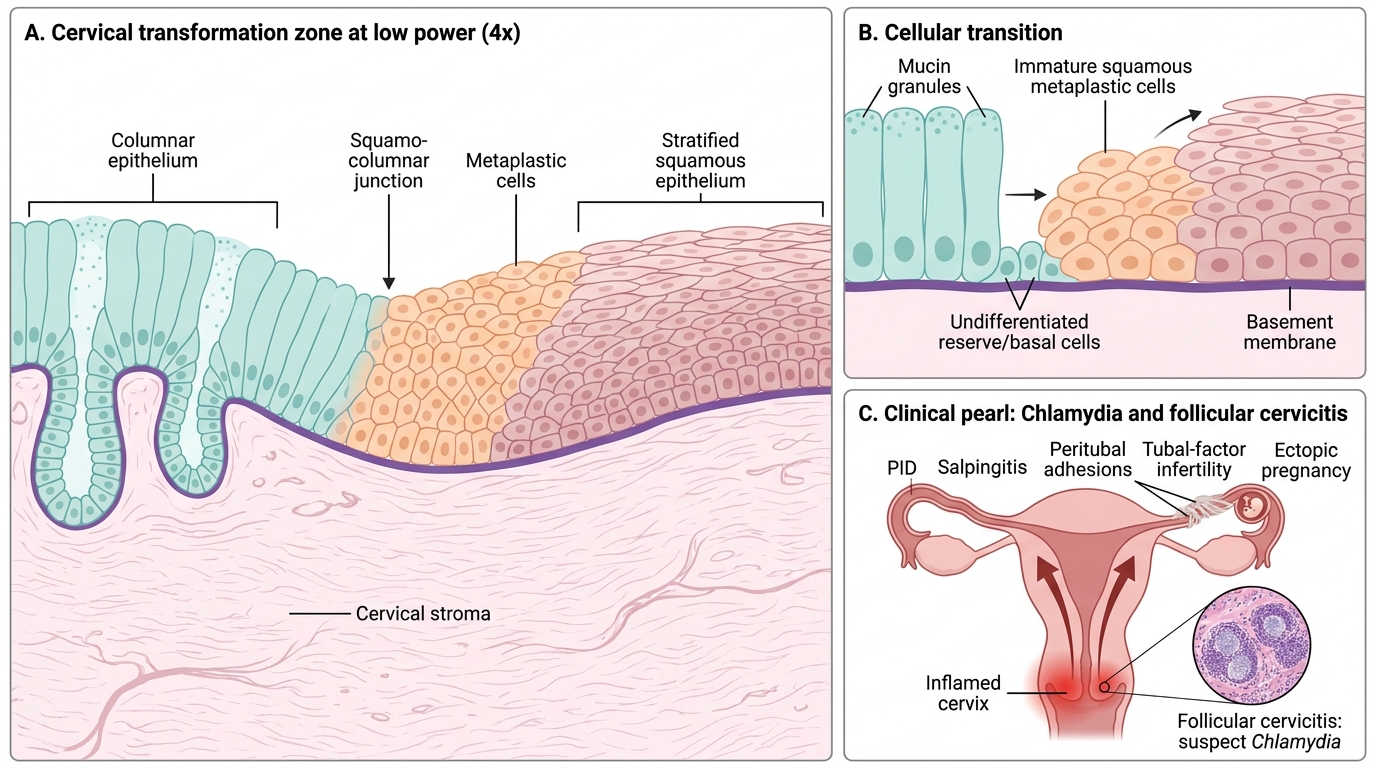
Cervical Transformation Zone with Squamous Metaplasia
CLINICAL PEARL
Pearl: Chlamydia is the 'silent' destroyer of the female pelvis.
Chlamydia trachomatis cervicitis is asymptomatic in up to 70% of infected women. Untreated, it ascends to the endometrium and fallopian tubes, causing pelvic inflammatory disease (PID), salpingitis, and peritubal adhesions — the leading cause of tubal-factor infertility and ectopic pregnancy in young women. The follicular cervicitis pattern on biopsy is your histological cue to suspect Chlamydia even in the absence of purulent discharge. When you see 'follicular cervicitis' in a histopathology report, think Chlamydia first.